Comments
Note: This report was produced with only one week of desktop research, for the purpose of identifying promising causes to evaluate at depth. We only have low confidence in our findings here, and the conclusions should generally be taken by readers as merely suggestive rather determinative.
Summary
Factoring in the expected benefits of treating tinnitus (i.e. improved health and increased economic output) as well as the tractability of expanding sound therapy as a treatment option, I find that the marginal expected value of expanding sound therapy to treat tinnitus to be 450 DALYs per USD 100,000, which is around 70% as cost-effective as giving to a GiveWell top charity.
Key Points
- Importance: This is a strongly important cause, with 3.19 * 108 DALYs at stake from now to the indefinite future. Around 82% of the burden is health related, while 18% is economic in nature.
- Neglectedness: The efforts of governments/nonprofits/business in solving the problem are likely insufficient, as indicated by low levels of research funding.
- Tractability: A moderately tractable solution in the form of direct delivery of masking devices (a form of sound therapy) by collaborating with local primary care physicians is available.
Discussion
- The estimation of the proportion of tinnitus sufferers who want treatment but currently lack it is highly uncertain, relying as it does on a very simplified model with parameter calibrations that could very well be off.
- The projected growth in the disease burden of tinnitus over time is also very rough, and is certainly something that would be materially improved by expert advice and modelling.
- There is considerable uncertainty over the effectiveness of the specific treatment we evaluate – masking – as the evaluation relies on the results of a meta-analysis that examined sound therapy in general rather than masking in particular; we may also be overly optimistic as to the cost of the masking devices used to treat tinnitus.
- On the flipside, we might be understating the effectiveness of this intervention insofar as failure to convince individual physicians to implement the solution simply means freeing up resources to support another persuaded physician. I suspect the main limiting factor in this endeavour will be more the time of the charity co-founders and employees, especially in a context where they may have to travel to various rural clinics to truly reach the unserved.
Expected Benefit: Improved Health from Treating Tinnitus
The primary expected benefit from treating tinnitus is improved health, in terms of less disability and suffering. This benefit is around 2.6 * 108 DALYs, and is modelled in the following way.
Moral Weights: The value of averting one year of tinnitus (i.e. the disability weight of tinnitus) is calculated by taking the various disability weights for various degrees of hearing loss (mild, moderate, moderately severe, severe, profound and complete) with ringing, and subtracting the various degrees of hearing loss (mild, moderate, moderately severe, severe, profound and complete) without ringing, and then averaging. This yields a disability weight of tinnitus – specifically, the condition of hearing ringing noises in your ear even when no external cause is evident – of 0.07.
Scale: In terms of the proportion of the population affected by tinnitus in the baseline year of 2023 – per the Jarach et al meta-analysis, the pooled prevalence of any tinnitus amongst adults is 14.4% while the pooled prevalence of any tinnitus among children and adolescents is 13.6%. To calculate aggregate pooled prevalence, I take a population-weighted average of the adult and non-adult prevalence rates. However, (a) for the non-adult rate, I weigh the estimated headline rate of 13.6% against the young adult rate (9.7%) insofar as the data on children and adolescents is less reliable (e.g. children are more frequently asked about tinnitus without specifically mentioning the name of the symptom, and children may report the presence of noise to please the interviewers). Besides, there is reason to doubt that young children have higher prevalence rates of tinnitus than young adults anyway, given the otherwise strong empirical relationship between increasing age and tinnitus (not to mention the strong theoretical relationship between increasing age and increasing damage to the ear and hence hearing impairment. I use equal weightage in the weighing to balance in-sample data unreliability on the one hand and external validity on the other. Meanwhile, (b) I weigh the overall aggregate pooled prevalence against chronic tinnitus prevalence rates given the presence of publication bias in the former and the latter providing a more conservative estimate, weighing towards the any-tinnitus estimate, since it suffers from just publication bias, while the chronic tinnitus estimate is both for a narrower definition and from a much smaller sample size. All this yields a prevalence rate of around 13%.
At the same time, global population in 2023 is expected to be 8,045,311,448.
