This is the third in a sequence of posts taken from my recent report: Why Did Environmentalism Become Partisan?
Summary
Rising partisanship did not make environmentalism more popular or politically effective. Instead, it saw flat or falling overall public opinion, fewer major legislative achievements, and fluctuating executive actions.
Public Opinion...
I think right now EAs might be making a significant mistake by paying insufficient attention to the political realm. As EAs we tend to figure out what’s most impactful for us to work on and focus hard. That’s great! But there are various actions that are ‘non-delegatable’ - the extent to which an individual can do the action is limited (like voting, going to a protest, making hard money contributions to particular campaigns). It might be useful if we were all more in the habit of doing variou...
New Video from AI in Context: The Fall and Rise of Sam Altman
If you want to skip straight to the video, here it is!
AI in Context is excited to be back with our fourth video! For those just hearing from us, we make videos for 80,000 Hours, telling stories about transformative AI...
If you're seeing this in summer 2022, we'll be posting many submissions in a short period. If you want to stop seeing them so often, apply a filter for the appropriate tag!
Summary (Conclusions)
Occupational causes of death and ill health have a significant, global impact. Worldwide, work-related factors are responsible each year for in-between 1.88 to 2.78 million deaths (ca. 5% of global deaths). Another estimate places global burden of disease due to occupational factors (combining deaths and disabilities together) at 2.7% of the entire global burden of disease. Global GDP lost is estimated at 4%.
South-East Asia, Western Pacific and Africa WHO regions are especially impacted in terms of workplace deaths and negative health outcomes, with Asia in general being the most impacted.
There are multiple global and local actors in the field of Occupational Health and Safety (OHS), however the general sentiment sourced from written expert comments is a one of neglectedness of the field, preventable harm not being prevented, global aid programs falling behind on their funding and results etc. Global spending on OHS is difficult to clearly estimate.
Broadly speaking, the issues of global OHS exhibit similarities to other general issues of global health and wellbeing. However, the topic received little attention from the Effective Altruism community so far.
Due to significant Importance and a worrying level of Neglectedness, better research on global OHS as an EA cause area is needed and can likely lead to tractable results.
Candidates for effective direct interventions can be recognized via further study of the most harmful occupational risk factors (e.g., exposure to long working hours, asbestos exposure etc.) and related negative health outcomes (e.g., work-related circulatory and pulmonary diseases).
OHS puts a large emphasis on prevention, and in developed countries there are multiple OHS interventions and standards with good track record. In principle, this makes it probable to use similar OHS methods in the developing world and achieve positive outcomes effectively – similar to how effective global aid interventions are achieved.
Sources of uncertainty
True scale of harm related to work-related causes is likely underreported and understudied; key statistics are several years old which prevents from assessment of the likely detrimental effects of COVID-19 on the global OHS.
Global landscape of OHS organizations, global aid programs etc. is a complex one – areas requiring expert knowledge were identified and indicated throughout the paper.
Detailed estimates on cost-effectiveness of existing OHS methods (especially when applied in the developing world) need to be further researched or produced where unavailable.
Importance
Definition:“Occupational safety and health (OSH), also commonly referred to as occupational health and safety (OHS), occupational health, or occupational safety, is a multidisciplinary field concerned with the safety, health, and welfare of people at work (i.e. in an occupation)” (Source).
Several reports were published in the recent years discussing the issue of OHS worldwide. These reports appear to be among the most comprehensive as well as the most popularly cited sources. Key findings of the selected reports are presented below:
WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury, 2000-2016: Global Monitoring Report (Published in 2021 - link)
WHO and ILO (International Labour Organization, the United Nations agency in the area of work – learn more here) analyzed 41 pairs consisting of occupational risk factor and associated health outcome. This was done across 183 countries covering all six WHO regions (Africa, Americas, South-East Asia, Europe, Eastern Mediterranean region and Western Pacific region).
Globally, for 2016 alone the authors estimated 1.88 million deaths and 89.72 million DALYs attributable to these 41 pairs.
Work-related diseases accounted for 80.7% of deaths and 70.5% of DALYs, while the remainder of deaths and DALYs were attributable to injuries.
