This is a compelling proposal. The use of books and peer support for the treatment of depression/anxiety is an extremely cost-effective way of increasing well-being, and even more so when focused on child mental health in LMICs.
I mainly had questions about the details of implementation, especially whether this proposal could make use of pre-existing resources. As you might know, the WHO has developed a program called Early Adolescent Skills for Emotions (EASE), for ages 10-14. Among other virtues, having a standardized framework with the imprimatur of the WHO might be attractive both from the point of view of research and of funding.
EASE is a bit different from each of the four methods you outline – for one thing, it involves some training for caregivers, which as I understand it none of your four methods does. Do you think EASE could be an appropriate intervention for your population? Would there be special obstacles to its implementation in the Philippines (according to the Mental Health Innovation Network, EASE is being trialed in Tanzania, Lebanon, Jordan, and Pakistan)?
This is the third in a sequence of posts taken from my recent report: Why Did Environmentalism Become Partisan?
Summary
Rising partisanship did not make environmentalism more popular or politically effective. Instead, it saw flat or falling overall public opinion, fewer major legislative achievements, and fluctuating executive actions.
Public Opinion...
This post presents the executive summary from Giving What We Can’s impact evaluation for 2025. At the end of this post we share links to more information, including the full report and...
By: Shen Javier, Mae Muñoz, AJ Sunglao, Zam Superable
Summary
13% of children and adolescents globally had a mental disorder. Anxiety and depressive disorders make up almost half of the mental health disorders they experience.
Annually, US$387.2 billion worth of human capital is lost due to mental health conditions in children and adolescents aged 0 to 19.
Mental disorders developing at this life stage persist in adulthood. Certain disorders are also a risk factor for developing other types of mental disorders.
There is an association between childhood adversities and mental health disorders. Estimates show that eliminating childhood adversities would lead to a 30% reduction in mental disorders.
Mental health disorders have an early onset but it takes people with mood and anxiety disorders 6 to 23 years to get treatment.
The mental health burden in children and adolescents is disproportionately carried by LMICs. 90% of the world’s children and adolescents are living in less developed regions and more than half of the DALYs associated with mental health are found in middle-income countries.
In LMICs, mental health issues among children and adolescents are particularly pressing due to their exposure to a broader number of risk factors(e.g. poverty, poor health, poor education, violence) compared to their counterparts in high-income countries (HICs).
There are many interventions that have demonstrated effectiveness in treating different mental disorders in children and adolescents. However, there are still some uncertainties about the effects being demonstrated at a larger scale and/or in a different setting.
The top 4 mental health charity ideas we found to start in LMICs(more specifically, in the Philippines) are:
Self-Help Workbooks for Children and Adolescents
School-based Psychoeducation for Intermediate Level Students
Guided Self-Help Game-based App for Adolescents
Youth-led Mental Health Support
Background
This shallow investigation on child and adolescent mental health (CAMH) in low-and-middle-income countries (LMICs) is part of Effective Altruism Philippines’ Mental Health Charity Ideas Research. We identified the top mental health interventions for children and adolescents that are most promising to build as charities in the Philippines.
What is the problem?
Scale and nature of mental health conditions in children and adolescents
Mental health conditions among children and adolescents continue to be an important global concern. Estimates indicate that 13%, 166 million of 1.2 billion, of 10- to 19-year-olds in the world had a mental disorder (UNICEF, 2021). Of the different mental disorders experienced by adolescents, the Global Burden of Disease Study by the Institute for Health Metrics and Evaluation (IHME) estimates anxiety and depressive disorders constitute 40% of the mental health disorders experienced by adolescents (UNICEF, 2021). This is followed by conduct disorders and attention-deficit or hyperactivity disorders each making up 20%.
About one 10- to 19-year-old ends their own life every 11 minutes, amounting to 46,000 children and adolescents per year and suicide being the fifth leading cause of death for this age group (UNICEF, 2021). To compare with other mortality causes, for boys aged 15 to 19, suicide is the fourth leading cause of death after road injury, interpersonal violence and tuberculosis. For girls aged 15 to 19, it ranks third after tuberculosis and maternal conditions.