Multiplying the prevalence rate and population, this yields a total number of tinnitus sufferers in 2023 of 1,064,041,781.
Of course, not everyone in this population wants treatment, or (if they want it), isn't already getting it. To calculate this proportion of tinnitus sufferers who want treatment but lack it, I model people getting treatment for tinnitus as a function of tinnitus sufferers wanting to do what's best for themselves (e.g. treatment is beneficial in treating their tinnitus, but they may also be worried about the perceived costs like the inconvenience of sound therapy, the side effects of drugs, or being discomfited by CBT), subject to affordability constraints. In high income countries, around 54.67% of tinnitus sufferers get treated (n.b. this is calibrated using three studies, of the US, UK and South Korea, with the South Korean figure estimated by dividing total treated by estimated total prevalence; overall, a weighted average is taken, with the South Korean estimate penalized for relying on a relatively longer and more uncertain chain of logic in arriving at the country-level estimate). Meanwhile, health coverage in high income countries is around 90%. Together, this suggests that around 60.81% of tinnitus sufferers in high income countries want to get treated (conditional on being able to afford it). The upshot is that the global proportion of tinnitus sufferers who are potentially treatable is simply (a) this proportion in high income countries that is willing to be treated, less their present treatment proportion; and (b) the proportion willing to be treated in LMICs (as given by the high income willing-to-be-treated proportion, assuming similar global rates), less their present treatment proportion (as estimated by multiplying the willing-to-be-treated proportion with their health coverage proportion), (c) averaging the two by weighing for population in high income countries vs LMICs.
Finally, by multiplying the number of tinnitus sufferers by the proportion who want treatment but lack it, we get the critical figure we need of the number of tinnitus sufferers who want treatment but lack it in the baseline year of 2023 – around 227,747,926 people.
Persistence: The problem of tinnitus is likely to persist, and eliminating it will bring benefits not just for one year but across multiple years. In terms of how this multi-year benefit is to be discounted –
Firstly, I discount for the probability of our solution (sound therapy, as will be discussed below) not persisting (i.e. the treatment effect being reversed): Assuming an intervention of providing full treatment as soon as possible in a single year to all tinnitus sufferers who want treatment but lack it, the reversal rate is a a function of both the relapse rate as well as the replacement rate (i.e. the population experiencing turnover from some people dying out and others entering into it). For the former, 7.9% of patients who achieve total remission nonetheless relapse over an 18-month period, which yields a 5.27% per annum relapse rate. For the latter, it can be approximated as the inverse of life expectancy. Overall, this gives us a reversal rate of 6.56% per annum.
Secondly, I apply a block discount to account for the proportion of disease burden that would be solved by other agents' intervention anyway (i.e. governments, nonprofits, businesses). Broadly speaking, research into hearing disorders and tinnitus in particular is severely underfunded by government agencies (e.g. the US National Institute of Health, or the European Union's various national funding agencies). Meanwhile, funding by private non-profits (e.g. the American Tinnitus Association, or the Wellcome Trust in London) is comparatively modest, which shows in the small number of studies on tinnitus published. Finally, the pharmaceutical pipeline is scarce – companies are not spending to develop new treatments because of our still incomplete understanding of tinnitus's pathophysiologic mechanisms. On the basis of all this, I assess that governments/nonprofits/businesses are uninterested in and unlikely to make a push to expand tinnitus treatment to those who need but lack it (especially in LMICs), the way they might do for the likes of AIDS/malaria/COVID. Hence I take the proportion of the remaining tinnitus disease burden that will be counterfactually solved by various agents (excluding the effects from the secular improvement in health systems) to be 0.1%, and the remaining disease burden still requiring treatment to be 99.9%.
Thirdly, I take into account how the proportion of the disease burden requiring treatment will evolve over time given structural trends. To model the growth of the disease burden over time, I model total number of tinnitus sufferers as a function of prevalence and population. The former itself is a function of the original baseline, plus growth from age and non-age reasons.
- The per annum growth from age reasons is estimated by using Stohler et al's British data on tinnitus incidence rate by age group to estimate increase in incidence from increase in age, and then multiplying by the year-on-year increase in median age (as given by UN estimates).
