Update 2024-02-26: due to a
serious
typo all the results in this post were off by a factor of 100.
Sequencing from individuals still looks promising, but by less than it
did before. I've updated the numbers in the post, and added notes
above the charts to explain how they're wrong. Thanks to Simon Grimm
for catching my mistake.
While this is about an area I work in, I'm speaking for myself and
not my organization.
At the Nucleic Acid
Observatory we've been mostly looking at metagenomic sequencing of
wastewater as a way to identify a potential future 'stealth'
pandemic, but this isn't because wastewater is the ideal sample type:
sewage is actually really—the joke writes itself. Among other
things it's inconsistent, microbially diverse, and the nucleic acids
are have degraded a lot. Instead the key advantage of wastewater is
how practical it is to get wide coverage. Swabbing the noses and/or
throats of everyone in Greater Boston a few times a week would be
nuts, but sampling the
wastewater gets you 3M people in a
single sample. [1]
Imagine, though, that people were enthusiastic about taking samples
and giving them to you to sequence. How much better would that be?
What does "better" even mean? In Grimm
et al. (2023) we operationalized "better" as RAi(1%):
what fraction of shotgun metagenomic sequencing reads might come from
the pathogen of interest when 1% of people have been infected in the
last week. For example, in our re-analysis of Rothman et
al. (2021) we found a RAi(1%) of ~1e-7 for SARS-CoV-2,
which means we'd estimate that in a week where 1% of people contracted
Covid-19, one in 10M sequencing reads would come from the virus.
Let's say you were able to get throat swabs instead; what might
RAi(1%) look like?
The ideal way to determine this would be to swab a lot of people, run
untargeted sequencing, analyze the data, and link it to trustworthy
data on how many people were sick. But while public health
researchers do broad surveillance, collecting and testing swabs for
