(This cause area report is viewable as a google doc here, and has a CEA here).
Executive Summary
Oral diseases (such as cavities) affect around 3.5 billion people worldwide; around 45% of the world’s population (WHO, 2022). In turn, it is likely that the severity of dental conditions (in terms of the suffering they cause) is underestimated—at least for people living in regions with poor access to dental healthcare. In particular, there is strong reason to think that disability weights (which are used to calculate DALYs) may underestimate the severity of dental pain. While oral healthcare is not necessarily under-resourced on a global level (e.g. countries such as the UK and US invest large amounts of money into both preventative and curative oral healthcare), some regions are extremely under-resourced, with very limited access to dental treatment. However, interventions such as fluoridation are an extremely cost-effective way to reduce oral health problems.
Summary
Oral diseases are largely preventable, yet they pose a major health and wellbeing burden: untreated dental caries (tooth decay) is the most common health condition according to the Global Burden of Disease (2019). Cavities are caused by a breakdown of tooth enamel by acids that are produced by the bacteria in plaque. Untreated decay can result in related oral health conditions, such as gum infection and tooth loss (Oral Health Conditions, 2020) which can result in chronic pain. Yet oral healthcare is extremely limited in Low and Middle Income Countries (LMICs); globally, the proportion of dentists per capita in High Income Countries (HICs) is almost 1:2000, yet countries such as Tanzania have a ratio of around 1:360,000 (Nyamuryekung’e et al., 2015; Uguru et al., 2020). This means that oral diseases which would be treated in HIC are likely to remain untreated in many LMIC—allowing mild infections to progress to painful and chronic conditions.
In this report, I argue that oral health in LMIC represents a promising funding opportunity for increasing global wellbeing. From the perspective of importance, poor oral health is both very common and has significant impacts upon wellbeing. The primary effect upon wellbeing comes directly from the experience of dental pain. In addition, there may also may be effects stemming from raising the risk of other diseases such as coronary heart disease and diabetes[1] (King et al., 2022), and smaller effects via reducing attendance at school and work. In addition, there is strong evidence that this problem will become larger in the future, as LMIC undergo the ‘nutrition transition’; a switch towards more sugary foods. Evidence from ‘key players’ in the global sugar industry (such as Coca-Cola and PepsiCo) suggests that they are switching their focus towards LMIC (Peres et al., 2019).
There are also strong reasons to think that dental health in LMIC is neglected—namely, the fact that many LMICs have very limited dental care (see Figs 9 and 10). This neglect reflects an underestimation of the burden of oral health diseases, which has occurred for several reasons. First, relative to other forms of health, dental ill health is unlikely to have a significant effect upon mortality—and most health funding bodies focus upon reducing mortality, rather than wellbeing per se (e.g. the WHO). Relatedly, most global health funding bodies utilise DALY estimates to prioritise new initiatives, but here I argue that DALY estimates do not adequately capture the burden of suffering caused by poor oral health. Second, dental healthcare is often poorly linked to existing healthcare systems (e.g. Benzian et al. 2011; Watt et al., 2019). Third, dental treatment has historically focused upon comparatively expensive curative treatment rather than preventative treatment—yet LMICs often struggle to fund curative treatment (Watt et al., 2019).
Overall, I think that oral healthcare in LMIC is very likely an important and neglected issue and therefore represents a promising funding opportunity. I also think that this issue is tractable. In particular, interventions such as salt and milk fluoridation are likely to be extremely cost-effective (my CEA roughly estimates a value of approximately $31 per WELLBY in the first year of set up, then $2 per WELLBY in subsequent years; see CEA). Note that salt fluoridation can be ‘tacked on’ to existing salt iodisation programs (Gillespie & Marthaler, 2005). I am less confident if there are suitable charities operating in this area, and am currently trying to identify and reach out to suitable organisations.
Importance
What is the problem?
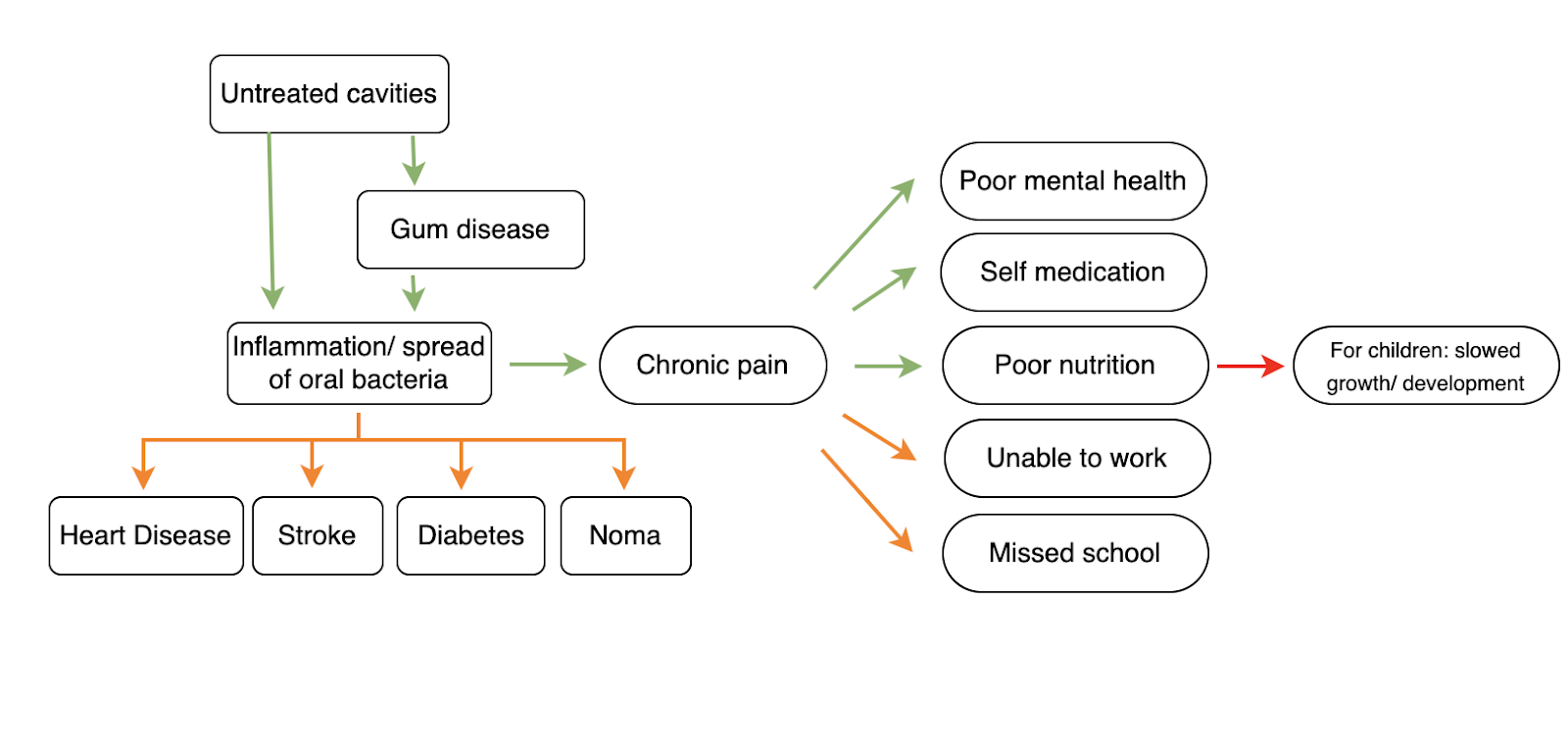
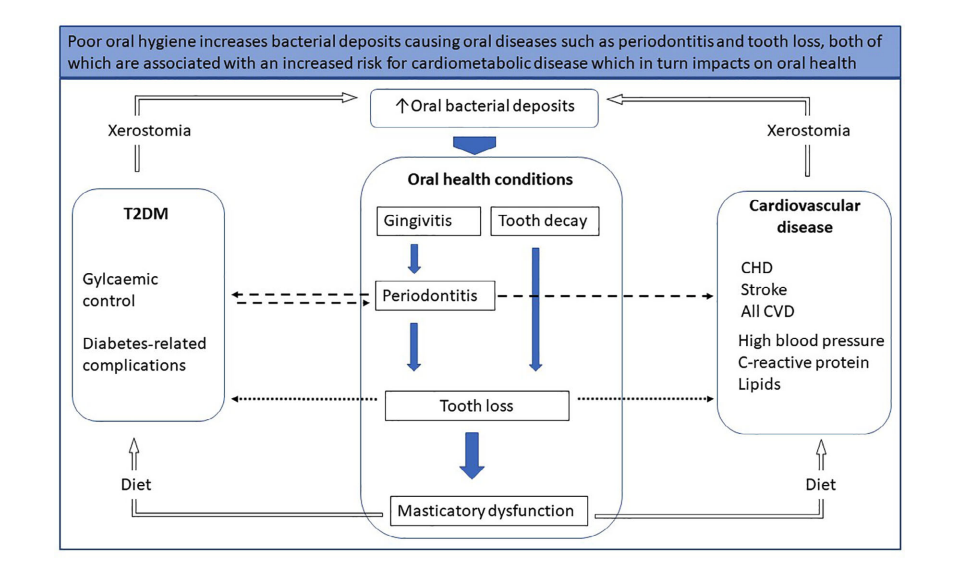
Oral health conditions cause approximately 0.82% of global DALYs [2] (GBD Results Tool | GHDx, 2019), despite being largely preventable (Oral Health, 2022). They cause suffering through dental pain (that can be severe, given the sensitivity of the nerves inside the tooth pulp), and through a number of indirect pathways—such as causing difficulty in eating and speaking, and by reducing attendance at school and work (see Fig 1).
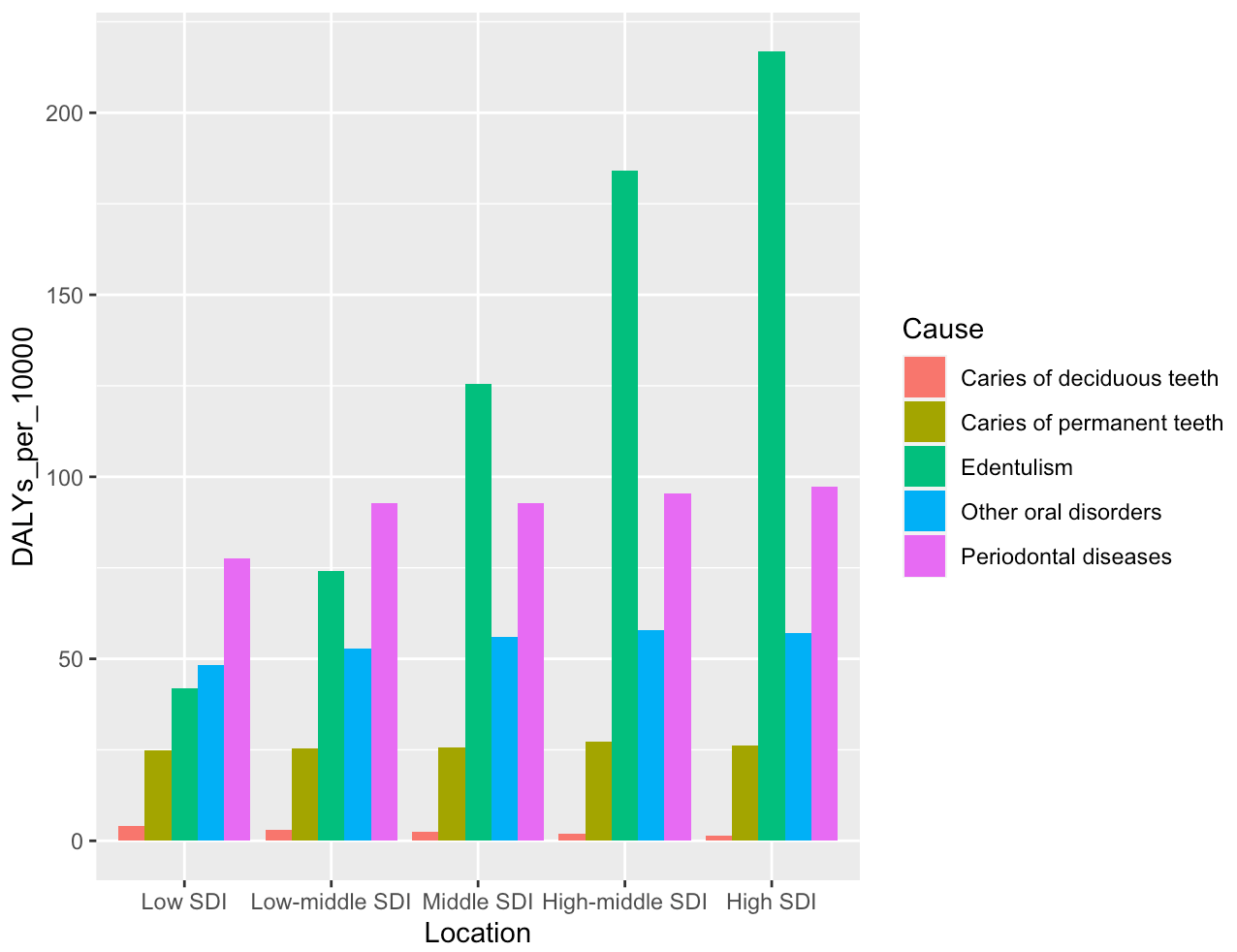
Oral health problems include dental caries, periodontal (gum) disease, edentulism (lacking any functional teeth), as well as other conditions such as cancers of the mouth: see Fig 2 for an overview of the relative DALY disease burden of each condition.[3] Since most interventions would act to target multiple oral healthcare conditions at once (e.g. fluoride reduces cavities as well as gum disease, and therefore subsequent tooth loss), this report examines oral healthcare broadly rather than focusing specifically upon a particular oral healthcare condition.