- The per annum growth from non-age reasons is calculated by using Stohler et al's British data on growth in age-standardized incident rate. To the extent that cultural trends are relevant (e.g. increasing education levels causing people to eat more healthily/exercise more and hence be less likely to suffer potential tinnitus risk factors like obesity, smoking and hypertension), this is taken into account of here. Note that the analyses in both (a) and (b) assume that prevalence scales linearly with incidence, which will be the case so long as disease duration remains constant.
- Finally, population growth and eventual decline is modelled by pulling from UN estimates.
- Last but not least, economic trends will matter, with greater wealth expanding access to treatment. I model this by using the difference in health coverage between high income countries and LMICs, and dividing by the number of years required for the average LMIC to reach current average high income country GDP given existing growth rates, to yield the per annum growth in treatment rates and hence the per annum reduction in the potentially treatable tinnitus population. That said, I cap the age and non-age growth extrapolation to 2100 due to uncertainty over longer term trends; I also freeze population estimates from 2101 onwards, to 2100 levels, since that is where the high-confidence UN estimates end. For reduction in potentially treatable tinnitus population due to economic growth expanding health coverage, I put a floor at 0.06081 given current rich world coverage rates and the proportion of people who want to be treated conditional on being able to afford it.
The projected growth of the tinnitus disease burden requiring treatment given structural trends is shown in Diagram 1. Note that the sharp reversal after mid-century is precisely because of the cap in coverage rates – you can't expand healthcare forever.
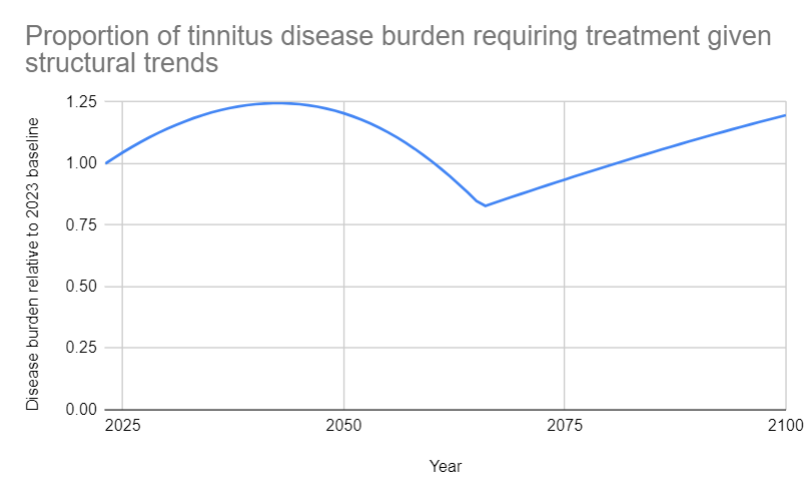
Diagram 1: Proportion of tinnitus disease burden requiring treatment given structural trends
Fourthly, I discount for the probability of the world being destroyed anyway (i.e. general existential risk discount). I take into account the probability of total nuclear annihilation, since the benefits of saving people from tinnitus in one year is nullified if they had already died in a previous year. For the exact risk of total nuclear annihilation, I take it to be one magnitude lower than the risk of nuclear war itself, since nuclear war may not kill everyone. For the probability of nuclear war, I use the various estimates on the probability of nuclear war per annum collated by Luisa, but with accidental nuclear war factored in, and then calculate a weighted average that significantly favours the superforecasters. The reason for this is that (a) the estimate of the probability of intentional nuclear war based on historical frequency is likely biased upwards due to historical use being in a MAD-free context; (b) the probability of accidental nuclear war based on historical close calls is highly uncertain due to the difficulty of translating close calls to actual probabilities of eventual launch; and (c) experts are notoriously bad at long-range forecasts, relative to superforecasters. Meanwhile, I do not take into account other existential risks like supervolcano eruption and asteroid impact, since the chances of those occurring at all is very marginal per Denkenberger & Pearce, let alone the chances of such events killing everyone and not just most people. Overall, therefore, I treat the general existential risk discount to be just the risk of nuclear war but adjusted a magnitude down – around 0.07% per annum.
