All of James Snowden🔸's Comments + Replies
Hi Wayne, that’s fair. I hadn’t been including farmed animal welfare in the comparison because I don’t think people donating to therapy organizations are doing it for animal welfare reasons.
I don’t think it would be practical for givewell to include animal welfare in its evaluations. I think donors who care about both animal and human welfare would have more impact giving to separate projects optimising for each of those goals
Nice post Joey, thanks for laying it out so clearly.
I agree with almost all of this. I find it interesting to think more about which domains / dimensions I'd prefer to push towards prioritization vs. pluralism:
- Speaking loosely, I think EA could push more towards pluralism for career decisions (where personal fit, talent absorbency and specialization are important), and FAW/GHD/GCR cause prioritization (where I at least feel swamped by uncertainty). But I'm pretty unsure on where to shift on the margin in other domains like GiveWell style GHD direct deliver
Hi, James! When it comes to assessing bednets vs therapy or more generally, saving a life vs happiness improvements for people, the meat eater problem looms large for me. This immediately complicates the trade-off, but I don't think dismissing it is justifiable on most moral theories given our current understanding that farm animals are likely conscious, feel pain, and thus deserve moral consideration. Once we include this second-order consideration, it's hard to know the magnitude of the impact given animal consumption, income, economic growth, wild anima...
Hi Midtermist, I think this is a pretty important worry and appreciate you sharing your perspective.
Just speaking for myself and the EA (global health and wellbeing) program I work on (though it’s mostly led by Mel Basnak now).
Here are a few things we’re doing:
- We fund Probably Good, who try to empower people to think along impact-focused lines while remaining open-minded about how different people can best help others.
- We support orgs like Founders Pledge and Charity Entrepreneurship, who share our core values but who do their own research and might have di
Yes, I think that’s mostly fair.
Air pollution in South Asia has a lot of different sources requiring distinct policy interventions, and often at local levels. Eliminating emissions entirely from any one source category would address a relatively small fraction (5%-10%, say) of the problem in a given city or state.
Some interventions that are relatively scalable across India, and likely to be effective are politically intractable: power plant emission controls (expensive and with costs borne by a small group of influential firms), or subsidies to make cleane...
Thanks ajyl! I think the biggest takeaway for me is that you can do a bit of storytelling without compromising on rigor / honesty.
- The ITN framework is compelling and appeals to people outside EA.
- Jenna Forsyth's work in Bangladesh really resonated with people. Combining that story with an estimate of 20,000 lives saved seemed to hit home for a lot of folks.
- Comparison is helpful. Lead exposure is estimated to kill 1.5 million people but receives only $15m in funding is compelling to people who can put those numbers in perspective. But lead exposure is estima
Thanks Rafael! A few theories:
- There just aren’t many people whose job it is to look for important, tractable and neglected causes. It’s striking how much of the recent upsurge in interest has been related to EA.
- While there are some individual cases of very severe exposure, most of the burden is caused by relatively small risks of harm spread across entire populations, so victims aren’t identifiable.
- A lot of global health funding is allocated by disease category. Lead exposure cuts across disease categories, so it just doesn’t naturally fit into a lot of fu
The most direct focus of LEAF’s source-specific mitigation work is paint and spices, but that’s largely because of tractability: these are both products where there are only weak economic incentives to use lead, and where production is fairly consolidated. That makes them easier to regulate. For other sources (batteries, cookware, cosmetics etc.), we want to fund more exploratory work: piloting and testing regulatory interventions rather than scaling them.
I think figuring out what to do on informal ULAB recycling is really important. ~80% of global lead is...
Thanks Parth, I appreciate it and thank you for your support along the way!
How did you first learn about lead as an issue? I know you were looking into public health regulation broadly at that time (e.g. pesticides) and in your conversation notes from 2017 you cite various statistics (e.g. WHO statistic that 10% of children globally have >20 micrograms of lead NYU study on $1 trillion of economic costs). What first rang the alarm bells for you that this was an area worth investigating?
IIRC, I first learned about it as a development issue from some...