specific things, as far as I can tell no one has combined this with
metagenomic sequencing. [2] Instead, we can get a rough estimate from
looking at studies that just sequenced sick people.
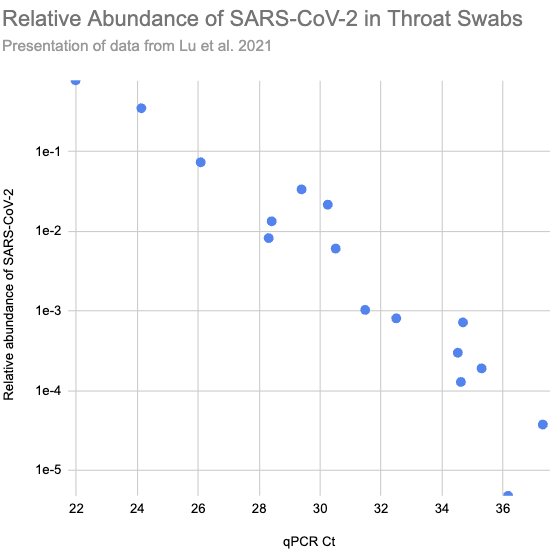
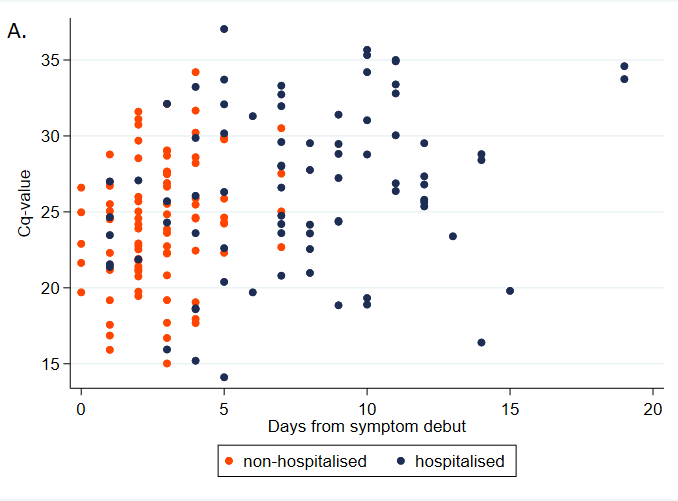
In Lu et
al. (2021) they ran shotgun metagenomic RNA sequencing on throat
swabs from sixteen Covid patients in Wuhan. Patients with higher
viral load, and so lower Ct values on their qPCR tests (roughly the
number of times you need to double the amount of SARS-CoV-2 in the
sample until it's detectable), consistently had higher relative
abundance:
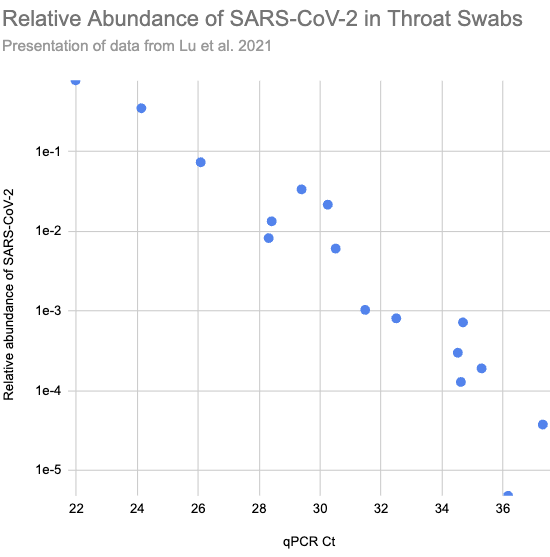
Larger version of Fig 2.a.1, reconstructed from Supplementary Table
S1)
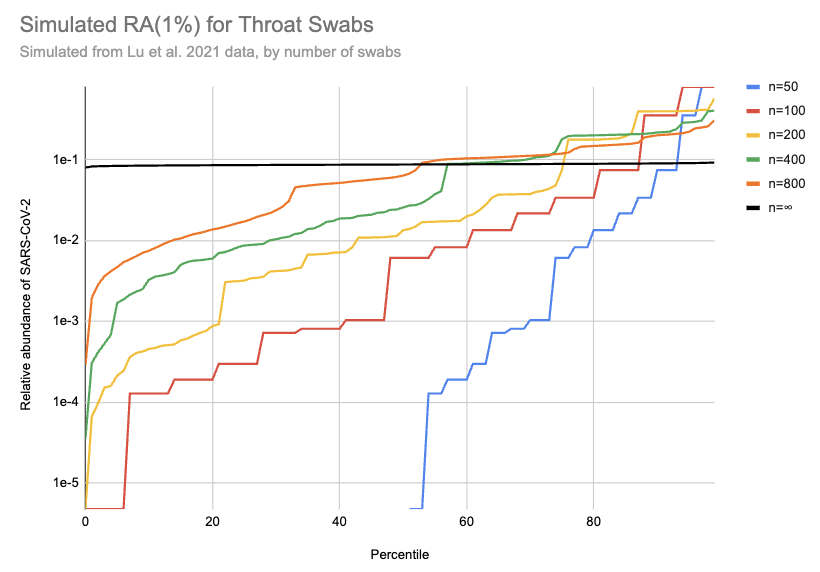
Imagine we got swabs from a lot of people, of which 1% were sick.
What sort of relative abundances might we get? If we collect only a
few swabs it depends a lot on whether we get anyone who's sick, and if
we do get a sick person then it matters a lot how high their viral
load is. On the other hand, if we collect a very large number of
swabs then we'll just get the average across the population. Assuming
for the moment that we can model "sick" as "similar to one of those
sixteen hospitalized patients", here's a bit of simulating (code):
[EDIT: the y-axis on this chart is 100x too high. For example, the
black line should be just below 1e-3]
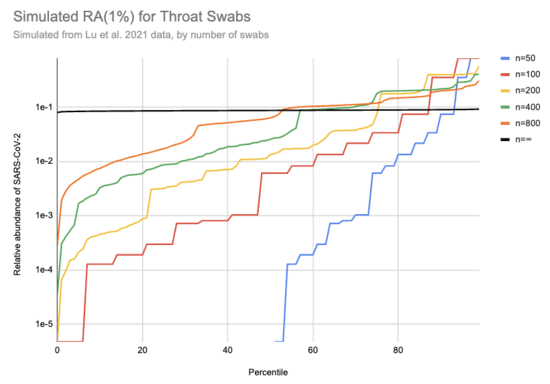
This is 10k simulations, ordered by the relative abundance each gave.
For example, if 1% of people are sick and you only swab 50 people then
in half the simulations no one in the sample is sick and the relative
abundance is 0, which is why the blue n=50 line only shows up for
percentiles 50% and above. On the other hand, if we collect a huge
number of swabs we end up with pretty consistently 0.08% of sequencing
reads coming from SARS-CoV-2. With 200 swabs the median
RAi(1%) value is 0.01%.