These figures likely underestimate the scale of mental health conditions in 10 to 19-year-olds. Mental health conditions are historically underreported likely due to the stigma surrounding them. In addition, there is limited data from low-and-middle-income countries where most of the world’s adolescents live and these places only get 2% of mental health research funding (UNICEF, 2021).
Consequences of mental health conditions in children and adolescents
Every year, US$387.2 billion worth of human capital is lost due to mental health conditions in children and adolescents aged 0 to 19 (UNICEF, 2021). Of this, US$340.2 billion reflects disorders that include anxiety and depression, and US$47 billion reflects the loss due to suicide. These economic costs are estimated by assigning one disability-adjusted life year (DALY) attributable to mental health a monetary value that represents the contribution of children and young people to the economy if they were not affected by mental health issues. The value of this economic contribution is based on the country’s gross domestic product per capita.
Mental disorders developing at this life stage have shown a high degree of continuity in adulthood (WHO, 2005; Kessler, 2007). A longitudinal study conducted by Costello et. al. (2003) aimed to track the development of mental disorders by assessing children aged 9 to 13 yearly up until they are aged 16. Children who were diagnosed in the previous year with a mental disorder were three times more likely to have a disorder in the subsequent data collection (Costello et al., 2003). Except for phobia, most disorders (e.g. panic disorders, psychosis, substance use disorders) persisted after their initial onset (Costello et al., 2003). Diagnosis of certain disorders was also a risk factor for developing other disorders. This continuity pattern is observed in depression to anxiety, anxiety to depression, ADHD to oppositional defiant disorder, and anxiety and conduct disorder to substance abuse (Costello et al., 2003).
Even outside diagnosis, children and adolescents still suffer later in life without proper mental health support. Types of childhood problems predict the likelihood of developing specific adult psychopathology – children with anxiety and depression-related problems were at risk of developing internalizing disorders and children with childhood delinquent behaviors were at risk of developing externalizing disorders (de Girolamo et al., 2012).
Using the World Mental Health Survey data, Kessler et al. (2010) examined the association between childhood adversities and adult mental disorders. Childhood adversities in the study included interpersonal loss (parental death, parental divorce, other separation from parents), parental maladjustment (mental illness, substance misuse, criminality, violence), maltreatment (physical abuse, sexual abuse, neglect), life-threatening respondent physical illness and family economic adversity. They showed that childhood adversities have a prevalence rate of 40% globally. They concluded that all childhood adversities are linked to an elevated risk of developing mental disorders in adulthood such that eradication of childhood adversities would lead to a 30% reduction of mental disorders, regardless of income classification of countries (Kessler et al., 2010). This reduction is for all types– mood, anxiety, behavior and substance disorders. Among the different childhood adversities, the strongest predictor of developing disorders is maladaptive family functioning which includes parental mental illness, child abuse and neglect (Kessler et al., 2010). Individuals who developed mental health disorders are 1.6 to 2.0 times more likely to have grown up in such environments. They are also 1.1 to 1.5 times more likely to have experienced other childhood adversities. In addition, they found that exposure to multiple childhood adversities compounds and increases one’s predisposition for developing mental illness later in life (Kessler et al., 2010).
How neglected is child and adolescent mental health?
Treatment gap
Those who do get treatment only make up 27.3% to 95.3% of those with anxiety, 33.9% to 51.8% of those with impulse control and 52.7% to 76.9% of those with substance disorders (de Girolamo et al., 2012). Those with mood disorders have higher rates of treatment contact at 88.1% to 94.2% (de Girolamo et al., 2012). We found no good estimates for how these rates vary across years. Thus, we are uncertain about whether neglectedness in terms of existing services significantly differs across age groups. However, the case for children is unique due to its effects lasting more years as described in the section on consequences and disorders being harder to treat when more time has passed as will be discussed in the next subsection.
In 67 countries studies, less than 2% of their health care budgets are allotted to mental health (WHO, 2021 as cited in WHO, 2022). In the world’s poorest countries this means spending less than US$1 per person per year and in upper-middle-income countries, this only goes up to $US3 per person per year (UNICEF, 2021).