Impacts from poor oral healthcare
Pain
Dental caries are strongly associated with pain (e.g. Pentapati et al., 2021; Slade, 2001) because they provide access for bacteria to the sensitive nerve endings within the tooth pulp. If an infection (from a cavity or periodontitis) takes hold, it can spread to surrounding bone and risk sepsis. Even in mild cases, the anatomy of the tooth means that there is little room for infected tissue to swell without pressing on adjacent nerves. Evidence suggests that dental pain is both common and frequently severe—especially in areas with limited dental healthcare access, where dental disease is more likely to progress towards painful stages. Evidence reviewed below.
Dental pain is common
Dental problems—and consequent dental pain—are extremely common: more than 80% of people will have had at least one cavity by the age of 34 (CDC: Oral Health Conditions, 2020), and untreated dental caries are the most common health condition according to the Global Burden of Disease (2019). While cavities can be asymptomatic, cavities generally become symptomatic without treatment (Cavities/Tooth Decay - Symptoms and Causes, n.d.).
Accordingly, rates of dental pain are high. In children, a meta-analysis estimated that 20% of children below five and 40% of children between 6 and 12 years of age have experienced dental pain, with studies from Africa reporting the highest pooled prevalence (50.1%) (Pentapati et al., 2021). Heterogeneity in this meta-analysis was high, but the prevalence of dental pain in children is a well-established finding. Using specific studies (and noting that different studies use different timeframes); 61.4% of children in Nigeria reported experiencing dental pain in the last 3 months (Adeniyi & Odusanya, 2017), 16.5% of Brazilian children in the last 6 months (Boeira et al., 2012), and 7.6 % of British children in the last 4 weeks (Shepherd et al., 1999).
In adults, a meta-analysis looking at dental pain also found a high prevalence of dental pain; prevalence of toothache was estimated at between 7-32% (Pau et al., 2003), although note that the included studies were mainly from HIC. In the US specifically, it has been estimated that 12.2% of people have experienced dental pain in the last 6 months (Lipton et al., 1993).
It is possible that these rates are higher in LMIC, although there is less data from adults than children. In Tanzania, data from 1759 adult respondents from a house-to-house survey indicates that 59% of people have experienced dental pain in the last year (Kikwilu et al., 2008). In South-East Iran, a population-based survey found that 55.1% adults reported toothache in the last 6 months (Kakoei et al., 2013). Finally, a common theme is that oral pain is strongly socially stratified; individuals from lower socioeconomic classes are more likely to experience dental pain (do Carmo Matias Freire et al., 2021; Pentapati et al., 2021).
Overall, I have strong epistemic certainty that dental pain is sufficiently widespread as to be an important issue, although the exact prevalence of dental pain is very geographically variable. Estimates from LMIC—where I would expect a charity to target—vary from around 16.5% prevalence (birth cohort study of Brazilian children in the last 6 months) to 64.1% (cross-sectional survey of Nigerian children in the last 3 months), although many estimates are around the 50% mark (e.g. Kakoei et al. 2013; Kikwilu et al., 2008; Pentapati et al. 2021). Given the possibility of publication and sample bias (in particular, perhaps the birth cohort study estimate is lower because they are more successfully avoided a sample bias effect), I discount the 50% value to roughly estimate that around 30% of people in LMIC are likely to have experienced dental pain in the last year.[4] However, this would vary according to the actual location of a given intervention, and could be significantly higher.
Dental pain is severe
In addition to being common, available survey evidence also suggests that dental pain is frequently severe—especially in regions with poor access to dental treatment. I think this is unintuitive to people who (like myself) are accustomed to good oral healthcare, and who have experienced the preventative benefits of fluoride. See below:
- Of 1850 adults in South-East Iran, 55.1% reported toothache in the last 6 months. Of those who had experienced pain, 42.4% ranked the pain as being either severe or very severe, 30.8% as intermediate, and 26% as weak (Kakoei et al. 2013).
- Of 401 schoolchildren in Tubarão, Brazil (7 and 8 years old), 31.7% reported pain, of which 46% reported the pain as being severe or very severe. (de Lacerda et al., 2013)
- Of 1237 school children in Bangalore, India, 15.6% of children reported dental pain. 40% of those reported severe pain, 43% moderate pain, 17% mild pain (Saheer et al., 2015).
- Of 353 individuals at >18 attending a public homelessness shelter in a Brazilian state capital (Goiâna), 50% reported dental pain in the last 6 months, with most reporting ‘very severe’ pain. For those reporting pain, 12.9% reported auto extraction of the tooth (!) (do Carmo Matias Freire et al., 2021).
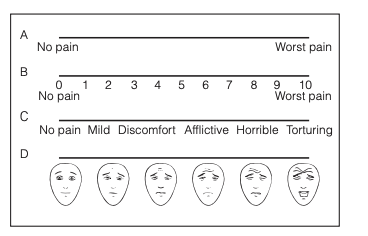
Another line of evidence comes from patients who are actively seeking dental treatment. While it might be expected that these estimates would be biased upwards relative to the general population (since the severity of dental pain in this population is sufficiently high that they sought out treatment), the results I found are broadly similar to the survey results outlined above. For example, a study in Brazil found that patients seeking treatment for toothache rated their pain at 5.2 on a 0-10cm scale before treatment, see Fig 3 [5](between ‘discomfort’ and ‘afflictive’) (Dos Santos et al., 2012). Using a similar method, researchers studying Nigerian dental patients classified mild pain when the patients marked between 1-3cm, moderate pain at 4-6cm, and severe pain at 7-10cm. Most patients suffering from pulpitis (infection of the pulp, frequently caused by untreated cavities) marked their pain as being either moderate or severe; for example, 43% of patients suffering from acute pulpitis reported their pain as being severe (Odai et al., 2015).
As far as I am aware, there are few studies available that contrast the pain intensity of different conditions. However, to give a rough sense of scale (note that pain estimates could be altered by specifics such as the wording of the question and cultural context, which I do not go into here); a report from the Happier Lives Institute found that migraines are typically rated at between 5 and 7 on analogous 0-10 pain scales, while low back pain is typically estimated at between 3 and 5 (Sharma et al., 2020). The Brazilian dental pain study listed above (which also used a 0-10 scale to assess pain severity; Dos Santos et al., 2012) places dental pain at 5.2, which is roughly between the intensity of these two conditions. Note that the estimate from the Brazilian study does not appear to be inflated relative to populations that were not actively seeking out dental treatment (e.g. since 42.4% of Iranian adults reporting dental pain judged it as being either ‘severe or very severe’; Kakoei et al. 2013).
While precise estimates of the intensity of dental pain vary, the studies that I found were all consistent with the idea that dental pain in LMIC tends to be of moderate to severe intensity (with most participants reporting pain levels in this range; de Lacerda et al., 2013; do Carmo Matias Freire et al., 2021; Kakoei et al., 2013; Odai et al., 2015; Saheer et al., 2015). I would still discount these estimates somewhat, due to publication bias and the possibility that these populations are especially extreme. In particular, I could not find many estimates of dental pain from the general adult population in LMIC. My best estimate is therefore that around 50% of the people experiencing dental pain in LMIC are experiencing moderate to severe levels of pain. Using my estimate (30%) of the prevalence of dental pain per year, this suggests that approximately 15% of people experience moderate to severe levels of dental pain per year, in the LMIC countries that a dental charity might prioritise.
In the absence of treatment, dental pain is long lasting
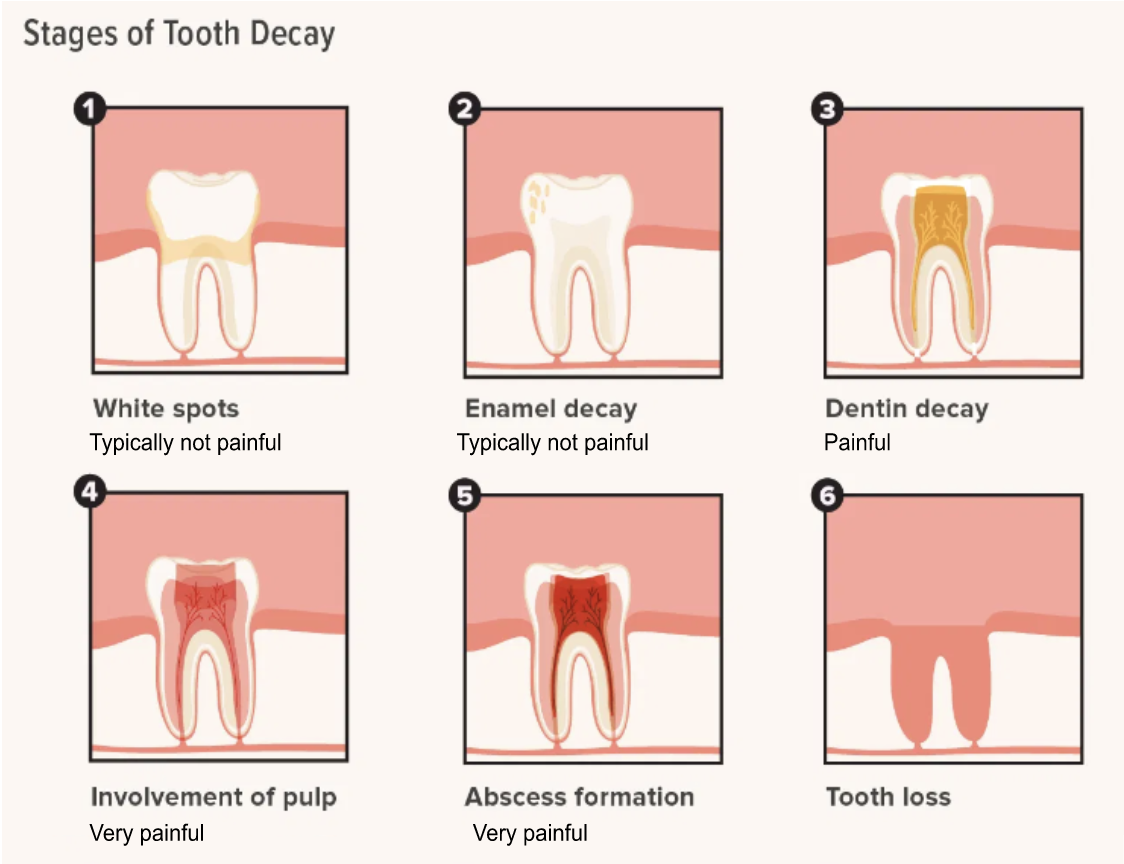
In countries with good dental care (including preventative treatments such as exposure to fluoride), dental pain is unlikely to become severe or chronic; namely because the problem will typically be rectified in time (e.g. typically at Stage 2 or 3 in Fig 4 below). Dental decay is not usually painful in the early stages, where the decay is limited to the outer areas of the enamel. If the decay persists past this point, it will reach the dentin layer of the tooth (panel 3 in Fig 4). Unlike enamel, dentin is sensitive and contains ‘tubules’– which can transmit sensations to the nerves (Fosse et al., 1992). Consequently, exposed dentin will typically result in toothaches and sensitivity to hot and cold food.
If the decay continues, the inner pulp of the tooth (where the nerves and blood vessels are) will likely be affected. When damage to the pulp occurs, it is liable to swell. Because the tooth cannot expand to accommodate the swelling, and due to the proximity of the nerves, this is usually very painful (Schwebel & Larimer, 2018). In regions with good oral healthcare, a patient with this problem would typically get a root canal treatment.
Without treatment, the bacteria from the tooth decay will often proceed to infect the pulp. This results in the formation of a dental abscess, a collection of pus. This causes intense pain, and is considered to be a dental emergency in HIC (requiring root canal or possible tooth extraction; Dental Abscess, 2017). Without treatment, the swelling will cut off the blood supply to the nerve and kill the tooth. In time, the abcess will eventually drain and pain levels will typically subside. However, at this stage there is risk of the infection spreading further—in some cases, serious complications such as septic shock can result. I could not find estimates of how frequently this occurs in the absence of treatment, but note that dental infection was continually listed as the fifth or sixth leading cause of death in the pre-antibiotic 1600s era of the London Bills of Mortality (Schweta et al. 2013).
The rate of progression from cavity to abscess can take several months or even years (How Long Does It Take For a Cavity To Develop?, n.d.). In addition, there is risk of the infection spreading to adjacent teeth—essentially restarting the process. Consequently, in the absence of treatment it is reasonable to describe dental as chronic (lasting longer than 3 months).
Pain affects wellbeing
The relationship between pain and wellbeing is not well-understood, and I could not find any data regarding the relationship between dental pain and wellbeing specifically—making this section necessarily speculative.