Open Phil’s main role was organizing a group of donors to commit most of the funding which was announced alongside the Partnership for a Lead-Free Future. The Lead Exposure Action Fund comprises $104m of the $150m that was announced, and Open Phil staff will manage the allocation of those funds. The work to launch a collaborative fund was quite far along when we formalized a partnership with USAID, so it’s an interesting coming together of two strands.
We’ve also been working very closely with USAID and UNICEF to help design the PLF (and we’re still working...
Thanks Nick, that’s very kind of you to say. I’ve also really appreciated your contributions to the forum.
Yes! I’ve updated on how quickly smart and driven people can build networks and expertise to make an impact on policy, especially in neglected areas.
I do think lead exposure (and particularly paint) was a wise choice for LEEP’s founders who were starting out with less previous policy experience. It’s a fairly technocratic regulatory intervention without much opposition, the area’s neglected so it’s easier to build your network, and there are already model laws and various international agreements in place. And I also think LEEP’s team is unusually ca...
Yes! Giving What We Can is how I first got involved with effective altruism, and I’ve given at least 10% of my income since graduating. This year, I gave to the Lead Exposure Elimination Project, Effektiv Spenden, and the GiveWell All Grants Fund. I think they’re all awesome organizations, and I feel confident in personally standing behind them, given how well I know their work.
In 2017, I split my donation across cause areas and part of the reason was to signal that I believed in the importance of GCR and animal welfare work. I also thought giving might mo...
We're limiting ourselves to a fraction of GWWC's funding. At the moment, that's in the region of 70%, but GWWC and OP are aligned that we expect to dial it down substantially over time, both to enable a more diverse funding base for GWWC and to free up programmatic budget for other organizations.
Fwiw I disagree that OP's bar is 2x the cost-effectiveness of GiveWell's top charities in practice. In my view (not an official OP position or anything) differences in modeled cost-effectiveness between GW and OP's bar are indistinguishable from noise.
Hi Evan, thank you for the kind words!
I wanted to clarify one point:
>It could exceed the value of all the money that has ever flowed through EA to any charity GiveWell has ever recommended.
LEAF and the Partnership for a Lead-Free Future wouldn't have happened without GiveWell. They were the first major funder in the EA space to recommend grants for lead exposure, and much of the recent progress comes from those early investments, such as grants to Pure Earth and CGD. I also believe (though I’m less certain) that Charity Entrepreneurship’s recommendation...
You might find this article helpful for context: https://undark.org/2023/07/19/the-vice-of-spice-confronting-lead-tainted-turmeric/
Fwiw I’m sympathetic to your general point
Implicitly, yes. Though don’t use that exact formulation. money vs daly comparison is based on reported preference not swb. Daly vs swb comparison implicitly writes off time spent asleep where I assumed 1 daly = difference between 40->100 on swb scale.
If didn’t exclude sleep in botec, would make alcohol look worse as happiness bump from alcohol would be for lower % of time. (Set row 21 to 24)
>Another thought - you measure the effects of alcohol on subjective wellbeing as a fraction of someone's waking hours. This seems right from a subjective wellbeing perspective. But is that also the way you think about the value lost by a death? By consistency, you would also need to implicitly downweight the disvalue a death by a third for the time people spend asleep. Or do you already do that in your moral weights?
Oh that's interesting. It's been a while now since I did this, but I think I was implicitly doing that with this calc
>I'm not sure I follow the claim that if you assume that alcohol taxation merely shifts the tax burden, there aren't strong reasons to think the deadweight loss will be greater from alcohol taxation vs other forms of taxation. The subjective wellbeing study found that drinking increases people's wellbeing by almost as much as spending time with friends. It seems unlikely to me that if the tax were instead eg on income that the benefits of the income would be as large as this. Intuitively, this seems off.
Interesting. That doesn't seem off to me. If...
Hi Nick, thanks for your thoughts.
I agree air quality is meaningfully different from the other areas we highlight in terms of domestic salience (at least in India). But it’s not clear to me whether the existence of nascent government funding (and the consequent opportunity to improve the allocation of that funding) make philanthropic opportunities better or worse.