Treatment delay
Studies have shown that mental health disorders have an early onset. The World Health World Mental Health initiative (WMH) Survey Initiative, an epidemiological study exploring the lifetime prevalence and age-of-onset of mental disorders within the WHO countries identified that common mental health disorders begin to develop in childhood (Kessler et al., 2007). The earliest among these are impulse control disorders with a median age onset of 7-15 for attention-deficit/hyperactivity disorders and oppositional defiant disorders, 9-14 for conduct disorders, and 13 – 21 for intermittent explosive disorders (Kessler et al., 2007). In the anxiety disorder cluster, phobias and separation anxiety’s median age onset is 7-14 (Kessler et al., 2007). Other forms of anxiety disorders (generalized anxiety disorders, post-traumatic stress disorder, and panic disorder) and mood disorders tend to appear later in life (Kessler et al., 2007). Substances use disorders are often observed to begin in adolescence and increase as teens transition to early adulthood (Kessler et al., 2007). Another study assessing individuals with DSM-IV diagnosis at age 26 has shown that almost half had already had a diagnosable disorder at 11-15 years of age, and three-quarters met their first diagnosis at 18 years old (Kim-Cohen et al., 2003, as cited in de Girolamo et al., 2012).
Despite these early onsets of mental disorders, it is only after 6 to 8 years that those who have mood disorders get treatment while it takes 9 to 23 years for those who have anxiety disorders (Wang et al, 2005 as cited in de Girolamo et al., 2012).
It is important to treat children and adolescents as soon as possible. Within the domain of developmental psychopathology, changing the child’s maladaptive psychological patterns becomes more difficult the longer the child is left untreated, especially if the child bears these maladaptive patterns as they crossed significant life stages (Sroufe, 1997, as cited in Zeman & Suvege, 2016). For instance, children who experience an adverse life event such as bullying in early childhood may internalize the belief that others are set to harm them, which impacts their pattern of relating and eventually reinforce negative and aggressive peer relationships (Lansford et al. 2013, as cited in Zeman & Suvege, 2016).
Why focus on LMICs?
Mental health burden in children and adolescents in LMICs
In 10- to 19- year-olds, most of the mental health burden is found in middle-income countries (Global Burden of Disease, 2019). Almost half of the world’s DALYs associated with mental disorders are in lower-middle-income countries, a quarter in upper-middle-income countries, 15% in high-income countries and 13% in low-income countries.
Additionally, in LMICs, mental health issues among children and adolescents are particularly pressing due to their exposure to a broader number of risk factors compared to their counterparts in high-income countries (HICs). These risk factors include poverty, the absence of caregivers, problems with regard to physical health and nutrition, poor quality of education, and increased exposure to disasters, violence and armed conflict. Thus, LMICs have to carry most of the young’s mental health burden globally while still struggling to establish necessary services.
In terms of childhood adversities studied by Kessler et al. (2010), their prevalence and population attributable risk proportions do not vary widely across countries’ income classification. This may suggest that preventive interventions are needed more or less equally in different income levels while curative interventions are more needed in LMICs due to a large number of DALYs in the age group 10 to 19.
Neglectedness of child and adolescent mental health in LMICs
There are variable treatment coverage and quality across countries. WHO estimates that 29% of people with psychosis receive mental health care but this is 70% of people with psychosis reported to be treated in high-income countries and only 12% of people with psychosis reported to be treated in low-income countries (WHO, 2021 as cited in WHO, 2022). For major depressive disorder, minimally-adequate treatment comprises 23% of available treatment in high-income countries but only 3% in low- and lower-middle-income countries (Moitra et al., 2022, as cited in WHO, 2022).
Aside from a lower spending proportion on mental health in LMICs, they also have a scarcer mental health workforce compared to HICs. In LMICs, there is fewer than one mental health worker of any kind per 100 000 population (WHO, 2022). This figure only goes up to almost ten for upper-middle-income countries while it is more than 60 in high-income countries (WHO, 2022). The global median is 13 mental health workers per 100 000 population (WHO, 2022).