However, as we might expect, pain impacts upon wellbeing (e.g. Sharma et al., 2020). A recent report (requested by Founders Pledge from the Happier Lives Institute), conducted a literature search and associated analysis to examine the relationship between pain and wellbeing. The authors estimate that having any chronic pain condition results in a decrease in life satisfaction of approximately 0.2 points, on a 0-10 scale (Dupret & Guire, pending publication). However, they note that that this may be an underestimate; for instance, because the estimate doesn’t include spillover effects (effects on people other than the person with chronic pain—an example could be feeling less satisfied with one’s own life, because a partner or household member is suffering from chronic pain) and because some estimates of chronic pain attribute wellbeing effects towards intermediary conditions that chronic pain ultimately causes (e.g. depression).
The Happiness Research Institute estimates that the process of moving from no pain to chronic pain rated at 2.5 (out of 10) correlates with a decrease in life satisfaction of approximately 0.5 points out of 10, based upon a large European dataset of over-45s (Happiness Research Institute, 2020).
Given the reasoning I outline in the ‘Dental pain is longlasting’ section, I think it is reasonable to treat dental pain (in areas with poor access to dental care) as chronic. Hence, I use estimates of the effect of chronic pain upon wellbeing to get at the wellbeing effect of dental pain. However I include a large discount (80%) to account for the fact that some dental problems (such as milder gum disease) may resolve on their own, and to account for the fact that the pain might be relatively mild to begin with. In the absence of data about the progression of dental pain in areas with very limited dental treatment, I am highly uncertain of this value—this could be generating a significant underestimate of the wellbeing impact of dental pain.
On average, I therefore assume (for the CEA) that dental pain (for people with extremely limited dental access) reduces life satisfaction by 0.07 WELLBYs; that this person’s life satisfaction is reduced by 0.07 points out of 10 for one year. This is very rough: I took the average wellbeing effects across both the Happier Lives Institute study and the Happiness Research Institute study (0.35) and discounted by 80% to account for the fact that some dental problems may spontaneously resolve/ will be less painful at early stages.
Loss of income and other economic impacts
There is a small literature concerning the relationship between dental pain and work productivity. However, these effects were smaller than I anticipated. For example, a nationwide study in Canada indicated that dental-related issues resulted in an average of 3.5 hours of lost working time per person per year (Hayes et al., 2013). Among workers working in meat processing/ slaughter in Brazil, the average number of lost working hours as a result of dental causes was 0.88 per employee per year (Nardi et al., 2009). I could not find any data from low income countries, so it is possible that the effect there is somewhat stronger than these datapoints suggest—but overall, I expect these economic benefits to be relatively small compared to the wellbeing benefits of avoiding pain.
Another source of economic impact comes from the cost of dental treatment. Out-of-pocket payments are the primary source of healthcare financing in many countries (McIntyre et al., 2006). There is some evidence that links out-of-pocket payments for dental care to catastrophic dental health expenditure (i.e., spending so much upon dental healthcare treatment that basic household necessities can no longer be afforded). However, it is higher-income countries where dental spending is more likely to result in catastrophic expenditure; 50% of surveyed upper-middle class countries had at least 1% of households facing catastrophic dental health expenditure, but only 11% of low income countries had at least 1% of households facing catastrophic dental health expenditure (Masood et al., 2015).
One consideration is that in some countries, dental costs might be low because there is extremely limited access to dental care (e.g. people in these regions would spend money on dental care if they could). It is striking that a substantial minority of households in upper-middle income countries will voluntarily undergo catastrophic expenditure in order to receive dental treatment—the fact that people will undergo these costs highlights the severity of suffering caused by dental problems.[6] Overall, this suggests that while there may be some economic benefit to providing enhanced dental care in LMIC, the wellbeing benefits are dwarfed by those stemming from avoiding pain.
Missed School
It has been argued by a number of authors that poor oral health results in reduced school attendance (e.g. Guarnizo-Herreño & Wehby, 2012; Jackson et al., 2011; Krisdapong et al., 2013). Estimates from a systematic review suggested that children with one or more decayed teeth have a higher probability of poor school performance (OR: 1.44, 95%CI 1.24-1.64) and of a poor school attendance (OR: 1.57, 95% CI 1.14-1.57) compared to caries-free children (Rebelo et al., 2019). However, all the included papers were observational (with only one longitudinal study) and as such was limited by confounding factors—only 61% of the studies accounted for socioeconomic status.
Some of the best data is from the US. While adjusting for socioeconomic and demographic factors, data from 45711 children (from the 2016-2017 National Survey of Children’s Health) indicates that children with oral health problems were more likely to have problems at school (OR: 1.56, 95% CI 1.32-1.85), and to miss more than 6 school days (OR: 1.39, 95% CI 1.14-1.69) (Guarnizo-Herreño et al., 2019). I could not find data from LMIC to assess this relationship in lower income countries specifically—given that the pain from oral healthcare is less likely to be adequately managed in LMIC (presumably a mitigating factor in the US), I would predict that the relationship is stronger. However, I also suspect that there are likely to be some unmitigated confounding factors in the US data.
Overall, it seems likely that improving dental healthcare would have a small positive effect upon school attendance. However, the consequent effect upon wellbeing is likely to be small; while children with slightly better school attendance might have slightly improved lifetime earnings (and consequent improved wellbeing), it seems likely that this effect would still be small in comparison to the more direct impact of avoiding pain upon wellbeing.
Development
There is also some evidence that childhood caries (i.e. caries in milk teeth) impact upon nutritional status. One possibility is that this relationship is bidirectional; malnutrition can increase the likelihood of caries via the development of especially thin enamel (dental hypoplasia), and from poor development of the salivary gland (Psoter et al., 2008). At the same time, caries may also predispose individuals to malnutrition. In particular, the pain caused by caries may make it difficult to eat, and may result in patterns of chronic inflammation that affect normal growth (Sheiham, 2006).
However, a quick review of this shows that the evidence is mixed. While some studies have found evidence that children with more caries are more likely to be underweight (Oliveira et al., 2008; Sheiham, 2006), others haven’t found an effect (Kumar et al., 2017; Muhoozi et al., 2018), or even find that children with more cavities tend to be larger (van Gemert-Schriks et al., 2011). A recent meta-analysis concluded that dental caries are a risk factor for malnutrition, and the severity of caries are associated with being underweight and growth stunting–but that the ‘overall quality of the data was low’ and that ‘the impact of caries rehabilitation on the growth trajectories of nutritionally vulnerable children from low- and middle-income countries remains to be determined’ (Tanner et al., 2021).
Given how mixed the data is (Tanner et al., 2021), I suspect that the causal link between cavities and malnutrition in children is fairly weak, if it does exist. One possibility is that the associative link between dental caries and malnutrition is better explained via the effects of malnutrition upon caries (e.g. Psoter et al., 2008), rather than the other way round. Experimental evidence from LMIC (e.g. testing whether treating cavities in underweight children results in weight gain) would be very helpful, but I couldn’t find data of this nature. Overall, there may be some positive effects gained by treating the worst-affected children (aka who are more likely to have the kind of severe dental pain that could impact eating), but I don’t think this is likely to be a strong effect for the majority of children.
Impacts from associated disease risk
Poor oral health has been linked to a variety of health conditions including heart disease, stroke, diabetes and rheumatoid arthritis. In short, the theory is that poor oral health allows bacteria from your mouth to enter into the bloodstream—causing downstream effects such as heart disease (Your Teeth and Your Heart, n.d.). A key question is whether the presence of cavities is indeed causally related to the development of these conditions: if so, oral health interventions may be even more impactful than previously assumed. Many of the links between cavities and other diseases operate through tooth loss (aka tooth decay causes tooth loss, which is a risk factor for CHD) or other factors such as periodontitis (see Fig 5). Overall, I estimate an ~40% chance that poor oral health is an independent risk factor for these conditions (increasing the chance of developing these diseases by ~15%)—evidence outlined below.
Heart disease
Several observational studies have reported a link between poor oral health (such as presence of caries) and coronary heart disease (CHD) (Vedin et al., 2015). However, it has been difficult to pull out whether this relationship is causal, primarily due to confounding factors in observational studies such as smoking/ excess sugar.
A number of observational studies have found a moderate relationship between poor oral health and heart disease, while adjusting for other factors (Humphrey et al., 2008; Larvin et al., 2021; Leng et al., 2015). A meta-analysis from 2004 found a 20% increased risk of CVD with periodontitis (Meurman et al., 2004). This value is in line with other estimates, for example that periodontitis is associated with a 22% increased risk of hypertension– a strong risk factor for CHD (Munoz Aguilera et al., 2020). However, other studies have found that this relationship may be better explained by confounding variables such as smoking, including an exceptionally large cohort study (Batty et al., 2018).
Given this ambiguity, I looked at papers examining the proposed biological mechanism for this effect. There are mechanistic reasons to think there might be a causal relationship between oral health and heart disease. Dental caries may adversely cause chronic inflammatory responses in the endothelial coronary cells of the heart, through bacterial invasion from decayed teeth (causing endocarditis). That is, bacteria from infected gums spread to the inner lining of the heart, causing inflammation. A second potential mechanism is that bacteria can spread from the mouth into the bloodstream, and travel to the arteries—where they harden, causing atherosclerosis. Animal and cell culture experiments have lended significant support to these ideas: e.g. mice who are experimentally infected with S. mutans (a bacteria common to cavities) exhibit thicker arterial plaques, at least if they already have arterial injury (Kesavalu et al., 2012). There is also evidence that patients with poor oral health have raised inflammatory levels, aka high levels of C-reactive protein [7](Paraskevas et al., 2008).
As an additional note, if oral health does act as an independent risk factor for CHD, there is some reason to expect that effects upon CHD might be greater in LMIC than HIC. The reason for this is that rheumatic heart disease rates are far higher in LMIC (Rheumatic Heart Disease, n.d.); affecting approx. 5.7 children per 1000 children in Sub-Saharan Africa in 2005 (Mayosi et al., 2014). People who survive rheumatic fever frequently have lasting disease to their heart valves, and are more susceptible to infective endocarditis—an inflammation of the heart valves which can be caused by oral bacteria (Maharaj & Vayej, 2012; Quach & Wray, 2020).
Overall, I find this evidence suggestive of a possible causal link between cavities and heart disease. However, the large meta-analysis by Batty et al. (2018)—which suggested that smoking was a key variable that could potentially explain the CVD/ oral health link—pushed my estimate down. I estimate a ~40% likelihood that poor oral health is an independent risk factor for CVD.
Stroke
There has also been some work arguing that periodontal disease increases the risk of stroke. Frequent tooth brushing is negatively associated with risk of stroke occurrence (HR: 0.78, 95% CI: 0.73-0.84), and no. of dental caries (≥4) is positively related to stroke occurrence (HR: 1.28, 95% CI 1.13-1.44) (Chang et al., 2021). This is from a cohort study with 206,602 participants. I also found evidence for poor oral health as an independent risk factor for stroke in a few other studies (Alhadainy et al., 2021; Grau et al., 2004)—although I didn’t find the same volume of meta-analyses as I found for CHD. While there haven’t been extensive studies on the potential mechanism behind this effect, it has been proposed that oral disease can increase the risk of stroke through similar mechanisms as for CHD; e.g. by increasing rates of systemic inflammation (Sen et al., 2018), which could cause build up in the blood vessels and increase likelihood of a stroke-causing clot. I’d suggest a similar 40% likelihood of a causal link between oral health and stroke; while the evidence thus far is quite suggestive (and not as contradictory as the CHD evidence), there are not as many studies.
Type 2 Diabetes
The relationship between type two diabetes and poor oral health seems to be somewhat bidirectional, making it challenging to estimate the effect of poor oral health upon type 2 diabetes specifically.
This is because high blood sugar (from uncontrolled diabetes) adversely affects oral health. That is, high blood sugar can cause high levels of glucose in saliva and very dry mouths—given that saliva usually has a preventative effect upon cavity formation, this increases the risk of tooth decay. At the same time, painful/ missing teeth may result in a poorer quality diet, thereby potentially increasing the likelihood of the development of type 2 diabetes (Borgnakke, 2019). For patients with periodontitis, the relative risk of developing diabetes was elevated by 26% (Stöhr et al., 2021); this result comes from a recent and large meta-analysis. While most prior work has focused on the causality between diabetes and cavities (i.e. less control of blood sugar = more cavities), these results do not ‘disagree’ with prior results in the same way that the heart disease evidence is contradictory.
I’d suggest a 50% likelihood of a causal link between oral health and diabetes—although I suspect the relative risk of diabetes development (given that this link does exist) may be lower than current estimates suggest (i.e. due to publication bias).
Noma
Noma is a neglected tropical disease (campaigning for the WHO to officially recognise it as such is ongoing; (Noma: A Preventable but Neglected Disease | RSTMH, n.d.) that is most common in sub-Saharan Africa for children living in extreme poverty. It is a necrotizing disease that destroys the tissues of the mouth and face, frequently resulting in sepsis. There are about 140,000 cases each year (World Health Organization. Regional Office for Africa, 2016), and it is very severe: 85% fatal when untreated.[8] In addition to having a very high mortality rate, noma is a highly stigmatised disease that (when a person survives it) results in lifelong disfigurement: survivors often face difficulty talking and breathing, and frequently suffer social isolation (Srour et al., 2017).
Would dental health interventions help decrease rates of noma? It is difficult to answer this question, because the etiology of noma is very poorly understood. However, the early stages involve gingivitis, which proceeds to a very aggressive form of gangrene—one possibility is that these gangrenous bacteria enter through oral lesions caused by gingivitis (Whiteson et al., 2014). Hence, it is possible that improving oral health would decrease rates of noma.