One major issue with this approach is that the data was collected from
hospitalized patients only. Having a high viral load seems like the
sort of thing that should make you more likely to be hospitalized, so
that should bias Ct values down. On the other hand, people tend to
have lower viral loads later in their infections, and hospitalization
takes a while, which would bias Ct values up. Here's a chart
illustrating this from Knudtzen
et al. (2021):
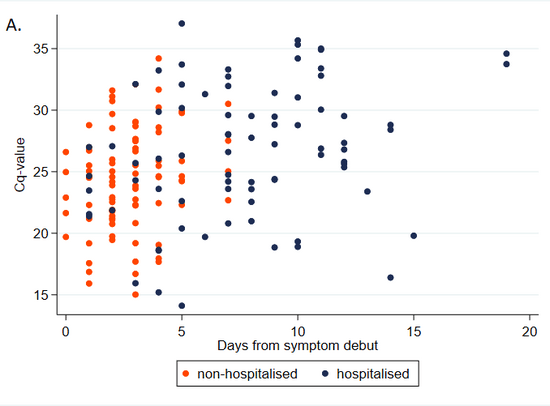
Note that Cq and Ct are different abbreviations for same
thing.
Is there a paper that tells us what sort of Ct values we should expect
if we sample a broad swath of infected people?
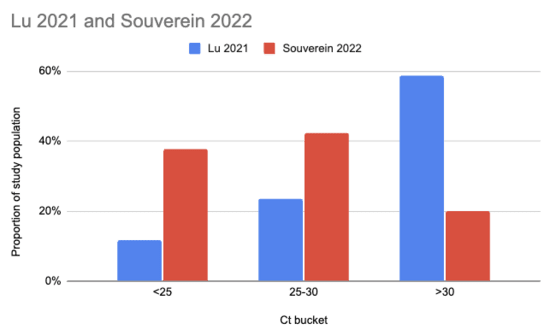
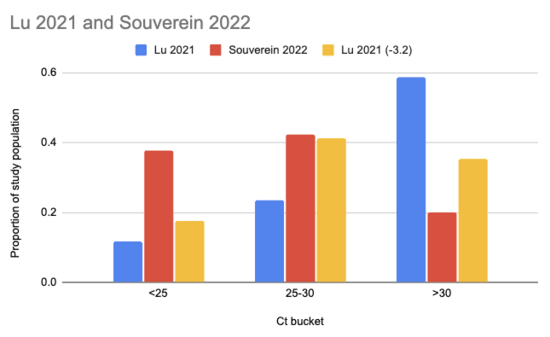
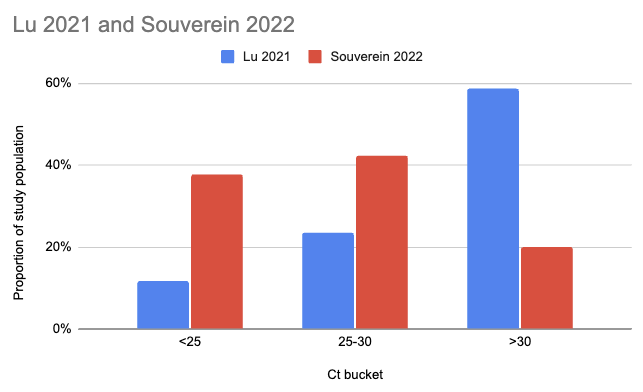
Souverein
et al. (2022) looked at a year's worth of SARS-CoV-2 PCR tests
from a public health facility in the Netherlands. The good news is
these tests averaged two days from symptom onset and they got results
from 20,207 people. The bad news is we only have data from people who
decided to get tested, which still excludes asymptomatics, and these
were combined nasopharyngeal (NP, "deep nose") and oropharyngeal (OP,
"throat") swabs instead of just throat swabs. Still, pretty good!
Comparing their Ct values to what we see in Lu et al. (2021), it looks
like viral loads are generally a lot higher:
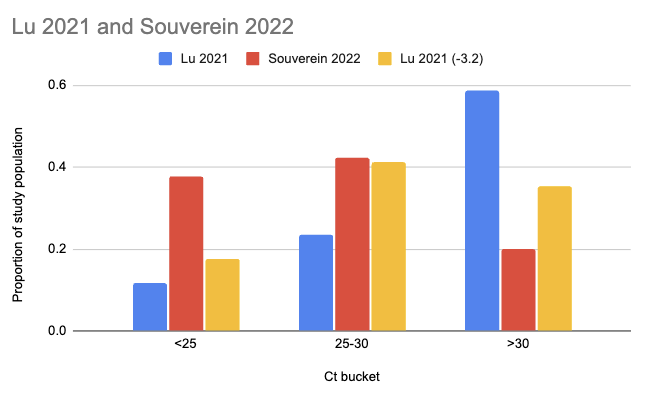
There are two issues with taking this chart literally. One is that
the combined swabs in Souverein should generally have given lower Ct
scores for the same viral load than throat-only swabs would have
given. A quick scan gives me Berenger
et al. (2020) where they found a median Ct 3.2 points lower for
nasopharyngeal than throat samples, so we could try to adjust for this
by assuming the Lu Ct values would have been 3.2 points lower:
The other issue, however, is worse: even though it's common to talk
about Ct scores as if they're an absolute measurement of viral load,
they're dependent on your testing setup. A sample that would read Ct
25 with the approach taken in one study might read Ct 30 with the
approach in another. Comparisons based on Ct within a study
don't have this problem, but ones across studies do.