Efforts like the NCAP framework and 15th Finance Commission budget allocations in India are fairly new, and there aren’t well-developed playbooks for prioritizing and addressing sources of air pol...
Thanks Barry,
At GiveWell (where I was working when we started the suicide prevention work), we discounted the impact to account for people who would otherwise die by suicide potentially living somewhat worse lives than a typical person in their context. Given the empirical and moral uncertainty, that estimate was based on a deliberative process and preference aggregation of different staff views rather than a single bottom-up model. Open Phil hasn't yet decided whether to incorporate a similar discount.
An overview of how GiveWell thought about it is ...
Thanks for the thoughts Kartik!
(Speaking for myself; the 10% estimate comes from work I did at GiveWell but others at Open Phil and GiveWell may disagree with me)
I agree we shouldn’t dismiss consumer surplus entirely, and in retrospect would soften some of the wording in that doc – I think the irrationality point is important but not totalizing. The Nielsen idea is interesting and I’d like to think about it more. I think internalities are less bimodally distributed between people than your model, which muddies the waters, but I wonder if an analysis like t...
>Since then, all the major actors in effective altruism’s global health and wellbeing space seem to have come around to it (e.g., see these comments by GiveWell, Founders Pledge, Charity Entrepreneurship, GWWC, James Snowden).
I don't think this is an accurate representation of the post linked to under my name, which was largely critical.
Hello James. Apologies, I've removed your name from the list.
To explain why we included it, although the thrust of your post was to critically engage with our research, the paragraph was about the use of the SWB approach for evaluating impact, which I believed you were on board with. In this sense, I put you in the same category as GiveWell: not disagreeing about the general approach, but disagreeing about the numbers you get when you use it.
[Speaking for myself here]
I also thought this claim by HLI was misleading. I clicked several of the links and don't think James is the only person being misrepresented. I also don't think this is all the "major actors in EA's GHW space" - TLYCS, for example, meet reasonable definitions of "major" but their methodology makes no mention of wellbys
Thanks Jason, mostly agree with paras 4-5, and think para 2 is a good point as well.
Do you think the neutral point and basic philosophical perspective (e.g., deprivationism vs. epicureanism) are empirical questions, or are they matters on which the donor has to exercise their own moral and philosophical judgment (after considering what the somewhat limited survey data have to say on the topic)?
I think the basic philosophical perspective is a moral/philosophical judgement. But the neutral point combines that moral judgement with empirical models...
From HLI's perspective, it makes sense to describe how the moral/philosophical views one assumes affect the relative effectiveness of charities. They are, after all, a charity recommender, and donors are their "clients" in a sense. GiveWell doesn't really do this, which makes sense -- GiveWell's moral weights are so weighted toward saving lives that it doesn't really make sense for them to investigate charities with other modes of action. I think it's fine to provide a bottom-line recommendation on whatever moral/philosophical view a recommender feels is b...
Sure, happy to elaborate.
Here's figure 4 for reference:
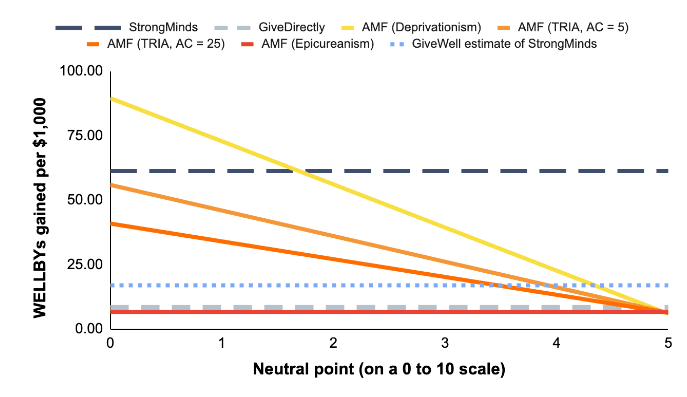
I think each part of this chart has some assumptions I don't think are defensible.
1. I don't think a neutral point higher than 2 is defensible.
You cite three studies in this report.[1] My read on what to conclude about the neutral point from those is:
i) IDinsight 2019 (n=70; representative of GW recipients): you highlight the average answer of 0.56, but this is excluding the 1/3 of people who say it's not possible to have a life worse than death.[2] I think including those as 0 mor...