At the same time, having a dysregulated immune system (for example, due to concomitant disease such as HIV and malaria) seems to be key to the development of this disease (Farley et al., 2018). As a disease of extreme poverty, there seem to be many factors at play (such as oral health, plus immune system irregularities, proximity to livestock, etc): it could be the case that once these other factors are in place, it is a case of ‘when’ not ‘if’ bacteria takes hold. Under this scenario, improving oral health would not significantly decrease rates of noma.
Overall, I think it is likely that improving oral health would somewhat decrease rates of noma. However, unfortunately I think this effect would likely be small—due to the importance of other risk factors beyond oral health. For particular initiatives (i.e. training up local dentists in very rural areas, who can also be trained to provide antibiotics to treat noma) this effect could be more substantial.
Chance that this problem will get bigger in future
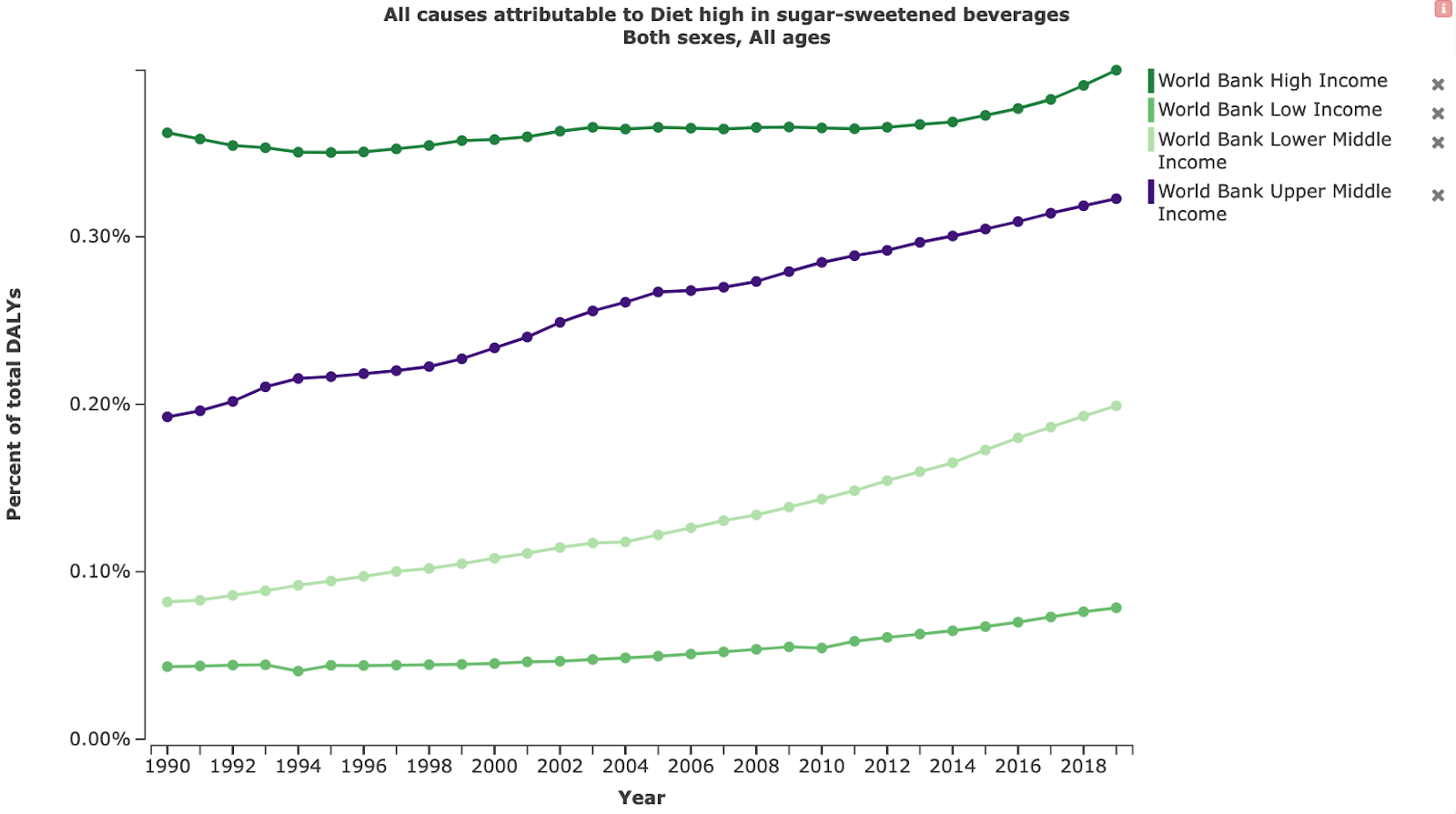
It seems very likely that oral health problems will become a more significant problem in the future, in LMIC. This is because LMICs are likely to undergo the ‘nutrition transition’ that most HIC have already experienced (Reardon et al., 2021); a shift in diet marked by an increase in sugary, fatty and less fibrous foods. In HIC, this has coincided with an increase in various non-communicable diseases, including dental caries (Ronto et al., 2018); see Fig 6.
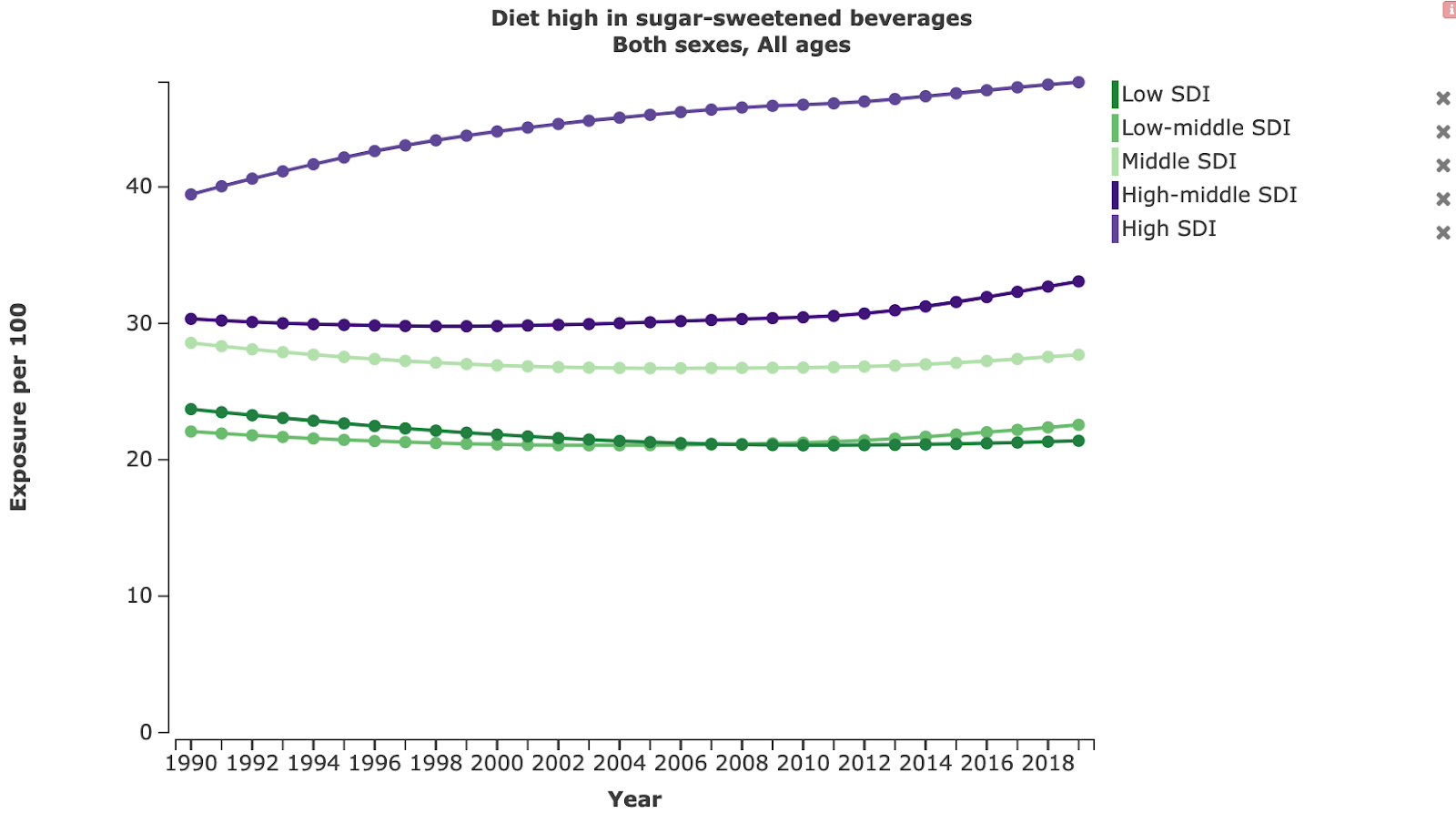
In most LMIC, sugar consumption is still low compared to HIC (see Fig 7). However, there is evidence that this will change in the future. First, we might expect LMIC to follow the general pattern that other countries have experienced, whereby countries that undergo economic development experience subsequent rises in non-communicable diseases (Reardon et al., 2021). For example, in China rates of childhood caries increased from 27% in 2005 to 37.92% in 2015 (Li et al., 2021). Second, there is evidence that ‘key players’ in the global sugar industry are switching their focus to LMIC; according to information from 2019, Coca-Cola set aside $12 billion for marketing their products in Africa by 2020, and PepsiCo set aside $12 billion for its operations in India until 2020 (by contrast, the entire WHO budget for 2017 was $4.4 billion) (Peres et al., 2019). Finally, consumption of sugar-sweetened beverages is rising most quickly in LMIC (Popkin & Hawkes, 2016).
For these reasons, I think it is very likely that oral health problems will increase in the future in LMIC, as diet shifts towards being higher in sugar (95% certainty). However, I am unsure about how quickly this will happen; note that sugar intake still appears to be significantly lower in LMIC than HIC. Putting preventative measures prior to this increase in sugar intake would decrease suffering from dental pain; i.e. see CEA. The CEA uses current rates of dental problems, and the interventions become even more cost-effective with higher rates of dental problems in the population.
Neglectedness
Is dental health neglected relative to other forms of healthcare?
A number of researchers have made the claim that dental healthcare is neglected, relative to other forms of healthcare (Benzian et al., 2011; Watt et al., 2019). There are several features of dental health that are thought to have contributed towards this:
- Relative to other forms of health, dental ill health is unlikely to have a significant effect upon mortality—although it can be debilitating. Many health initiatives focus upon reducing mortality, rather than improving wellbeing.
- Dental healthcare is often poorly linked to existing healthcare systems (e.g. Benzian et al. 2011; Watt et al., 2019).
- Historically, most dental treatment in HIC has focused upon curative treatment—which is expensive, and often unaffordable for LMIC (e.g. Watt et al., 2019).
While these arguments about why dental health may be neglected are quite strong, it is harder to find empirical evidence testing this. One way to do this is to look at oral healthcare spending versus other forms of healthcare spending, but it is difficult to find estimates of oral healthcare spending from LMIC. In Europe, it’s estimated that countries spend between 6-10% of their national health budgets upon oral care (Kandelman et al., 2012): given that oral health accounts for approximately 0.9% of global DALYs (GBD Results Tool | GHDx, 2019), this does not appear to be underfunded. However, in LMIC there is some evidence that the proportion of the health budget spent upon oral healthcare is lower—in Nigeria, approximately 0.41% of the healthcare budget was spent on oral healthcare from 2006-2010 (Adeniyi et al., 2012).