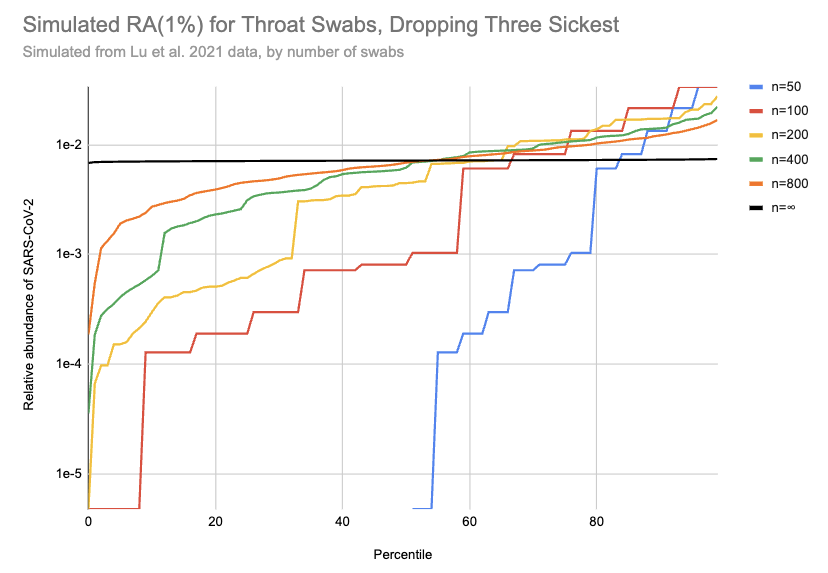
So, what can we do? My best guess currently is that the Lu data gives
maybe slightly lower relative abundances than you'd get sampling
random people, but it's hard to say. I'm going to be a bit
unprincipled here, and stick with the Lu data but drop the 20% of
samples with the highest viral loads (3 of 16) to get a conservative
estimate of how high a relative abundance we might see with throat
swabs. This cuts RAi(1%) by a factor of ten:
[EDIT: the y-axis on this chart is 100x too high. For example, the
black line should be just below 1e-4]
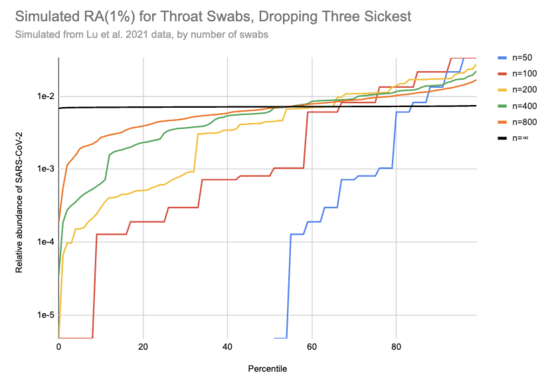
I really don't know if this is enough to where the remaining samples
are a good representation of what you'd see with random people in the
community, including asymptomatics, but let's go ahead with it. Then
with 200 swabs the median RAi(1%) value is now 4e-5, a
~400x higher relative abundance than we see with wastewater. [3] If
you could cost-effectively swab a large and diverse group of people,
this would allow surveillance with much lower sequencing costs than
wastewater. But that's a big "if": swabbing cost goes up in proportion
to the number of people, and it's hard to avoid drawing from a
correlated subgroup.
Thanks to Simon Grimm for conversations leading to this post and
for sending me Lu et al. (2021), to Will Bradshaw for feedback on the
draft and pointing me to Knudtzen et al. (2021) and Souverein et
al. (2022), and to Mike McLaren for feedback on the draft.
[1] Technically it gets you that in two samples, since Biobot tracks
the North System and South System separately. But you can combine them
if you want simpler logistics.
[2] If you know of someone who has, or who would if they had the money
for sequencing, please let me know!
[3] Pathogen
identification would also be much easier with swabs, since it's a
far simpler microbiome and the nucleic acids should be in much better
condition.
Comment via: facebook, facebook, lesswrong, the EA Forum, mastodon



Feel free to message me if you're interested in going deeper into what a typical viral load might look like. I can generate trajectories, based on the data from the ATACCC study. Note that this is in viral RNA copies, not Ct values - they did the conversion as part of that study.
Thanks! I'm most interested in viral load in the sense of the relative abundance you get with untargeted shotgun sequencing (since you need sequencing (or something similarly general) to detect novel threats and/or avoid having a trivially-bypassable detection system) but there's not much literature on this.