The largest numbers of attributable deaths globally were due to exposure to long working hours (exceeding 55 hours per week); occupational particulate matter, gases and fumes; occupational injuries; and finally – due to occupational exposure to asbestos (in the descending order of attributable deaths). These four occupational risk-factors far outdistance any others. This is presented in Figure 1 from the report:
Majority of DALYs could be attributed to similar mix of causes (in descending order): occupational injuries; exposure to long working hours; occupational ergonomic factors; occupational particulate matter, gases and fumes; occupational noise and occupational exposure to asbestos. Per Figure 2 of the report:
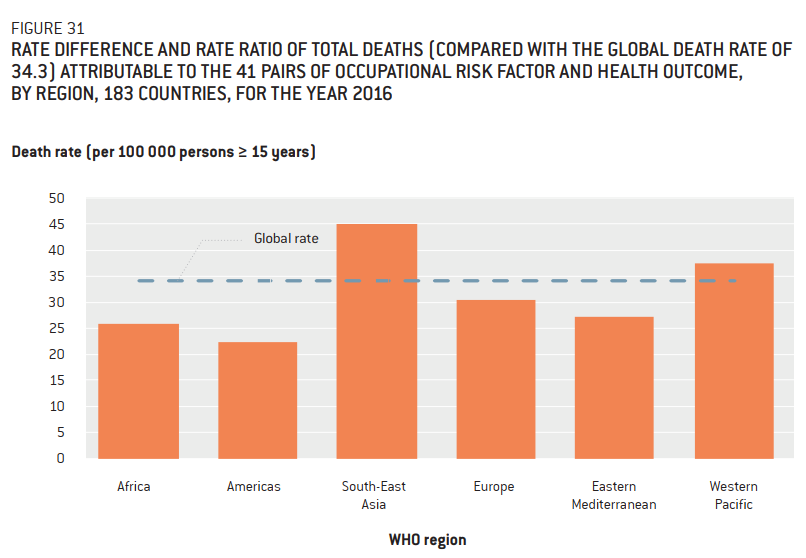
Work-related death rates per 100 000 were the highest for countries from South-East Asia and Western Pacific WHO regions. This is detailed in Figure 31 from the report:
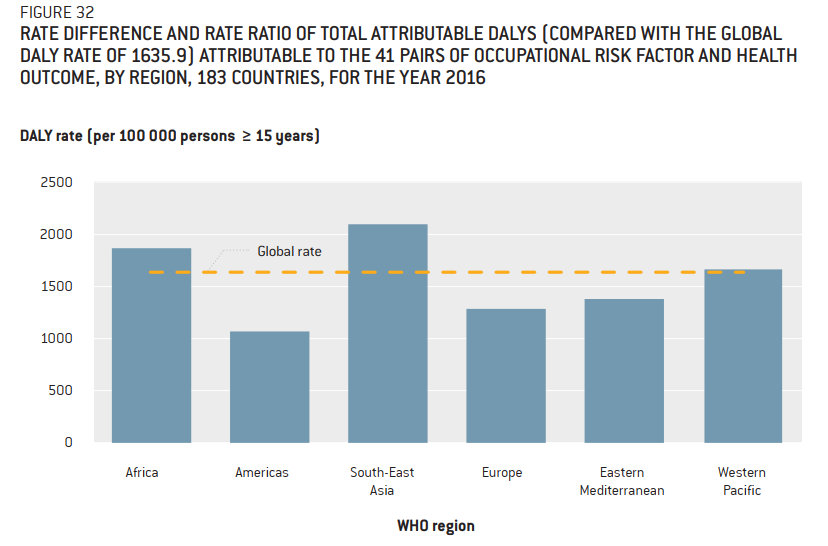
DALY rates per 100 000 were the highest in South-East Asia, Africa and Western Pacific WHO regions. This is detailed in Figure 32 from the report:
Comment: To set up a proper baseline for understanding the death rate and DALY rate it is worth noting that global death rate per 100 000 was 764 in 2016. (Source). World DALY rate per 100 000 from all causes was 34 275 in 2016 (Source).
Men and older age cohorts were also among the most highly affected in terms of both deaths and DALYs.
Chronic obstructive pulmonary disease, stroke and ischemic heart disease (resulting from occupational risk factors mentioned to this point) were the three health outcomes responsible for the largest shares of work-related deaths. For DALYs it was stroke; neck and back pain; and lastly - chronic obstructive pulmonary disease.
Authors were unable to provide estimates at a subnational level and relating to different occupations, industrial sectors and migration status. There is substantial room for improvement in terms of quality of data collected and in terms of researching further pairs of occupational risk factor – health outcome. Notably, biological risk, psycho-social risk and ambient air pollution risk were unaccounted for.
Global Estimates of Occupational Accidents and Work-related Illnesses 2017 (Published in 2017 by Workplace Safety and Health Institute (WSH), Singapore – link)
2.78 million of deaths could be attributed to work-related causes in 2014/2015.[1] Deaths due to work-related diseases and due to work-related accidents were split 86.3% vs 13.7%. Additionally, authors estimated non-fatal occupational accidents at 374 million in 2014. Overall, the number of fatal occupational accidents and fatal work-related disease cases was on the rise as of 2015. These findings are detailed in Table 4 of the report:
Work-related deaths are responsible for roughly 5% of global deaths.
Conditions responsible for largest shares of occupational mortality were circulatory diseases (31%), malignant neoplasms (26%), respiratory diseases (17%), occupational injuries (14%) and communicable diseases (14%).
For 2015 and when dividing the world into UN regions, work-related mortality in Asia exceeded sixfold the mortality for each of the three other major regions: Africa, America and Europe. In absolute numbers Asia had 1.8 million work-related deaths, while each of the three mentioned regions – roughly 0.3 million deaths each. Deaths in Asia constitute two thirds of work-related deaths globally. Asia also had the greatest number of deaths attributable to occupational injuries at 0.27 million.