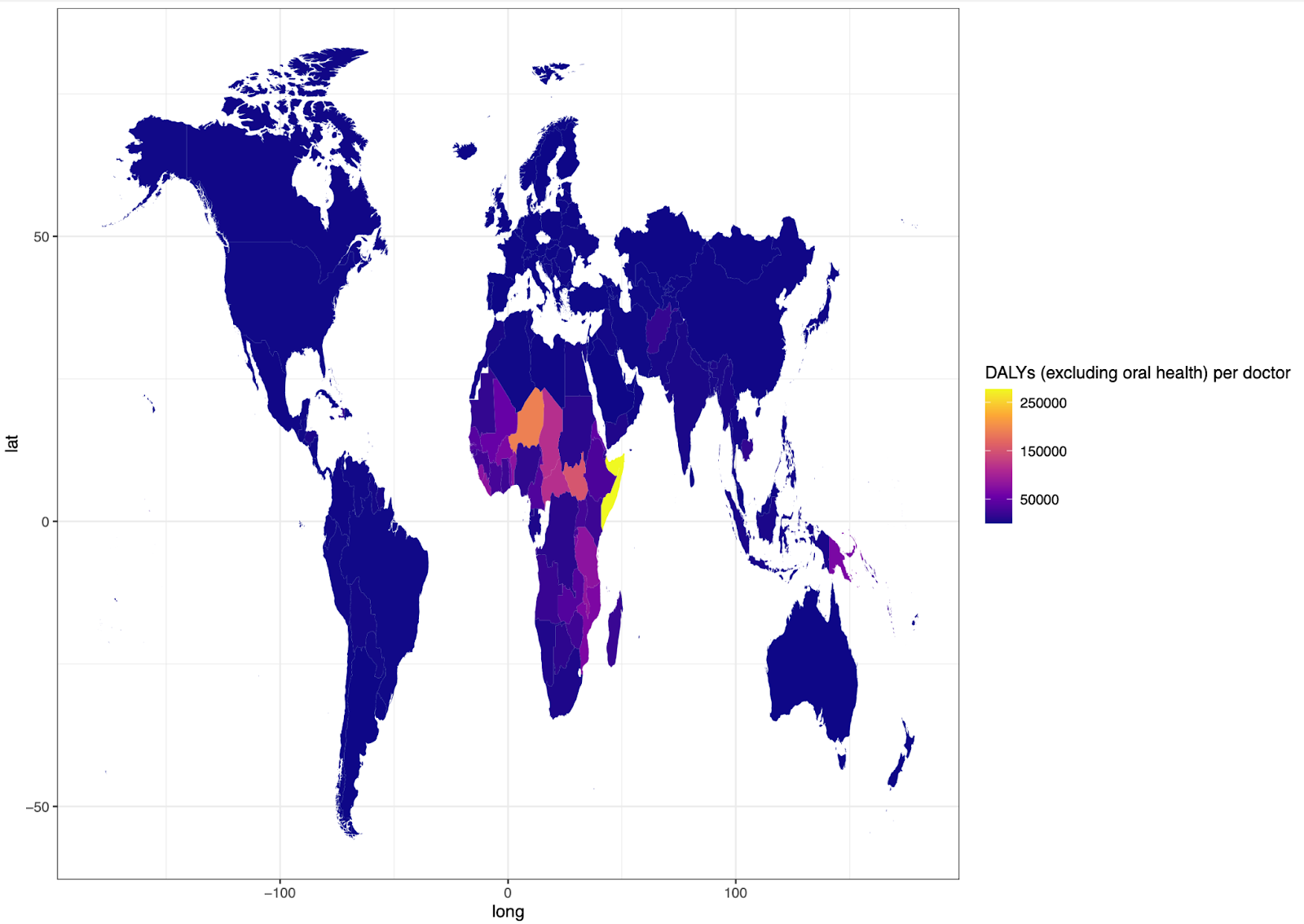
As a very rough proxy for investment into oral health, I therefore used WHO data on the ‘number of dentists per 10,000 of the population’ (GHO, n.d.): there is available data on this metric from LMIC. I used this data alongside measures of disease burden from the Global Burden of Disease Project (2019), to examine the number of relevant healthcare professionals per DALY of disease. If dental care is neglected, then the ‘Number of dentists per DALY from oral health disease’ (see Fig 6) should be less than the ‘Number of doctors per DALY from all diseases (excluding oral health)’ (see Fig 7). In reality, the ratio of ‘DALYs (excluding oral health) per doctor’ was higher in all countries than the ‘Oral health DALYs per dentist’ ratio.
However, I think there are a few crucial caveats. First, oral health is expected to get worse in LMIC as they go through the nutrition transition (Reardon et al., 2021). This means that the current GBD estimates of oral health burdens are likely underestimates for LMIC, when looking to the future. Second, as I argued in the ‘Pain’ section (and below in the ‘Is the burden of dental pain underestimated?’) oral diseases are given quite a low weight in the GBD measures. For example, toothache is given a weighting of 0.01, the same weighting as mild acne (GBD Results Tool | GHDx, 2019): this might be correct in some cases, but the pain ratings that I found in the ‘dental pain is severe’ section placed the pain at a similar level to migraine pain (which has a disability weighting of 0.441). There also doesn’t seem to be a separate weighting for severe forms of toothache (such as pulpitis). See section below for further discussion of DALY weightings as applied to dental health.
Finally, note that many of the causes of oral health DALYs (such as cavities: see Fig 1) are treatable/preventable via dentistry and use of fluoride—other leading causes of DALYs, such as stroke and ischemic heart disease, are not as easily curable. This suggests that oral health may be neglected relative to its tractability (which I examine further in the Tractibility section).
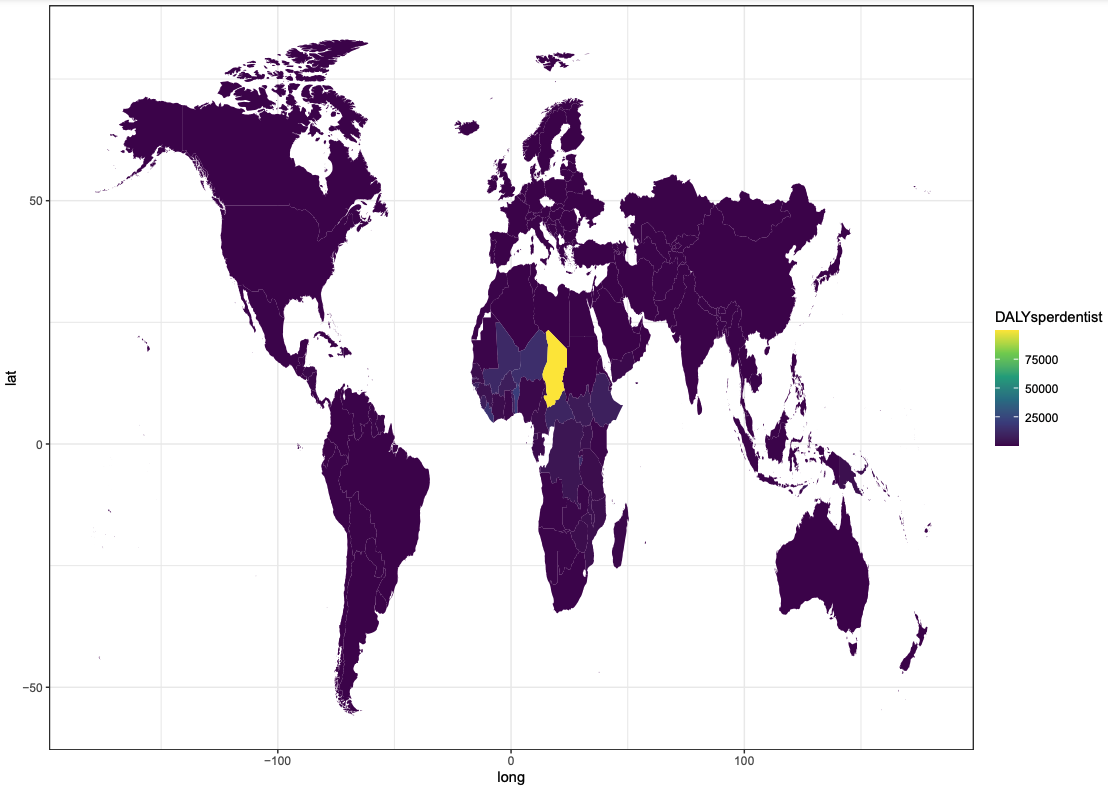
Taking this together, I think it is unlikely that oral health is drastically underfunded on a global level. However, given that (1) GBD estimates might be an underestimate of dental pain severity; (2) the nutrition transition will likely enhance existing international inequities in oral healthcare and; (3) there seems to be huge regional differences in the ratio of oral health DALYs to dentists (e.g. Fig 8 suggests that this ratio is especially high in Chad), it is still plausible that oral healthcare specifically in LMIC may be neglected—which I examine in the next section.
Is the burden of dental pain underestimated?
DALYs are currently the only metric that can provide global estimates of the burden of oral health; other metrics (that are specific to wellbeing) such as WELLBYs have unfortunately only been utilised for a small subset of conditions, in particular populations. For these reasons, I have used DALYs to get an overview of the importance and neglectedness of oral healthcare– even though this report is focused upon wellbeing impacts.
I think there are several reasons to suspect that DALY weightings of oral health are underweighted when applied to wellbeing. To lay this out clearly, I will recap how a DALY is calculated. A DALY represents the loss of an equivalent of one year of full health, and is the sum of the YLL (years of life lost) due to premature mortality, and the YLD (years lived with disability) due to the condition in question.
For example, a DALY estimate for the burden of dental caries in Kenya would be as follows:
DALY (caries in Kenya) = YLL (caries in Kenya) + YLD ( caries in Kenya)
While the YLL metric relies upon estimates of the years of life lost due to caries, the YLD also attempts to capture the health-related impact of living with the disease (beyond mortality). This is captured by the disability weight;
YLD (caries in Kenya) = disability weight (caries in Kenya) X prevalence (caries in Kenya)
Note that the estimate of the severity of oral health conditions is especially sensitive to any errors in this disability weight, because it is relatively rare for oral health conditions to result in premature mortality—their impact is primarily felt through the suffering they cause during the lifespan.
Disability weights are constructed by surveying thousands of people in the general population whether they think that person A (who has a particular condition) is more or less healthy than person B (who has a different condition). These pairwise comparisons are then used to generate the disability weights of each condition, using the probability that a given condition is selected as ‘less healthy’ than another given condition (Salomon et al., 2012).[9]
There are several reasons that these preferential comparisons might underweight the burden of dental conditions with regards to wellbeing (alongside other chronic pain conditions, and mental health disorders). To the best of my understanding, while a number of surveys took place in LMIC, the majority of the people who undertook these surveys were in Europe and completed the surveys over the internet (e.g. Salomon et al. 2015). These groups are especially likely to have access to good curative dental care, and to have experienced preventative benefits from fluoridated water and toothpaste. Therefore, they may have experience with mild toothache (e.g. caused by minor enamel decay) but are less likely to have experiences with severe dental pain. Consequently, the impact of severe dental disease may be underestimated.
Second, people’s conception of ‘health’ obviously encompasses aspects other than wellbeing. For example, people might define health as ‘how close to death is this person?’ Diseases that exhibit their effect via wellbeing (as opposed to mortality) will likely have a lower DALY estimate. This poses a problem, when we are trying to get estimates of the impact of different diseases upon wellbeing—it is important to have some measure which can provide an overview of the global impact of different diseases, but measures that are specific to wellbeing (such as WELLBYs and WALYs) have thus far only been estimated for a relatively small subset of conditions in particular locations.
Finally, preferences are subject to cognitive biases (e.g. Kahneman et al.,1982) that may skew estimates. In particular, we are poor judges of ‘hedonic adaptation’ or our ability to return to our baseline level of happiness. There is evidence that humans exhibit considerable adaptation (returning to their baseline happiness level) in response to physical illness (e.g. Graham et al., 2011; Tyc, 1992), but there is some evidence that we do not experience the same degree of adaptation towards chronic pain (Graham et al., 2011). Therefore, chronic pain from dental problems may be underweighted in terms of impact relative to physical health conditions.
Taken together, I think it is highly likely that DALY scores systematically underestimate the burden of these disorders when we are trying to capture wellbeing impacts.
Availability of dental care in LMIC
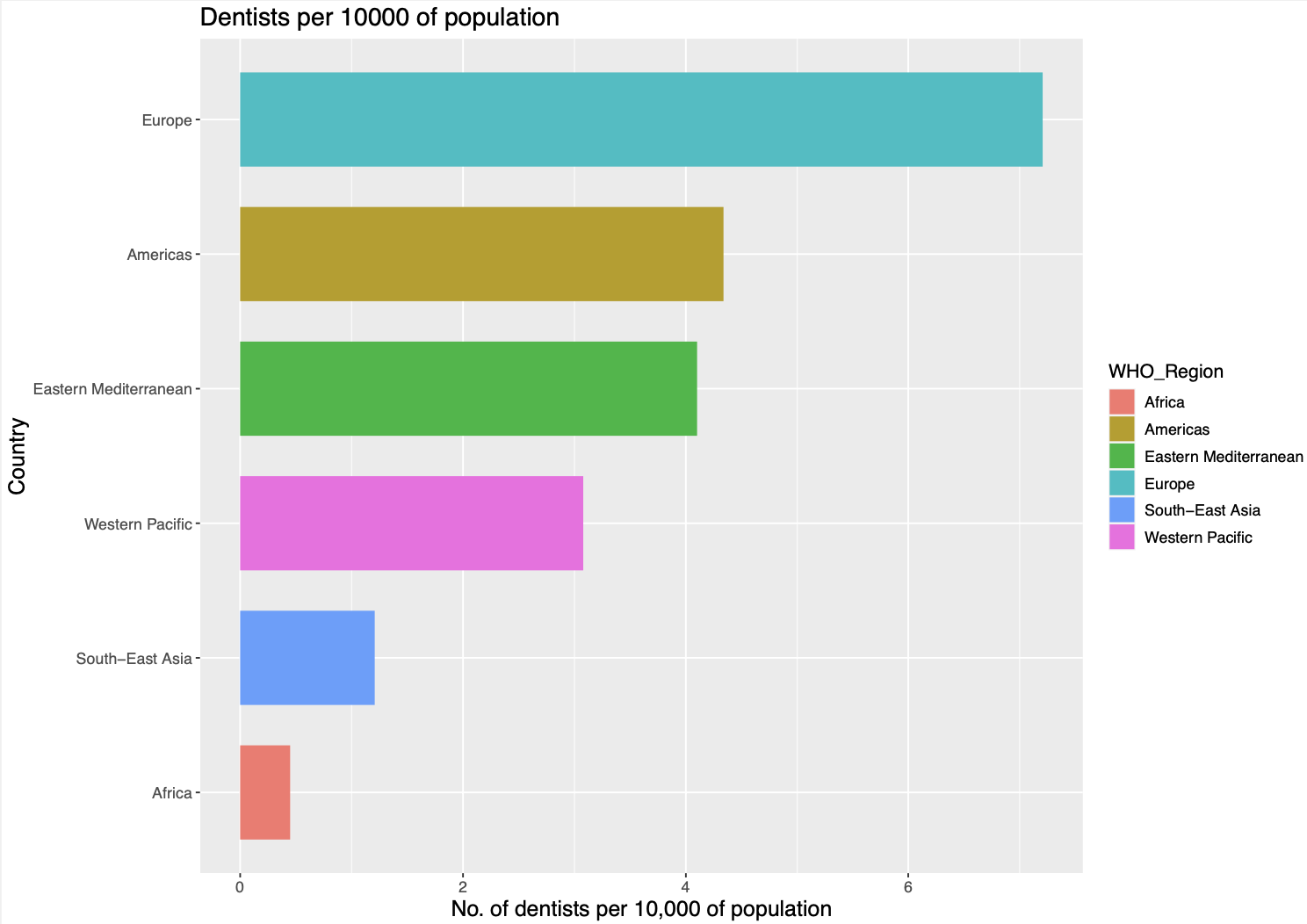
There is huge variation in the number of dentists by country; WHO data indicates that Chad has 3 dentists, while Belgium (which has a smaller population size than Chad) has 12,751 dentists (GHO, n.d.). The full dataset is displayed as the ‘Number of dentists per 10,000 population’, in Fig 10: the countries with the fewest dentists per capita are mainly in sub-Saharan Africa.