Here are other ways the public mental health gap is more apparent in LMICS as identified by WHO (2022).
Information gap: Less than 5% of mental health research funding goes to LMICs.
Governance gap: While 78% to 83% of low and lower-middle-income countries have a mental health policy or plan, only 3% to 14% report implementing a fully compliant policy or plan. For upper-middle-income countries and high-income countries, 87% to 89% of them have a mental health policy or plan with 25% to 32% implementing one that is fully compliant.
There are many challenges to improving CAMH policy in developing countries. Zhou et al. (2020) reviewed 31 publications and found six major challenges, namely: poor public awareness and low political willingness, stigma against mental disorders, biased cultural values toward children and adolescents and CAMH, lack of CAMH data and evidence, shortage of CAMH resources and unintended consequence of support from international organizations and nongovernmental organizations (NGOs). Biased culture values include the belief that children’s development cannot be changed and the perception of CAMH as a luxury or something not as important as physical health. On the other hand, support from other organizations may reduce the government’s sense of urgency and lead to a narrow focus on specific aspects of CAMH, especially disorder-specific actions, due to donors’ interest. This support may also disrupt the use of CAMH services due to their projects’ short-term lengths. This last issue should be kept in mind when getting started to found a charity.
The poor supply of quality mental health services suppresses demand (WHO, 2022). People become reluctant to get treated due to concerns about costs and time and there remains little to no options for them to avail services since two-thirds of low-income countries did not include mental health care in national health insurance schemes in WHO’s Mental Health Atlas 2020. Thus, many people remain untreated.
Unique advantages of starting a mental health charity in LMICs
Approximately 90% of the world’s children and adolescents are living in less developed regions (UN DESA, 2010). Focusing on these regions may already lead to eliminating suffering in most of the world’s young people. In addition, pilot-testing an intervention in even just one of these countries will already provide valuable insights because of the lack of research specifically made for these regions. Replicating the research or the intervention in other low-resource regions will also be easier since the settings are more similar (South-to-South cooperation) instead of adapting one made for high-resource or developed countries.
Children and adolescents also make up more than half of the population in these regions. Thus, the well-being of more than half of the developing countries can be improved if interventions target these age groups.
What are possible solutions?
Evidence of existing interventions
Nonspecific interventions
Psychosocial interventions include early stimulation programs carried out on children aged 0 to 3 years old to support neuro-cognitive development. Early stimulation programs teach mothers to positively engage their children in various enrichment activities which may include play, reading books, providing massage, physical touch, and listening to music, among others (Klasen & Crombag, 2013). Current evidence shows that the benefits of early stimulation programs may be sustained in the long term (Klasen & Crombag, 2013). In longitudinal studies, adolescents in early stimulation treatment groups reported fewer symptoms of anxiety and depression, and higher self-esteem, while parents noted fewer attention problems (Walker et al., 2006). In adulthood, they engaged in less violent behavior, had higher IQ and educational attainment, and had fewer symptoms of depression and social inhibition (Walker et al., 2011).
Interventions for Behavioral Problems
Proven interventions to address behavioral problems in children include parenting programs to manage a child’s maladaptive behavior, teacher training in the classroom, and psychosocial interventions targeted at children (Kieling et al., 2011). Programs implemented in LMIC may focus on one component or may integrate these various components.
There are several school-based programs, with teacher training and/or delivery of a social-emotional curriculum that has shown to be effective in reducing behavioral problems. For instance, an RCT study demonstrated that a 13-session universal program for elementary-aged children in China reduced behavioral problems and sustained this effect at 6-month follow-up (Hong et al., 2011, as cited in Klasen & Crombag, 2013). Incredible Years and Zippy’s Friends are two examples of programs adapted from HIC and implemented in LMICs (Kieling et al., 2011; Klasen & Crombag, 2013). In controlled trials conducted, these programs have shown to be effective at reducing problem behaviors and competencies among children aged 3 – 8 years old (Kieling et al., 2011; Klasen & Crombag, 2013).