On 3. Epicureanism being a defensible position
Epicureanism is discussed in almost every philosophy course on the badness of death. It’s taken seriously, rather than treated as an absurd position, a non-starter, and whilst not that many philosophers end up as Epicureans, I’ve met some that are very sympathetic. I find critics dismiss the view too quickly and I’ve not seen anything that’s convinced me the view has no merit. I don’t think we should have zero credence in it, and it seems reasonable to point out that it is one of the options. Again, I’m incline...
Hi James, thanks for elaborating, that’s really useful! We'll reply to your points in separate comments.
Your statement, 1. I don't think a neutral point higher than 2 is defensible
Reply: I don’t think we have enough evidence or theory to be confident about where to put the neutral point.
Your response about where to put the neutral point involves taking answers to survey questions where people are asked something like “where on a 0-10 scale would you choose not to keep living?” and assuming we should take those answers at face value for where to ...
Do you think the neutral point and basic philosophical perspective (e.g., deprivationism vs. epicureanism) are empirical questions, or are they matters on which the donor has to exercise their own moral and philosophical judgment (after considering what the somewhat limited survey data have to say on the topic)?
I would graph the neutral point from 0 to 3. I think very few donors would set the neutral point above 3, and I'd start with the presumption that the most balanced way to present the chart is probably to center it fairly near the best guess fr...
I think I’m more skeptical than you that reasonable alternative assumptions make StrongMinds look more cost effective than AMF. But I agree that StrongMinds seems like it could be a good fit for some donors.
Interested if you could elaborate here. I'm not sure which intuitions you consider 'reasonable' and why. As Joel's figure 4 above indicates, for either HLI's or GiveWell's estimates of StrongMinds, talk therapy can be more cost-effective than bednets, and vice versa, but which is more effective depends on the philosophical assumptions - so that ou...
FWIW I don't think GiveDirectly should be "the bar" for being considered one of the most effective organizations in the global health and development space.
I think both 5x and 10x differences are big and meaningful in this domain, and I think there are likely billions of dollars in funding gaps between GiveWell's bar (~10x) and GiveDirectly. I think donors motivated by EA principles would be making a mistake, and leaving a lot of value on the table by donating to GiveDirectly or StrongMinds over GiveWell's recommendations (I say this as someone who's donat...
Fair points. I'm not planning to move my giving to GiveWell All Grants to either SM or GD, and don't mean to suggest anyone else does so either. Nor do I want to suggest we should promote all organizations over an arbitrary bar without giving potential donors any idea about how we would rank within the class of organizations that clear that bar despite meaningful differences.
I mainly wrote the comment because I think the temperature in other threads about SM has occasionally gotten a few degrees warmer than I think optimally conducive to what we're trying ...
Thanks, this looks like a helpful report!
It looks like this estimate comes from the proportion of countries the Bloomberg consortium and World Bank worked in that passed various policies over a decade without adjusting for the counterfactual chance of policy changes without their work.
I’m curious if CE had any luck trying to estimate the counterfactual (Eg by looking at other countries, trends before BB, or diving deep on individual case studies)?
Fwiw when I looked at this a few years ago (at GiveWell, not OP) I couldn’t find any evidence of a difference i...
(I work at Open Phil on Effective Altruism Community Building: Global Health and Wellbeing)
Our understanding is that only a small proportion of FTXFF’s grantees would be properly classified as global health or animal welfare. Among that subset, there are some grantees who we think might be a good fit for our current focus areas and strategies. We’ve reached out individually to grantees we know of who fit that description
That being said, it’s possible we’ve missed potential grantees, or work that might contribute across multiple cause areas. If you think that might apply to your project, you can apply through the same form.
On (1)
>people inflate their self-reports scores generally when they are being given treatment?
Yup, that's what I meant.
>Is there one or more studies you can point me to so I can read up on this, or is this a hypothetical concern?