While this suggests that many countries in sub-Saharan Africa are especially under-resourced for dental care, an important point is that dental health in LMIC is often estimated to be superior to that of HIC. This is partially because HIC have undergone the ‘nutrition transition’ (Reardon et al., 2021); a shift in diet marked by an increase in sugary, fatty and less fibrous foods. In addition, some researchers argue that the natural levels of fluoride in some regions (such as the Great Rift Valley of East Africa) protect many Africans from dental caries (Petersen et al., 2005). It could therefore be the case that oral healthcare is less under-resourced in LMIC than this data suggests.
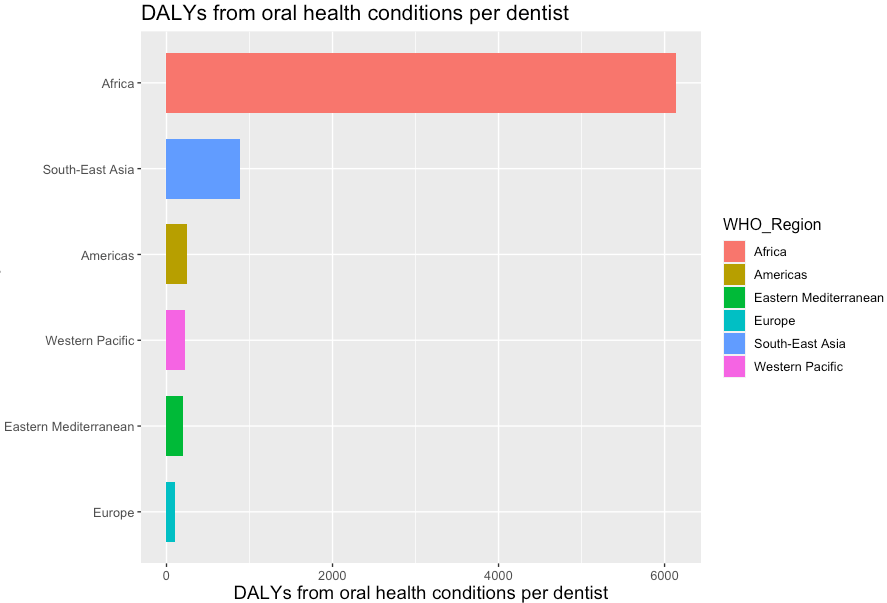
To test this idea, I graphed out the number of DALYs [10] caused by oral health conditions (GBD Results Tool | GHDx (2019), n.d.), divided by the number of dentists per country (both measured as per 10,000 of the population); see Fig 11. Importantly, many sub-Saharan African countries still have the fewest dentists per DALY. This suggests that these countries are indeed under-resourced for dental care, despite a lower incidence of dental caries relative to HIC countries.
Current work in this area
I think that dental healthcare has somewhat ‘fallen through the cracks’ between different funding bodies, and that there is not enough current work in this area. On the one hand, dental health is not strongly associated with mortality—which has the effect of lessening its perceived impact when measured in DALYs (even if the effects on wellbeing are significant). This may have the result of making dental healthcare less appealing to groups such as the WHO who utilise DALY estimates. That’s not to say that there is no action from the WHO: they approved a Resolution in 2021 that recommends shifting from a curative approach to a more preventative approach, and they aim to create an action plan in 2023 with targets to achieve by 2030 (World Health Organization, n.d.). However, I could not find actual data on increased funding.
At the same time, dental care itself is quite expensive—making it less exciting to groups that are focused upon cost-effectiveness, although preventative treatment can be very cost-effective (see CEA). Finally, there are not good estimates about how the intensity of dental pain impacts upon wellbeing—my own estimate is rough. This has the effect of making it more difficult to justify funds to this cause area. Accordingly, I could not find any evidence of funding from effective altruist organisations. In general, there are also relatively few oral health charities (that I could find) that seem to be focused upon cost-effectiveness—although I did find some possibilities, which are outlined below.
Tractability
What could a philanthropist do?
Fluoridation
Fluoride binds to tooth enamel, acting to strengthen it. According to the WHO, inadequate exposure to fluoride is one of the primary reasons for the prevalence of oral disease in LMIC (Oral Health, n.d.)
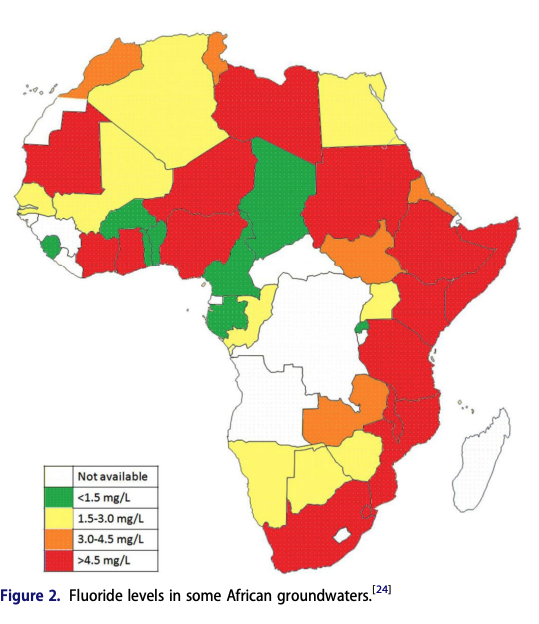
An important point is that while too little exposure to fluoride is associated with dental caries, it is also possible to have fluoride exposure that is too high—which can result in a condition called dental fluorosis, where teeth become weakened. Cases of high fluoride levels in groundwater have been reported in almost all of the sub-Saharan Africa region, but it is more prevalent in East African countries, Sudan and South Africa (Onipe et al., 2020). For example, of the top ten countries that I identified as having neglected oral healthcare, Niger, Mali and Ethiopia all have groundwater with a concentration >1.5mg/L (See Fig 12; Onipe et al., 2020). At this level, fluoride is linked to fluorosis—meaning that in these regions, a program that increases fluoride exposure would likely be deleterious. Consequently, my best understanding is that the following interventions in this section would only work in regions with low groundwater fluoride.
Improve access to fluoride toothpaste
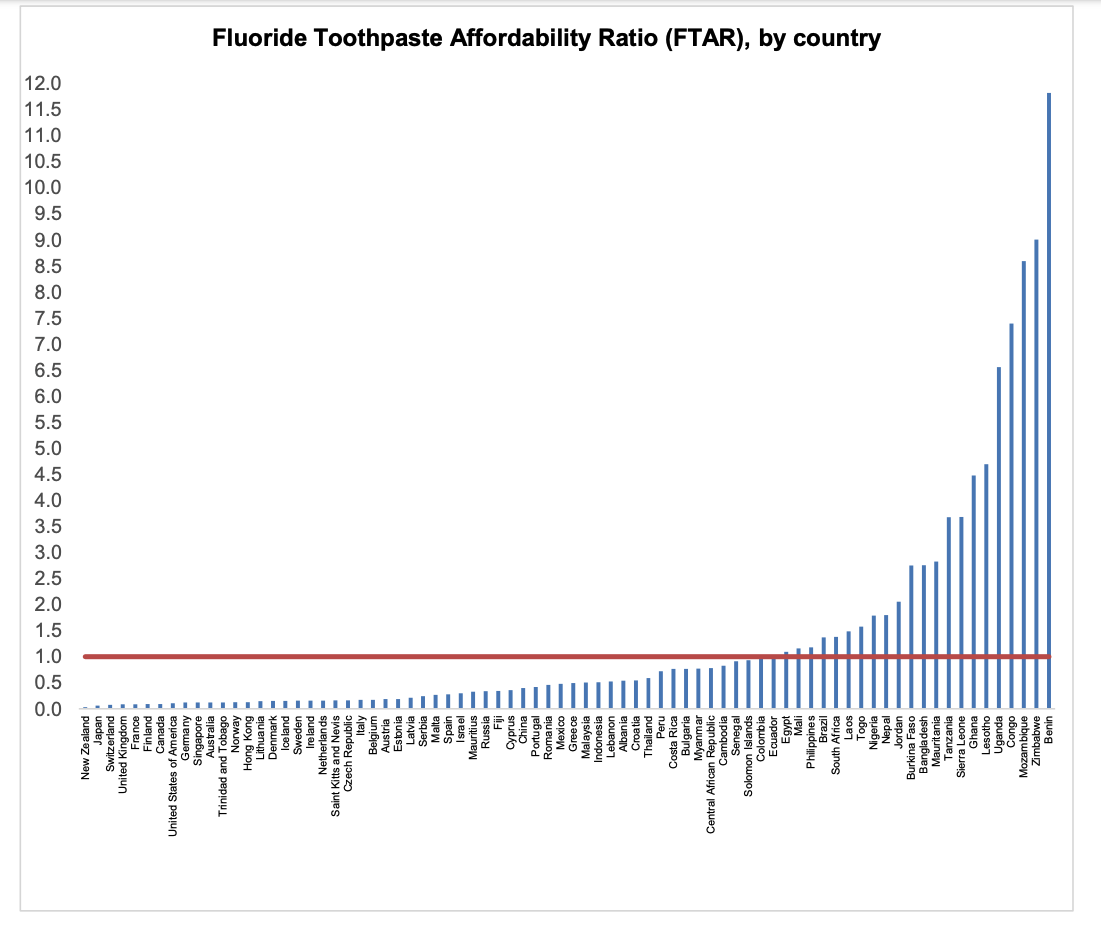
Fluoride toothpaste is considered to be a main contributor to the decline in dental caries observed among people of industrialized countries, but it is not universally used due to cost (Petersen & Ogawa, 2016). In the UK, a year's supply of toothpaste costs 0.037 days’ worth of household expenditure for the poorest 30% of households—yet is 10.75 days’ worth in Kenya (Goldman et al., 2008). A recent preprint (note: this study has not yet gone through peer review) calculated Fluoride Toothpaste Affordability Ratio as the price associated with the recommended annual consumption of fluoride toothpaste, relative to the daily wage of the lowest-paid unskilled government worker (so ratio > 1 = unaffordable spending on fluoride toothpaste.) Fluoride was strongly affordable in high-income countries, and strongly unaffordable in lower middle-income and low income countries (see Fig 13.)
This suggests that there could be significant benefit towards improving access to fluoridated toothpaste, for example by subsidising its cost. One caveat is that individuals from many countries where toothpaste is unaffordable nonetheless gain some of these benefits from using chewing sticks. These sticks work via mechanical plaque control by the friction between plant fibers and tooth surface, and by chemical plaque control due to the composition of the stick (Dahiya et al., 2012). These chewing sticks appear to be highly effective in reducing dental caries (Ezoddini-Ardakani, 2010; Halawany, 2012; Nordin et al., 2020), although it is unclear how effective they are relative to toothpaste (Ramli et al., 2021).
Overall, this intervention is promising because it could be highly cost-effective: toothpaste is relatively cheap, and extremely effective at reducing dental caries. On the other hand, the degree to which people would benefit is unclear—many of the benefits from toothpaste may already be attained via the use of chewing sticks. In addition, I could not find any relevant charity doing this kind of work.
Water fluoridation
The CDC states that water fluoridation is one of the ten greatest public health achievements of the 20th century (CDC, n.d.). For example, in a recent study with Lithuanian adults, Water fluoridation is associated with a 15-33% decrease in the proportion of decayed/ missing/ filled tooth surfaces (Stangvaltaite-Mouhat et al., 2021).
A critical problem with this possibility is that many of the countries that appear to be most neglected for oral healthcare (such as Chad, Benin, Burundi, Liberia, Niger, Mali, etc.) do not have high levels of piped water coverage. In 2015, Sub-Saharan Africa had a 24% piped water coverage (17% in rural areas, 56% in urban areas) compared to a 94% coverage in Europe and North America (Hope et al., 2020). This would limit the intervention’s effectiveness, especially given that the rural regions are often those with the strongest need for improved dental healthcare.
Nonetheless, this intervention might work in some areas (such as Serbia) where there are significant oral health problems as well as piped water coverage. In other cases, adding fluoride to salt or milk might work better.