Parenting interventions have also demonstrated effectiveness in this problem. An RCT of an 8-session parenting program delivered by non-specialized general health and social workers to parents of children with behavioral problems in Lebanon reduced children’s behavioral problems and parents used corporal punishment less when compared to control groups (Fayyad et al., 2010, as cited in, Klasen & Crombag, 2013). A brief parenting program, integrated into the primary health services, for parents of children aged 2- 6 years old (Kieling et al., 2011). A quasi-RCT study conducted indicates that intervention led to improvements in parenting practices and a decline in incidences of abuse (Oveisi et al., 2009, as cited in Kieling et al., 2011)
In adolescence, behavioral problems often targeted include sexual risk-taking behaviors and substance abuse. In China, community-based preventive programs have reduced drug use among adolescent men aged 15 – 19 years old (Wu et al., 2002, as cited in Kieling et al., 2011). In Africa, there are also programs aimed at preventing drug and alcohol abuse and sexual risk-taking behaviors to reduce HIV infection (Klasen & Crombag, 2013). In large-scale RCTs conducted Zimbabwe (Cowan et al., 2010, as cited in Klasen & Crombag, 2013) and Tanzania (Doyle et. al. 2010, as cited in Klasen & Crombag, 2013), these interventions have been effective in improving knowledge, attitude and educational planning.
Interventions for Emotional Problems
Interventions specifically for emotional disorders are often school-based universal prevention programs. Apart from these, targeted or selective preventions are provided to children who encounter emotional problems as an aftermath of a traumatic life experience.
Systematic reviews of school-based interventions in LMIC aimed at preventing emotional disorders for children and adolescents have shown that intervention yields benefits, although only a few of these studies used RCT design (Kieling et al., 2011; Klasen & Crombag, 2013). Some of these interventions are directed at children predisposed to disorders due to the presence of risk factors (e.g. poverty, trauma) or children with subclinical presentation, described as having features of the disorders but not meeting the threshold enough to be diagnosed with a disorder.
There are several examples of school-based interventions with varying components. A school-based physical activity program for 15-year old adolescents in an impoverished community in Chile resulted in improved self-esteem and alleviated symptoms of anxiety but not depression (Bonhauser et al., 2005, as cited in Klasen & Crombag, 2013). Another school-based CBT-informed program for sub-clinically depressed 8 – 15-year-old children in China reduced depressive symptoms among children post-treatment and was sustained at 3- to 6-months follow-up (Yu & Seligman, 2002, as cited in Klasen & Crombag, 2013). A school-based psychosocial intervention program in Mauritius for 12-16-year-old adolescents improved depressive symptoms, hopelessness, coping skills, and self-esteem post-intervention (Bonhauser et al., 2005 as cited in Kieling et al., 2011). In this intervention, effects on coping skills and self-esteem were sustained at 6-month follow-up (Rivet-Duval et al., 2010, as cited in Kieling et al., 2011)
For Trauma-Related Problems
Several of the interventions are designed for children who had encountered traumatic life experiences, such as war, migration, natural disasters, chronic poverty, death of a close relative (Klasen & Crombag, 2013). Outcomes targeted include reduction of symptoms of PTSD, anxiety, and depression.
A systematic review of interventions for children conflict-affected has shown that these interventions are effective in reducing negative symptoms and/or enhancing protective factors (Jordans et al., 2009, as cited in Kieling et al., 2011). In some studies that evaluated universal school-based or camp-based interventions, recommendations include the use of universal in conjunction with selective or indicated prevention (Klasen & Crombag, 2013). Universal interventions may yield positive outcomes (e.g. reducing aggression, psychosocial difficulties, enhancing pro-social behaviors), but are ineffective in reducing symptoms of PTSD, anxiety, and depression (Jordans et al., 2010). Programs that implemented a tiered approach, providing universal interventions for all children and selective interventions for children with more severe symptomatology, have demonstrated significant improvements in PTSD and depressive symptoms (Layne et al., 2008 as cited in Klasen & Crombag, 2013).
For Developmental Disorders and Childhood Disability
There are limited psychosocial interventions to prevent neurocognitive deficits. As risk factors for developing cognitive deficits are biological (e.g. undernutrition, micronutrient deficiencies, poor cognitive stimulation), most programs are target reducing or preventing exposure to these risk factors (Kieling et al., 2011). As a result, these programs often involve maternal and child nutrition supplementation, immunization, prenatal and perinatal health, and malaria intervention, among others (Kieling et al., 2011).