I'm afraid I don't know this literature on blinding very well but a couple of pointers:
(i) StrongMinds notes "social desirability bias" as a major limitation of their Phase Two impact evaluation, and suggest collecting objective measures to supplement their analysis:
"Develop the means to negate ...
Excited to see your work progressing Michael!
I thought it might be useful to highlight a couple of questions I personally find interesting and didn't see on your research agenda. I don't think these are the most important questions, but I haven't seen them discussed before and they seem relevant to your work.
Writing this quickly so sorry if any of it's unclear. Not necessarily expecting an answer in the short term; just wanted to flag the questions.
(1) How should self-reporting bias affect our best guess of the effect size of therapy-ba...
I would deprioritise looking at BasicNeeds (in favour of StrongMinds). They use a franchised model and aren't able to provide financials for all their franchisees. This makes it very difficult to estimate cost-effectiveness for the organisation as a whole.
The GWWC research page is out of date (it was written before StrongMinds' internal RCT was released) and I would now recommend StrongMinds above BasicNeeds on the basis of greater levels of transparency, and focus on cost-effectiveness.
Thanks Holden. This seems reasonable.
A high impact foundation recently (and helpfully) sent me their grant writeups, which are a treasure trove of useful information. I asked them if I could post them here and was (perhaps naively) surprised that they declined.
They made many of the same points as you re: the limited usefulness of broad feedback, potential reputation damage, and (given their small staff size) cost of responding. Instead, they share their writeups with a select group of likeminded foundations.
I still think it would be much better if they mad...
It seems like you're assuming that the GiveDirectly money would have gone only to the M-Pesa-access side of the (natural) experiment, but they categorized areas based on whether they had M-Pesa access in 2008-2010, not 2012-2014 when access was much higher.
Ah yes - that kind of invalidates what I was trying to do here.
I didn't notice that GiveWell had an estimate for this, and checking now I still don't see it. Where's this estimate from?
It came from the old GiveWell cost-effectiveness analysis excel sheet (2015). "Medians - cell V14". Act...
Thanks for this Jeff - a very informative post.
The study doesn't appear to control for cash transfers received through access to M-Pesa. I was thinking about how much of the 0.012 increase in ln(consumption) was due to GiveDirectly cash transfers.
Back of the envelope:
- M-Pesa access raises ln(consumption) by 0.012 for 45% of population (c.20m people).
0.012 * 20m = 234,000 unit increases in ln(consumption)
GiveDirectly gave c.$9.5m in cash transfers between 2012-14 to people with access to M-Pesa. [1]
- GiveWell estimate each $ to GiveDirectly raises ln(c
I agree that dmu over crop yields is perfectly rational. I mean a slightly different thing. Risk aversion over utilities. Which is why people fail the Allais pradadox. Rational choice theory is dominated by expected utility theory (exceptions Buchak, McClennen) which suggests risk aversion over utilities is irrational. Risk aversion over utilities seems pertinent here because most moral views don't have dmu of people's lives.
In normative decision theory, risk aversion means a very specific thing. It means using a different aggregating function from expected utility maximisation to combine the value of disjunctive states.
Rather than multiplying the realised utility in each state by the probability of that state occurring, these models apply a non-linear weighting to each of the states which depends on the global properties of the lottery, not just what happens in that state.
Most philosophers and economists agree risk aversion over utilities is irrational because it violates the...
Thanks Austen. This is really helpful feedback.
Yes I agree. This is important but very hard to quantify. Of course the causal relationship goes both ways (poor physical health poor mental health) but it's probable that mental health disorders have worse downstream effects than most physical health problems (economic productivity, stigma, impact on carers, physical health). We tried to capture these qualitatively at the beginning of the report but could have been clearer that they weren't included in the cost-effectiveness calculations.
Thanks - this is
Eric - this is so great! Coincidentally, CEA has also been working on a very similar report which was completed last week. It's here: https://drive.google.com/open?id=0B551Ijx9v_RoZWlUUFVTYWZ6aTVCUDRDLTViVHVyQVpPWVNn
I've shot you an email. We should definitely discuss our conclusions.
Any thoughts on the impact multiple of funding them then vs. funding them now?