Milk fluoridation
Milk fluoridation schemes have been launched in at least ten different countries, usually aimed at children (Székely et al., 2007). They have sometimes been launched where there is an existing school milk program.
One of the best-known examples of this comes from Chile. More than 70% of Chileans benefit from fluoridated water, but this is restricted to urban and semi-urban areas (Chile | The Borrow Foundation, n.d.). In order to counter this gap in coverage, a government-affiliated program began providing free fortified milk to children under the age of six. Compared to a control group who did not receive the fortified milk, the children who were part of this program had significantly lower dmft (41% decrease in number of decayed, missing or filled teeth)—although note that this study was not fully randomised (Mariño et al., 2001). A Cochrane review from 2015 estimates this effect at 31% decrease in dmft primary teeth, but they note that the available evidence is low-quality (Yeung et al., 2015).
Advantages of this intervention include the fact that it is extremely cost-effective, and practical—note that powdered milk formula can be used where fresh milk is not available.
Salt fluoridation
Several countries add fluoride to their salt. For example, in Switzerland 85% of domestic salt is fluoridated, in Germany 67% of domestic salt is fluoridated, and in Jamaica close to 100% (Marthaler, 2013). These salt fluoridation programs have generally been ‘tacked on’ to existing salt iodization programs, where small amounts of sodium iodide/ potassium iodide are added to the salt—improving thyroid function (Leung et al., 2012).
Salt fluoridation programs have been highly effective where they have been introduced. Results have indicated caries prevalence reductions in 12 year-olds ranging from 84% in Jamaica, 73% in Costa Rica, to 40% in Uruguay at an average cost of $0.06/ capita/ year (Gillespie & Baez, 2005). Even if these are significant overestimates, it is likely that such a program would be cost-effective. For example, imagine that the reduction in caries (in a hypothetical country which goes through this intervention) was 10X less effective than in Uruguay (so caries reduction decreases by 4% at a cost of $0.06/ capita/ year). Plugging these values into my CEA (the salt fluoridation page, so the cost of salt is changed to $0.06 per year) indicates that this would come out to approximately $167 per WELLBY in the first year, and $21 per WELLBY in subsequent years. This is extremely cost effective, as we currently estimate Give Directly improves welfare for approximately $199/ WELLBY.
A large proportion of salt in Africa is iodized, yet I could not find any records of salt fluoridation in any African countries. UNICEF estimates that approximately 81.5% of households in Eastern and Southern Africa consume iodized salt, and 83.3% of households in Western and Central Africa (Iodine, n.d.). Note that organisations such as GAIN are working to further increase this proportion; (Bilberrry, n.d.)
Overall, I think that salt fluoridation could be a highly effective intervention. There are current charities conducting salt iodisation projects in regions with poor dental access (e.g. GAIN) suggesting this approach would be possible. However, GAIN have indicated that they are not especially interested in fluoridation, as they are focused upon other micronutrients that the WHO rates as being more significant in terms of potential public health impact. The Borrow Foundation has funded some similar schemes (including a milk fluoridation scheme in Chile), and may be a useful source to identify suitable programs.
Education
According to the Global Oral Health Inequalities Research Network, gaps in knowledge constitute one of the key barriers towards reducing oral healthcare inequality (Abid et al., 2015). The WHO recommends educational programs in school, for example to make students aware of the link between sugary drink intake and poor oral health (Petersen, 2004).
I found it difficult to find data about oral healthcare knowledge from the areas that I have identified as being most neglected. However, data from Chad shows that 40.82% of the rural population report ‘never’ brushing their teeth, and 15.83% of the urban population (Natto et al., 2014). A study from Burkhina Faso (which is admittedly quite old—from 2006) also indicates that substantial proportions of both children and adults do not perform regular oral hygiene. In rural areas, approximately one tenth of 12-year-olds had tooth cleaning on a daily basis, and the majority of respondents were not aware of the benefits of fluorides for prevention of dental caries (Varenne et al., 2006).
Despite these gaps in knowledge, evidence about the effectiveness of existing oral health program interventions are somewhat mixed. For example, a systematic review of school-based dental health education found that they improved children’s dental healthcare practices (Geetha Priya et al., 2019), while a meta-analysis found that education alone is not sufficient to improve children’s oral hygiene skills (Stein et al., 2018). In reality, I suspect that this strongly varies according to the specific educational program in hand—this is something I would want to look into for a given charity (although note that education might form a complement to an intervention, rather than being a stand-alone program, e.g. training local dentists who also provide education).
Training local dentists
It is clear that there is a shortage of dentists in many LMIC (see Fig 10.) Increasing the number of dentists will allow people to attain necessary dental care, such as having a tooth pulled. In addition, local dentists could likely provide education to the surrounding community. Note that the charities listed below have not yet been vetted to Founders Pledge standards; I list them as examples, and as possibilities that may be worth examining in greater detail. There may be further promising charities in this general area.
One potential charity I found in this area is Bridge2Aid. They are a small, UK-based training charity who work in Africa—where they train local people in oral health promotion, as well as training local health workers to give emergency dental treatment. They estimate that one trained healthcare worker can give access to emergency dental care to 10,000.
Another possibility that I found is the Maldent Project. This is a collaboration between the Kamuzu University of Health Sciences and the University of Glasgow; the purpose is to establish a Bachelor of Dental Surgery degree program at the Kamuzu University of Health Sciences in Malawi. I suspect that up front costs would be very high, but this could have long-lasting effects.
Relatedly, the Afghanistan Dental Relief project trains local dentists as well as providing free care to local people.
Sugar tax
Sales of sugary foods (especially sugary drinks) are rapidly rising in sub-Saharan Africa (Reardon et al., 2021). A key method for addressing the impact of sugar is to introduce relevant legislation, such as the ‘sugar sweetened beverage tax’ introduced by the South African government in 2016 (Abdool Karim et al., 2020). Evidence has shown these taxes to be effective at reducing the purchase of sugary drinks; the equivalent of a 10% sugar sweetened beverage tax is associated with a 10% decline in purchases (95% CI: 5% to 14.7% decline) (Teng et al., 2019). There is some evidence that reductions in sugar sweetened beverage consumption tends to be greatest in the poorest households (Reducción en el consumo de bebidas con impuesto después de la implementación del impuesto en México, n.d.).
These taxes are thought to be cost-effective, and to have significant health benefits through driving a reduction in consumption. In Mexico, an excise tax of 1 peso per litre on sugar-sweetened beverages was implemented in 2014. It is estimated that this tax saved $3.98 per dollar spent on its implementation, due to a reduction in healthcare costs (Basto-Abreu et al., 2019). In addition, it is thought to have prevented 239,900 cases of obesity and 61,340 cases of diabetes (Basto-Abreu et al., 2019).

Seven African countries already have sugar taxes, such as South Africa and Morocco (Popkin & Ng, 2021). Note that the introduction of sugar taxes in South Africa generated significant controversy, due to perceived impacts upon local cane growers. However, it is generally considered to have been successful overall; see the WHO coverage (South Africa’s Sugar Tax, n.d.).
I couldn’t find many groups working on this, but I did find an NGO lobbying for this in Kenya.
Conclusion
Oral health in LMIC is an important and neglected area for global wellbeing. Poor oral health is extremely common, and—in the absence of treatment—can cause severe pain and consequently impact wellbeing. In turn, the lack of oral healthcare in LMIC is startling and is likely to become an even more significant problem as LMIC undergo the nutrition transition towards a more westernized diet. The neglect of oral health has occurred for several reasons, including the focus of existing health initiatives upon reducing mortality as opposed to suffering, and a historical focus upon curative dental treatment rather than (cheaper) preventative treatment. However, oral health is likely also a tractable issue: LMIC (and charities working in LMIC) can learn from the mistakes of the HIC approach, by better investing in preventative (rather than purely curative) treatments. Interventions such as fluoridation and sugar taxes are likely to be highly cost-effective, and some curative treatments (such as training local dentists) may also prove to be cost-effective. Finally, this report highlights the importance of understanding the relationship between pain and wellbeing (also see; Sharma et al., 2020)—an area that may be crucial towards establishing funding opportunities that are high impact with regards to improving global wellbeing.
Open questions
I am currently searching for suitable organisations working in this area, and would be grateful for any leads or recommendations. In particular, I have not been able to find many groups working in milk/ salt fluoridation in LMIC: I would welcome any information about this (such as potential leads, groups who might be interested in this, ideas of how to best implement this, or information about why this intervention might be less practical than this research has thus far suggested). I also especially welcome any information about groups lobbying for sugar taxes in LMIC.
Acknowledgments
I would like to thank Matt Lerner for insightful comments and advice on earlier drafts, and Prof. Stefan Ruhl for generously sharing his expertise with me. I would further like to thank all the researchers at Founders Pledge for their helpful comments during an initial presentation on this topic, and to everyone at Founders Pledge who bounced ideas around with me.
About Founders Pledge
Founders Pledge is a community of over 1,700 tech entrepreneurs finding and funding solutions to the world’s most pressing problems. Through cutting-edge research, world-class advice, and end-to-end giving infrastructure, we empower members to maximize their philanthropic impact by pledging a meaningful portion of their proceeds to charitable causes. Since 2015, our members have pledged over $7 billion and donated more than $700 million globally. As a nonprofit, we are grateful to be community-supported. Together, we are committed to doing immense good. founderspledge.com

Bibliography
Dental abscess. (2017, October 18). Nhs.Uk. https://www.nhs.uk/conditions/dental-abscess/
GHO. (n.d.). Retrieved 24 May 2022, from https://www.who.int/data/gho
Marthaler, T. M. (2013). Salt fluoridation and oral health. Acta Medica Academica, 42(2), 140.
Oral Health Conditions. (2020, November 3). https://www.cdc.gov/oralhealth/conditions/index.html
WHO. (2020). WHO methods and data sources for global burden of disease estimates 2000-2019.
WHO. (2022, March 15). Oral health. https://www.who.int/news-room/fact-sheets/detail/oral-health
Appendix
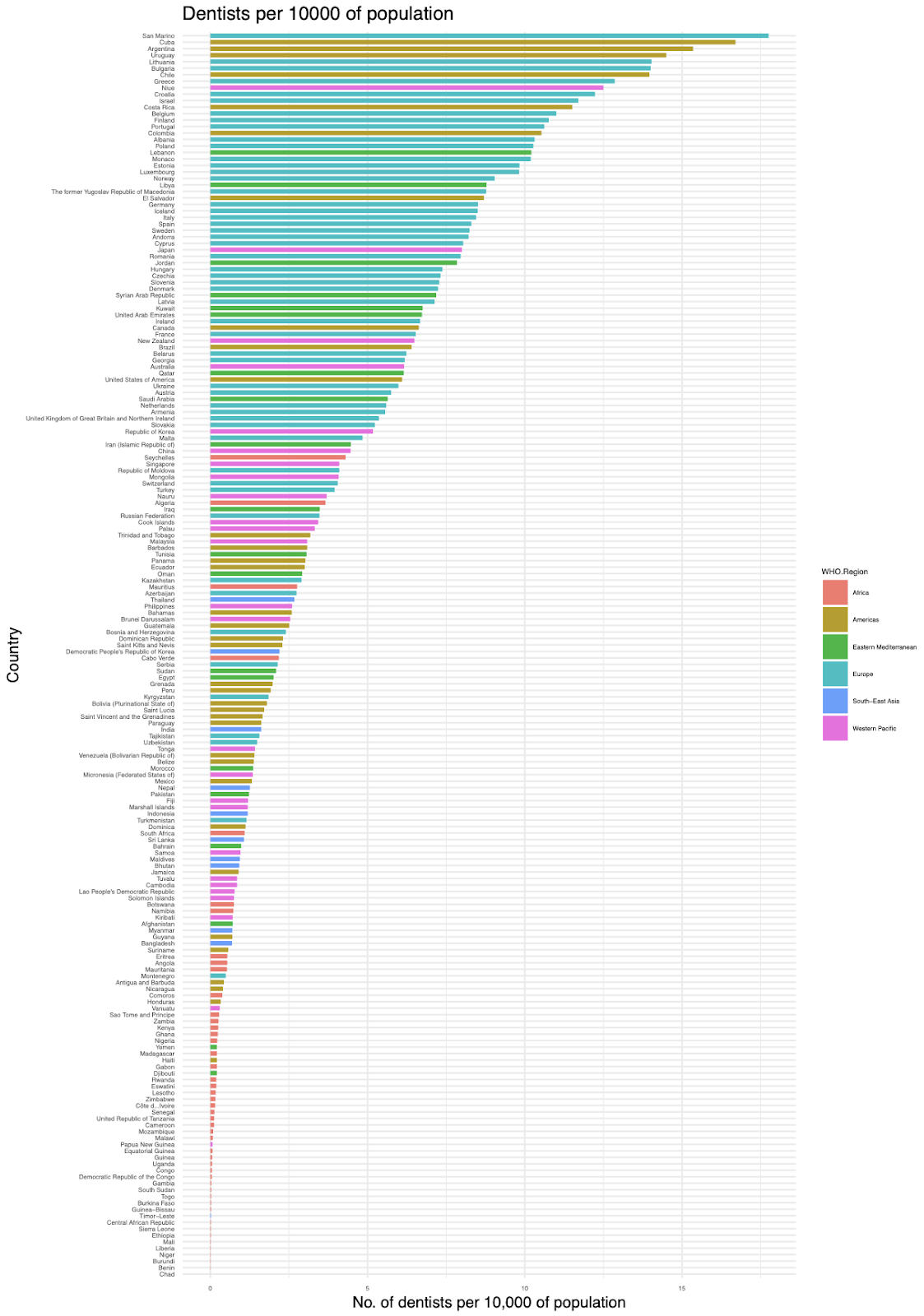
Fig 15: Dentists per 10,000 of the population, y country. Data from (GBD Results Tool | GHDx 2019), mapped with ggplot2 (Wickham, 2011).