Among children with disabilities, there are different interventions available to support their development. The effectiveness of these interventions has only been proven through some RCTs and more non-controlled design studies (Klasen & Crombag, 2013). In one quasi-RCT in Vietnam, parents were trained to effectively engage with their pre-school-aged children with intellectual disabilities and supported by teachers through weekly home visit coaching sessions (Shin et al., 2009). Assessment afterward indicated that children in the treatment group improved in adaptive behaviors, motor skills, and personal care compared to control groups (Shin et al., 2009).
Another notable intervention includes the WHO community rehabilitation program (CBR), a lay-delivered intervention where parents and children with disabilities are provided support aimed at learning skills to enact daily living activities, increasing attendance in school for children, and finding income-generating activities for adults. Although no RCTs are available, program evaluation showed that intervention is effective in enhancing ability scores and rates of school attendance and employment (Lagerkvist, 1992, as cited in Klasen & Crombag, 2013).
A survey of 29 non-controlled evaluation reports from 22 countries across Asia, Africa, and Central Africa summarizes the effectiveness of community rehabilitation programs in improving the daily functioning of people with disability, supporting parents of disabled children in coping, and increasing school attendance for children with disability (Velema et al., 2008, as cited in Klasen & Crombag, 2013).
General characteristics that may work
Given the nature of CAMH and the challenges of developing mental health care in LMICs, here are some characteristics of interventions that can be successfully implemented in these settings.
Because of the scarce mental health workforce in LMICs, we favored interventions that employ task-shifting such that trained and employed lay health workers will deliver the guidance. Lay health workers carry out functions related to health care delivery who are trained in the context of the intervention but have no formal professional or paraprofessional certificated or degreed tertiary education (Lewin et al., 2005). It has been a widely-recognized option for delivering different healthcare services, especially in low-resource settings. In Sub-Saharan Africa, 10 out of 11 studies showed significant positive results on depression scores (Galvin & Byansi, 2020).
Because of stigma, introductions to mental health should be non-threatening. This means considering interventions focusing on stress, strengths, values, problem-solving etc.--more familiar terms than mental health.
Our top four ideas
Although various interventions result in positive changes in mental health, ideas selected within this scope of the review are primarily psychosocial interventions targeting psychological or social factors contributing to people’s mental health conditions. Narrowing the scope of our research was a function of two factors. One, our positionality as mental health professionals oriented in the field of psychology provides us with a more comprehensive understanding of the psychosocial interventions for mental health, including theoretical background and key considerations for implementation. More importantly, from an advocacy standpoint, pursuing a charity with mental health as a primary outcome looks like the easiest way to start the conversation on mental health in our country. We expect pharmacological interventions, policy interventions such as influencing mental health funding and meta ideas such as improving mental health data collection to gain less interest in the Philippines but we are excited to see research on these ideas.
To clarify, we looked for evidence that does not only focus on LMICs for the most part of our process. Studies considered were not specifically done in LMICs. It is actually very difficult to find studies about most of the ideas we researched that are in this setting since as mentioned, almost all of mental health research funding goes to developed countries. However, while writing about our top four ideas, we focused the evaluation of the implementation of the charity in the Philippines. We also already consulted Filipino experts. We still think that these top ideas are generalizable due to the wide evidence base we included but country-level differences in terms of acceptability and implementation aspects (e.g. funding, talent, government interest) shall be explored.
This is the set of criteria that we used to evaluate the top ideas. More details about them are found here: EA PH MHCIR Deep Reports WFM.
Effectiveness
Acceptability
Ease of implementation
Ease of scaling
Ease of funding
Here are the four mental health charity ideas we found that are most likely to be impactful in the Philippines. You can see an overview of the ratings per criteria and a CEA comparison here: EA PH MHCIR Deep Reports WFM. We have not updated our CEAs to consider different scenarios and we are still in the process of editing these and the deep reports for sharing with the public. The deep reports will discuss each idea’s evidence for effectiveness, theory of change, cost-effectiveness analyses and some aspects of implementation.