Fifthly, I apply a broad uncertainty discount of 0.1% per annum to take into account the fact that there is a non-zero chance that in the future, the benefits or costs do not persist for factors we do not and cannot identify in the present (e.g. actors directing resources to solve the problem when none are currently doing so).
Overall, by taking the projected growth in disease burden requiring treatment due to structural trends up to 2100, and discounting each year's disease burden by the block discount (i.e. agents counterfactually solving this problem) and the other per annum discounts (i.e. solution reversal discount, existential risk discount, uncertainty discount), the total proportion of the remaining problem that would be counterfactually solved by our intervention can be calculated, and is displayed in Diagram 2.
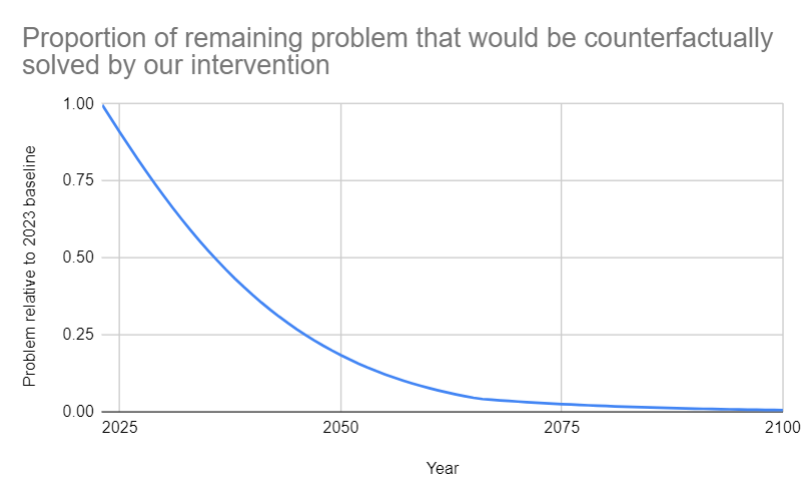
Diagram 2: Proportion of remaining problem that would be counterfactually solved by our intervention
Value of Outcome: By summing the discounted per annum relative values for 2023-2100 as shown above, and then using a perpetual value formula for 2101 to infinity, we can estimate the raw perpetual value of improved health from treating tinnitus as 2.6 * 108 DALYs.
Probability of Occurrence: In terms of the probability of tinnitus being an actual problem that harms people – unlike longtermist problems, there is no uncertainty that this is an actual problem. The scatter of tinnitus prevalence estimates is wide, but most study results have shown rates of between 10% and 15% of the adult population, and it's not as if the problem has been solved since. Hence, the probability that tinnitus is a problem can be trivially assigned a 1.
Expected Value: In all, the expected value of improved health from treating tinnitus is just 2.6 * 108 DALYs.
Expected Benefit: Increased Economic Output
Treating tinnitus is also expected to be beneficial in economic terms. This benefit is around 5.91 * 107 DALY, and is incorporated into the model in the following manner.
Moral Weights: I take the value of doubling consumption for one person for one year to be 0.21 DALYs. This is calculated as a function of (a) the value of consumption relative to life from GiveWell's IDinsight survey of the community perspective, as adjusted for social desirability bias, and (b) CEARCH's estimate of the value of a full, healthy life in DALY terms. For more details, refer to CEARCH's evaluative framework.