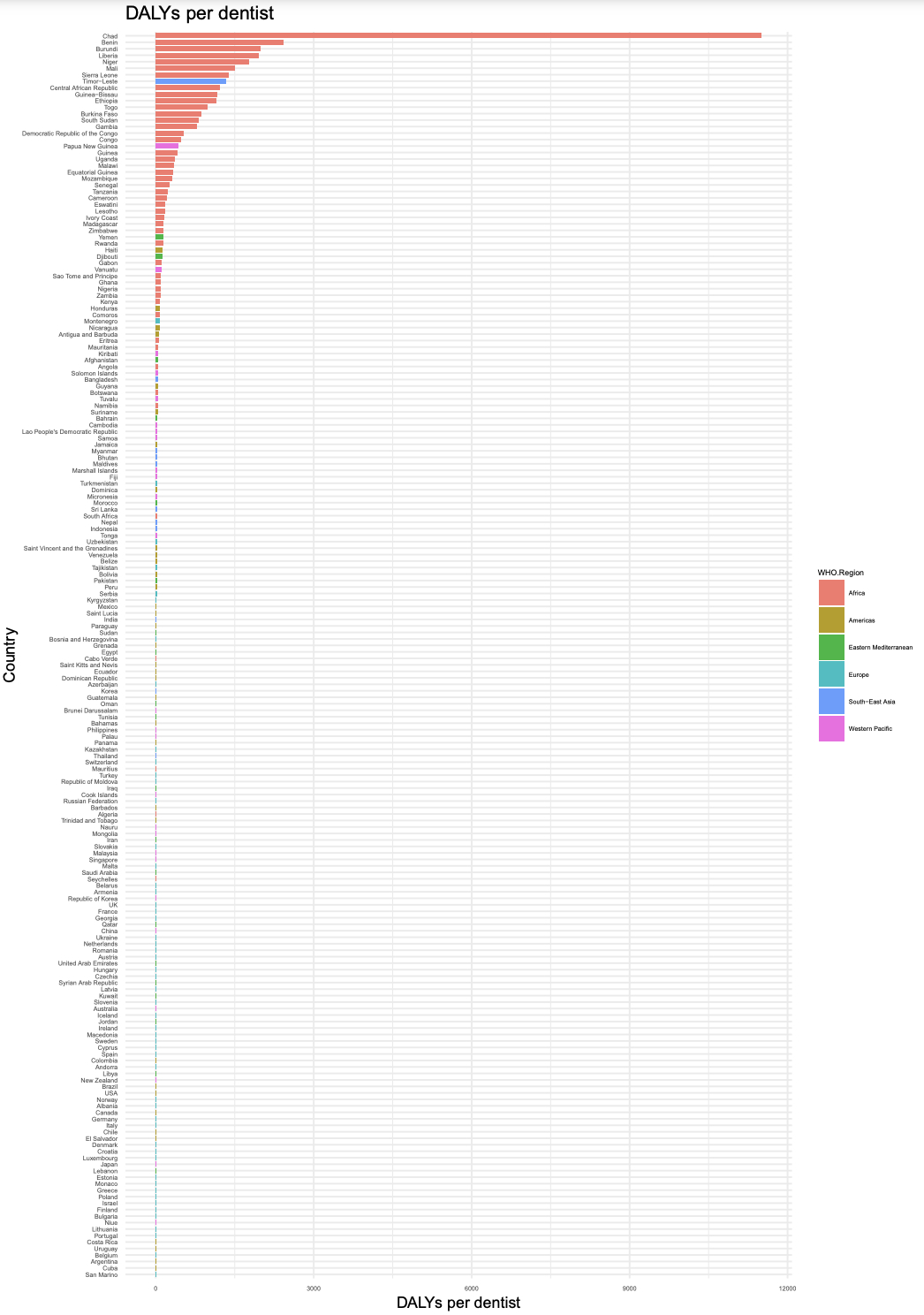
Fig 17: DALYs per dentist, by country. Data from (GBD Results Tool | GHDx 2019), mapped with ggplot2 (Wickham, 2011).
- ^
Note that it is unclear if this relationship is causal or merely correlative; this is covered within the 'Impacts from associated disease risk' section
- ^
Note that DALY scores may underestimate the suffering imposed from poor oral health, as I argue in the section ‘Is the burden of dental pain underestimated?’ However, given that other metrics (such as WELLBYs) have not yet been utilised to provide estimates for global oral health, I use DALY scores to give an overview of the impacts of poor oral health.
- ^
Note that the burden of edentulism is reported to be a lot higher in higher-income countries, presumably reflecting the older population of these countries.
- ^
It is difficult to estimate this value given that dental pain prevalence is very geographically variable. I weight the meta-analysis from children quite highly, given that it pulls from a large body of data (estimate of a 50.1% lifetime prevalence in children in Africa; Pentapati et al. 2021) but note that this is the lifetime prevalence. The study in Iran used a cross-sectional approach and achieved a high response rate (97.3%, Kakoei et al. 2013), so I also weight this quite highly.
- ^
One week after treatment, their average score reduced to 9.125.
- ^
I attempted to ascertain the degree to which people (in $) value treatment of dental pain, but I could not find enough data.
- ^
C-reactive protein (CRP) is a protein made by the liver, that moves to the bloodstream in response to inflammation. Hence, CRP is a marker of inflammation–and is strongly predictive of CVD.
- ^
Note that the prevalence figure varies widely, e.g. another estimate is 30,000-40,000 (Srour et al., 2017)
- ^
It is possible that statistical measures were taken to proportionately weight the responses of people from different countries/ economic groups according to their global representation; I struggled to find much information about this, and could not find evidence for this in the documents I read from the WHO about their methods (e.g. WHO, 2020). I would welcome any further information about this.
- ^
As argued in the section above, I do not think that DALYs are a perfect measure by which to capture the suffering caused by dental diseases. However, as far as I am aware, they are the only available measure that can provide a global overview of the impacts of oral disorders.
Thanks for this great analysis. This definitely speaks to some limitations of the most widely-used global health and well-being metrics. It seems to me that sugar taxes could be particularly promising due to multiple public health benefits (not only improvements in dental health). This seems like a worthy contender for the Cause Exploration Prizes; you might consider submitting it if you haven't already!
Thank you Marshall! Definitely agree with you about the limitations of DALYs—as useful as they can be in some contexts—and the point that sugar taxes likely have benefits beyond oral health. I think sugar taxes (and maybe other regulation, like trans fat regulation) are likely to be impactful in part from having pretty broad-reaching benefits that aren't reflected in my CEA here (blood pressure/ cardiovascular health, obesity, oral health, etc etc).
Thanks also for the note about the cause exploration prizes! Unfortunately, I think this piece is too long (and now has already been published online)—so I don't think it's eligible (? not quite sure) but i'll check it out!
Hi Rosie, great post!
When I looked at this briefly a year ago I flagged two organizations that seemed promising:
https://www.globaldentalrelief.org/
https://www.gcdfund.org/
Both are more holistic than the specific interventions you looked at. Did you happen to look at either of these in your research?
Thanks!
Thanks Tyner! I was hoping someone might be aware of potential orgs :) I haven't checked those ones out yet– I will add them onto my list to check out.
I expect that the main reason that your post doesn't recommend flossing is due to the lack of good evidence-based studies that show the benefits of flossing.
Funding more research into dental health to see whether intervention such as flossing should be rolled out more broadly, might be a good use of money.
Other cheap interventions such as tongue scrapping likely also deserve to be studied to check whether they are beneficial for oral health.
Yep! I do think flossing is good, but I suspect it's less impactful/ helpful than fluoride (especially fluoride added to water/ milk/ salt).
Thanks! I didn't especially look into tongue scraping, but I'll check it out a bit more. My general sense would be that it would be tricky to persuade people to do regularly, in comparison to something 'automatic' like fluoridated salt.
Instead of spending money on training local dentists, it might be more worthwhile to do disruptive innovation. There's no reason to believe that the eyes of dentists are superior at diagnosis to a well-trained machine learning model.
Dental health care as currently practiced needs a lot of trust. I have to trust my local dentist with their assessment of whether my teeth need costly procedures. Having well-justified trust is easier in the first-world even when first world dentists still differ a lot in their treatment recommendations. In the third world it's more likely that dentists will abuse trust by selling their customers unnecessary treatments.
If the diagnosis and treatment recommendations would be made by a branded computer program, it would get a lot easier to trust the model. Training costs would also go down if dentists wouldn't need to be trained in diagnosis anymore.
Interventions could also plausibly be automated but that might be more expensive than just automating the diagnosis.
Hey Christian, thanks for your comment! I totally agree that ML has great potential for diagnosis (in dentistry but also within the field of medical care more broadly– e.g. I was reading about this grant from Gates the other day, it's a diagnostic ultrasound for maternal conditions). Caveat that I'm not sure that the average person would trust an ML diagnosis over a 'real person' diagnosis (at least, not yet), and I think it would be a while until roll-out in an LMIC type context. Nonetheless, I think this is a promising area which I want to check out in more detail.
Within the field of oral health though, I think that investing in preventative treatment is currently more promising than diagnostics/ curative treatment: i.e. while I think that training up local dentists may be cost-effective, it seems a little borderline. However, preventative treatment (aka fluoride) seems to be extremely cost-effective, and we already know how to do it. This is mainly because salt and milk fluoridation appear to work and are insanely cheap—that's where my $2 WELLBY/ $9 DALY figures are coming from.
Part of why it's cheap is because you seem to put the non-monetary costs at zero.
Studies like https://ehp.niehs.nih.gov/doi/10.1289/ehp655 do suggest that there's a risk of negative side effects from just putting fluoride into everything.
Teeth need fluoride but it's likely harmful to the rest of the body. Application via toothpaste a lot more of the fluoride actually goes to the teeth has advantages over adding it to salt.
It might be that salt and milk fluoridation is still net-beneficial but that calculation is more complicated than just comparing the monetary cost.
As far as trust is concerned plenty of people also don't trust water, salt or milk fluoridization and programs by Westerns in Africa might face political problems.
Hi Christian,
Thanks for this comment, I am happy someone drew attention to this!
I did check out various papers (such as the one you linked, and some other papers proposing a link between fluoride exposure and adhd). I didn't find them convincing enough to add in a non-monetary cost to fluoride (bear in mind that I also left out various potential net-benefits, such as increased attendance at school and work).
To give a bit more detail (because I think this important), I found that the evidence linking fluoride to neurological outcomes was pretty low quality. I could only mainly find ecological studies, where i judge the risk of confounds to be very high- plus other issues that make me suspicious such as exclusion of outliers (without clear justification). That being said, I do think it's important to be cognisant of these theories, even if the available evidence is poor— I quite like this review, which basically argues that low to adequate levels of fluoride don't appear to be associated with any neurological conditions, but there is 'low level' evidence that they are at high concentrations.
To me, this gets at the point that fluoride should only be used in communities that have low levels of fluoride already— apart the speculation about neurological disorders, we know that fluoride can cause fluorosis (weakening of tooth enamel) in levels with high levels of fluoride. I have put the 'costs' of fluoride at zero, but have highlighted in the report that I think these kinds of interventions should only be used in area with low fluoride (for instance, not areas with high levels of groundwater fluoride). In areas with high fluoride, I agree with you that there might be 'costs' to be accounted for .
Totally agree with you on the point about trust! I quite like the salt/ milk interventions since they are more 'opt in' than water fluoridation (aka you could just buy the other salt/ milk), as well as being more practical in areas with lower levels of piped water access. I'd hope that this would mean less pushback.
The general way to account for side effects of clinical interventions is that low-level evidence is enough to take side effects seriously. Low-level evidence is enough for the FDA to require drug manufacturers to put a warning label on a drug.
The review you point to says "indicating the need for new epidemiological studies that could provide further evidences regarding this possible association". That means there's uncertainty about whether or not there's a negative effect.
If you actually take that systematic review seriously, the conclusion would be that philanthropists should fund more studies into investigating whether or not there's an association given that our current evidence base is not enough to know.
Hm I don't think that follows from the review- I would ideally like more studies looking at whether fluoride can affect IQ (esp at high concentrations), but I don't think this should be the highest priority thing.
I want to highlight that the 'low level evidence' refers to fluoride at high concentrations. As I've outlined above, I think that fluoride interventions should only be used in areas with low fluoride levels. See the start of that review's discussion, where it reads 'This systematic review and meta-analysis gathered evidence showing that, following the WHO classification of low and high levels in the drinking water, exposure to low/adequate water F levels is not associated with any neurological damage, while exposure to high levels is. The level of evidence for this association, however, was considered very low.'
I could still see an argument to add in a risk factor to my CEA, but (bearing in mind that this is in a low fluoride area) I think this risk is sufficiently small that it is not worth including. For example, I haven't included a factor for 'not in pain = can go to school = higher IQ/ earnings' which I'd argue has more support behind it. Nonetheless, I will keep an open mind and watch out for any new studies about this.