Idea Name
Description
Cost-Effectiveness ($ per unit, total costs)
Self-Help Workbooks for Children and Adolescents
This intervention will develop and distribute self-help workbooks to improve depression and anxiety symptoms in children and young adolescents, particularly 6 to 18-year-olds. Depending on the severity of mental health disorders, the workbook can be accompanied by weekly guidance by lay counselors through telephone, email, social media, or other available platforms.
$2.67 per WHO-5 improvement
School-based Psychoeducation for Intermediate Level Students in the Philippines
This preventive approach entails training and supervising teachers to deliver psychoeducation on mental health topics in their respective schools. Through weekly participatory learning sessions, students would learn to apply positive coping strategies, build interpersonal skills, and/or develop personal characteristics that would empower them to care for their mental health and navigate important life transitions.
$85.93 per GSES improvement
Guided Self-Help Game-based App for Adolescents
The intervention is a self-help game-based mobile application for help-seeking adolescents aged 12 - 19 years old. As a self-help format, the app aims to teach service users concepts and skills that will aid them in addressing MH concerns. The content of the app will be based on evidence-based therapeutic modalities. The game-based format is used to enhance service user engagement and prevent dropout.
$69.47 per SWEMWBS improvement
$36.89 per CDS-R reduction
Youth-led Mental Health Support
This intervention is a community-based intervention for adolescents aged 13-18. It uses task-sharing principles in delivering basic para-mental health support by training community members like SK officials and student leaders in basic mental health skills such as psychoeducation, peer counseling, and psychological first aid. The content of the training would be based on other community-based interventions like Thinking Healthy Programme, PM+, and Self Help+.
$105 per SWLS improvement
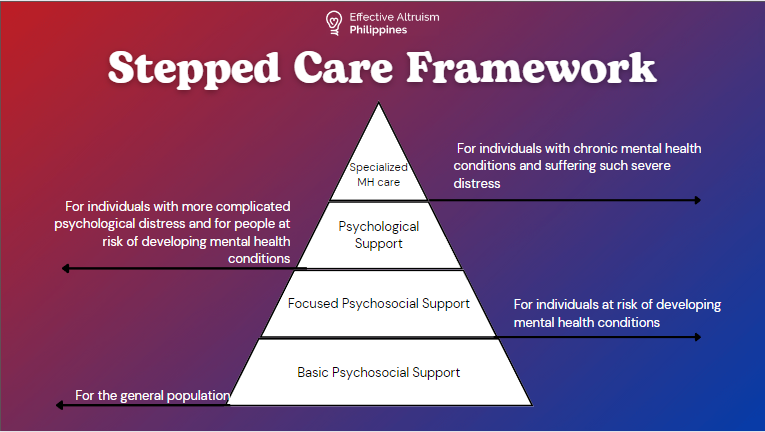
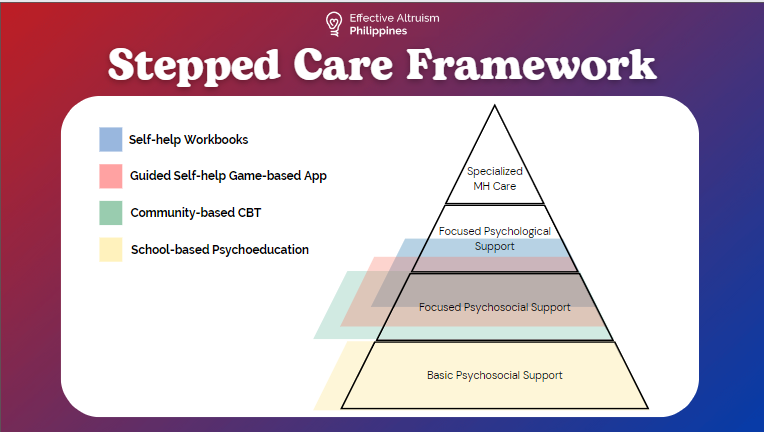
These ideas differ in the types of support they can provide as you can see in this stepped care framework.