Scale: At the outset, it will be important to estimate the economic burden of tinnitus relative to annual income per tinnitus sufferer. To do this, I look at three separate estimates. Firstly, I rely on the Goldstein et al estimate, taking their US data on the direct medical cost per patient and dividing by annual income to get the economic burden of tinnitus relative to annual income per tinnitus sufferer. Secondly, I look at the Maes et al estimate, taking their Dutch data on the total costs in euros (inclusive of direct medical costs, other treatment-related expenditure, as well as productivity loss), converting it to USD, dividing it by sufferers to get the total costs per tinnitus sufferer, and then dividing by annual income to get the economic burden of tinnitus relative to annual income per tinnitus sufferer. Thirdly, I consult the Shi & Martin estimate, taking their Chinese data on the cost of treatment per person in the form of hearing aids, discounting by the average number of years (i.e. five) that the hearing aids can be used for, and then dividing by annual income to get the economic burden of tinnitus relative to annual income per tinnitus sufferer. In calculating the weighted average of these three estimates, I apply the following relative penalties. One, I penalize the Goldstein et al and Shi & Martin estimates for not incorporating other treatment-related costs or productivity costs. Two, I penalize the Goldstein et al and Maes et al estimates for being less relevant to the LMIC context, which we are focusing on given the lower healthcare coverage and higher avertable disease burden. Three, I penalize the Shi & Martin estimate for only looking at one particular form of treatment. Overall, I weigh the Maes et al estimate heavier than the other two in relative terms, and estimate an economic burden of approximately 7% annual income per sufferer per annum due to tinnitus .
This means a corresponding 7% increase in the degree of consumption doubling per tinnitus sufferer if their tinnitus is cured.
And hence, we would have 1.68 * 107 in total number of consumption doublings achievable by curing tinnitus in the baseline year of 2023,as calculated by multiplying the degree of consumption doubling per tinnitus sufferer if their tinnitus is cured and the total number of sufferers who want treatment but lack it in the baseline year of 2023.
Persistence: With the economic burden proportional to the disease burden, the same per annum discounts, block discount, and projections of the disease burden over time, as discussed in the previous section, are used here as well.
Value of Outcome: Overall, the raw perpetual value of increased economic output is 5.91 * 107 DALYs.
Probability of Occurrence: The same probability as before is applied.
Expected Value: Overall, the expected value of increased economic output is 5.91 * 107 DALYs.
Tractability
To summarize our tractability findings: we can solve 0.000001 of the problem per additional USD 100,000 spent on direct delivery of sound therapy.
Direct delivery of sound therapy is the preferred option because it compares favourably relative to the alternative solutions for treating tinnitus. In terms of the effectiveness of various candidate treatments for tinnitus, Liu et al's network meta-analysis suggests that (a) sound therapy (e.g. masking, habituation) is effective, as are (b) drugs, while (c) education (e.g. counselling) is not, even as certain combinations of the three are effective, more so than individual treatments. In terms of the relative effectiveness of these various treatments and their combinations, we have in declining order:
- Sound therapy with drugs and education
- Sound therapy with education ~ sound therapy with drugs
- Sound therapy
- Drugs
- No treatment.
Meanwhile, for other candidate treatments:
- Emerging sound treatments lack the support of trial evidence so far
- Alternative medicine may have placebo-induced distress-reduction effects, but there are non-trivial risks (e.g. ear candling causing burns)
- Brain stimulation is backed by some promising evidence so far but the long term risks are unclear
- Laser treatments are ineffective, according to most studies
- As for surgery, Cochlear implantation is very effective but applicable only to a tiny proportion of tinnitus sufferers (i.e. those with profound hearing loss)
Separately, note that we are constrained by the lack of trained therapists in the countries where tinnitus treatment is presumably in the least supply and where the avertable disease burden is highest (i.e. LMICs) – which makes educational consultation infeasible. In contrast, distributing sound therapy equipment (e.g. maskers) and drugs is fairly straightforward a matter, and is achievable through partnering with primary care physicians.
Finally, note that sound therapy is potentially cheaper than drugs, and more effective besides; given a limited budget, we should therefore focus on sound therapy alone.
And as for our theory of change:
- Step 1: Persuade primary care physicians in LMICs to accept resources and training for the provision of sound therapy.
- Step 2: The physicians treat tinnitus sufferers who want treatment but currently lack it.
- Step 3: The treated individuals see a reduction in the disease burden suffered.
Step 1: To assess the probability of persuading primary care physicians to accept resources and training for the provision of sound therapy, so that they can actually treat the patients they diagnose, I consult both outside and inside views.
For the outside view, I consult three reference classes: (1) the general success rate of Charity Entrepreneurship (CE) charities; (2) physician willingness to use sound devices to combat tinnitus; and (3) degree of support for lifelong learning amongst rural Chinese physicians (as an indicator of how willing LMIC doctors will be with respect to subjecting themselves to medical training). Unfortunately, all three reference classes have their flaws. Firstly, the CE incubatee reference class is biased downwards insofar as charities can fail for other reasons (e.g. funding) than inability to deliver on their core service. Secondly, the reference class of physician willingness to prescribe sound devices to combat tinnitus is flawed insofar as the prescription rates may well indicate doctors reserving sound therapy for more serious cases of tinnitus and not a general scepticism towards this treatment method. And on top of that, we have to worry about external validity. Thirdly, the lifelong learning reference class suffers from uncertainties inasmuch as positive attitudes to lifelong learning need not translate to actual likelihood of a busy doctor agreeing to and attending more training. And again, external validity worries surface. I penalize the latter two reference classes relative to the first, yielding a weighted aggregate probability of around 44%.
For the inside view, I reason as such. On the one hand, physicians presumably care about their patients well-being and will welcome any additional resources and ways to treat them for tinnitus. The risk that patients' complaints on the ringing in their heads being dismissed out of hand seems low, insofar as interest and recognition of tinnitus has improved in the past few decades, partly as a result of advances in neuroscience. On the other hand, it will be a drain on doctors' time to get training for the implementation of sound therapy. On balance, it appears to me that persuading doctors to accept resources and training for the provision of sound therapy is not especially implausible (i.e. <=10%); and something like a 50% chance seems reasonable.
Overall, while the inside view is subject to a lot of the usual inferential uncertainty, the outside view is particularly flawed in this case – hence, I give equal weightage out of ignorance more than anything, and estimate a probability of around 47% for persuading primary care physicians to accept resources and training for the provision of sound therapy.
Step 2: As for the proportion of tinnitus sufferers (who want treatment but lack it) ultimately being treated – this is a function of the number of patients treated, divided by the total number of tinnitus sufferers who want treatment but lack it. Number of patients treated is in turn a function of the budget (normalized at USD 100,000), the proportion of the budget that can be spent on core services, and the per patient cost of treatment. For the proportion of the budget that can be spent on core services, I take the outside view of a weighted average of what AMF, Malaria Consortium and New Incentives spend on their core services, penalizing NI for being less procurement-oriented (n.b. I do not use an inside view as I do not believe I have sufficient experience on direct delivery logistics to make an accurate call). The per patient cost of treatment can be calculated by taking the cost of the sound therapy equipment – a masking device that is basically a white noise generator, and which costs around USD 25 – and multiplying by the number of such devices the average sufferer will need across the course of their life (around 2.7, given that the average sufferer is around 60, and the average lifespan is 73.5 and such hearing devices last around 5 years on average). Overall, the proportion of tinnitus sufferers (who want treatment but lack it) will be approximately 0.000005.
Step 3: Once patients are actually treated, we can expect some degree of disease reduction per patient – though not a total cure. Sound therapy reduces Tinnitus Handicap Inventory (THI) scores by -30.01 relative to no treatment, and by taking this mean reduction from treatment and divide by the average THI score of sufferers of 54.2, we can calculate the reduction in tinnitus disease burden per sufferer from use of sound therapy as around 55%.
Overall, therefore, the proportion of disease reduction from distributing sound therapy devices – as a function of (a) the probability of persuading primary care physicians to accept resources and training for the provision of sound therapy; (b) the proportion of tinnitus sufferers who want treatment but lack it ultimately being treated; and (c) the degree of disease reduction achieved per patient – will be 0.000001.
In terms of costing, we can take the one year operating cost of a direct delivery charity to be a normalized USD 100,000, as it does not matter for the purposes of our calculations; proportion of disease reduction from direct delivery scales with expenditure, and so tractability does not change regardless.
Putting problem reduction fraction and costing together, we see that the proportion of problem solved per additional USD 100,000 spent is 0.000001.
Marginal Expected Value of Expanding Sound Therapy to Treat Tinnitus
All in all, the marginal expected value of expanding sound therapy to treat tinnitus is 450 DALYs per USD 100,000 spent, making this around 70% as cost-effective as a GiveWell top charity.