Uncertainties and open questions
How much does the treatment gap vary across age groups?
The rate of treatment may not vary across ages or they may be another age group that is more lacking resources.
However, this is not the only criteria for focusing on one age group.
What is the specific age range of children and adolescents to focus on?
There are a lot of factors to consider when choosing such as type of intervention (e.g. Should we allow younger ones to use technology interventions?), type and level of engagement (e.g. Adolescents may prefer apps while children may prefer storybooks), and need of parental involvement.
Our research looked at a wide range of ages for children and adolescents. Generally, studies are usually on adolescents although we did not do a systematic comparison of studies for different ages. Experts we talked to generally agree about focusing on adolescents since they have more agency.
How long do these intervention effects last and how likely are they to demonstrate effects even at a larger scale and in a different setting.?
The answers to these questions depend from one intervention to another. Studies for an intervention usually have limited testing periods and samples and are usually set in HICs.
How effective would other types of interventions be? We only focused on psychosocial interventions but here are some other ideas.
Mental health policies
Pushing for larger mental health budgets
Better mental health data generation
More funding for mental health research
Inclusion of mental health in national surveys
Conclusion
Child and adolescent mental health is a promising new cause area for Open Philanthropy to fund. Mental health problems in this age group cause a lot of burden in terms of DALYs, mortality and economic costs. There are also mental health consequences that occur later in the lives of those affected by mental disorders at a young age. Most of these burdens are carried by LMICs. Many interventions have been proven to be effective. More resources are needed to better understand the problem and develop solutions fit for low-resource settings. A note on funding
We expect funding for pilot testing a mental health intervention to be difficult since most of the opportunities available are for research projects. Other sources may also be available depending on the target population’s location or mental health-related condition. Funding for the actual implementation and scaling up remain difficult too. Still, partnerships with the government and other organizations may be easier if the pilot test is successful. We believe that this state of funding also speaks about the neglectedness of mental health in general, not just of CAMH and hope that more opportunities become available soon.
There is minimal funding allotted for mental health projects outside developed countries. Two promising sources are listed below:
Wellcome is a foundation supporting research on mental health, infectious diseases, climate, and health. They offer funding schemes for mental health research and interventions.
The National Institute of Mental Health is the United States’s lead federal agency for mental disorders. They only offer grants for research which the new charity can apply for pilot testing of the intervention. They have Scale-Up Hubs to conduct implementation research on evidence-based mental health interventions for LMICs in the following regions: East Asia and the Pacific; Europe and Central Asia; Latin America and the Caribbean; the Middle East and North Africa; South Asia; Sub-Saharan Africa. Their research networks in Asia have not reached the Philippines yet.
Local Funding
Most likely, government agencies, educational institutions, foundations and other types of organizations can provide funding. In the Philippines however, most funding opportunities we found were only research grants.



This is a compelling proposal. The use of books and peer support for the treatment of depression/anxiety is an extremely cost-effective way of increasing well-being, and even more so when focused on child mental health in LMICs.
I mainly had questions about the details of implementation, especially whether this proposal could make use of pre-existing resources. As you might know, the WHO has developed a program called Early Adolescent Skills for Emotions (EASE), for ages 10-14. Among other virtues, having a standardized framework with the imprimatur of the WHO might be attractive both from the point of view of research and of funding.
EASE is a bit different from each of the four methods you outline – for one thing, it involves some training for caregivers, which as I understand it none of your four methods does. Do you think EASE could be an appropriate intervention for your population? Would there be special obstacles to its implementation in the Philippines (according to the Mental Health Innovation Network, EASE is being trialed in Tanzania, Lebanon, Jordan, and Pakistan)?
Here is an article on EASE: Improving access to evidence‐based interventions for young adolescents: Early Adolescent Skills for Emotions (EASE)
Here is a page on EASE at the Mental Health Innovation Network: Early Adolescent Skills for Emotions (EASE): a psychological intervention for young adolescents and their caregivers
Seconding the effectiveness of peer support interventions being potentially underexplored (disclaimer: it's my submission lol).