Safety and Health at the heart of the Future of Work: Building on 100 years of experience (International Labour Organization, published in 2019 – link)
The authors repeat the figure of 2.78 million of work-related deaths, however (likely erroneously – see footnote 1) they state that this is a 2017 figure (p. 3, Introduction).
Combining several sources authors state that work-related deaths are 5-7% of the global deaths.
On sources of uncertainties the authors state: “The systematic collection and analysis of reliable and comparable data have varied both geographically and over time, which means that comparing trends and data is challenging. In addition, even in countries with the longest and most well-established data collection systems, under-reporting, particularly of non-fatal occupational accidents and especially work-related diseases, is common”.
In a different measure of prevalence of work-related disease and death, the authors refer to an earlier WHO estimate: “In addition, the most recent estimates from the WHO show that when accounting for both deaths and disability, the fraction of the global disease burden in the general population due to occupation amounts to 2.7 per cent (WHO, 2018).”
On the biggest occupational risk factors, the authors can be quoted as saying: “Most recent figures suggest that ergonomic factors, injury risk factors, particulate matter, gases, fumes and noise make the largest contributions to the total global burden of occupational disease (Driscoll, 2018).”
Mapping Risk: A Review of Global Data Sources on Safety and Risk (Published in 2019 by Lloyd’s Register Foundation and GALLUP, cited statistics cover few years back from 2019 – link)
Authors repeat the 2.78 million deaths figure from the Workplace Safety and Health Institute 2017 report.
Annually[2] there were 340 million work-related accidents and 160 million people suffering from work-related illness (per another International Labour Organization estimate). Associated loss of GDP due to lost workdays was 4 per cent[3] (USD 3.2 trillion at the time).
Authors of the report highlight several sources contributing to uncertainties: developing countries failing to collect data and produce figures related to occupational health and safety, methodological differences between different entities which produce relevant figures, data being not up-to-date or poorly structured.
Discussion
Overall picture of Occupational Health and Safety (OHS) worldwide can be painted as follows by combining certain findings of the reports:
Two most prominent and up-to-date estimates for annual work-related deaths worldwide are 1.88 million and 2.78 million.
Work-related deaths worldwide account for roughly 4.5% of total global deaths (calculation based on joint WHO/ILO report and 2016 death rate) or perhaps even 5% (Workplace Safety and Health Institute estimate) or even 7% (ILO 2019 report figure).
Non-trivial share of DALYs or by other metric: hundreds of millions of accidents and illness cases are also attributable to work.
Another estimate places global burden of disease due to occupational factors (combining deaths and disabilities together) at 2.7% of the entire global burden of disease.
WHO/ILO joint report states that South-East Asia, Western Pacific and Africa WHO regions are especially impacted in terms of workplace deaths and negative health outcomes, which is broadly corroborated by other reports (while in Africa the number of work-related deaths is relatively lower, the share of DALYs is higher).
Work-related accidents and illnesses are also a major source of workdays lost leading to substantial financial losses (estimated 4% of global GDP).
Among major work-related risk factors are long hours, injuries, bad ergonomics, exposure to airborne pollutants, noise exposure and asbestos exposure – these mostly result in deaths and illnesses related to circulatory and respiratory systems as well as due to malignant neoplasms (in addition to non-fatal conditions, such as neck and back pain).
Many occupational risk factors and negative health outcomes are likely underreported and understudied. Lack of recent data prevents from seeing the most recent trends.[4]
Sources of uncertainty
Some sources of uncertainty on the importance of the problem are discussed in the respective reports. These are: methodological differences between different sources of data, hard-to-compare metrics and statistics, low availability and quality of relevant information (especially for developing countries) and finally - available information being out of date.[5] Existing information generally predates COVID-19 pandemic. Possible improvement in the field might be if WHO/ILO produced their joint estimates on a more regular basis, which they seem to agree on doing in the future.[6]
Most often cited figures (such as 2.78 million work-related deaths worldwide annually) seem to come from a limited pool of research, later disseminated across different reports and in other online publications. This indicates the need for more research to confirm and narrow down the existing estimates (sometimes very different for crucial numbers e.g., 1.88 vs 2.78 million of global annual work-related deaths).
Work-related deaths, diseases and injuries are not entirely separable from the ones not attributable to work. While authors of the reports resort to established methods, for grantmaking purposes it would likely be worthwhile to further scrutinize these methods, if possible, since even minor methodological changes can sometimes highly affect the importance estimates and the resulting cost-effectiveness estimates.
Neglectedness
Most important actors in the field of global occupational health and safety (OHS)
Goal 8, Target 8.8: “Protect labour rights and promote safe and secure working environments for all workers, including migrant workers, in particular women migrants, and those in precarious employment”.
(Indirectly) Multiple targets of Goal 3: “Ensure healthy lives and promote well-being for all at all ages”.
ILO (International Labour Organization, the United Nations agency in the area of work – learn more here).
WHO – OHS is classified as a part of responsibility of the Environment, Climate change and Health team (Source).
Multiple national OHS agencies and national authorities: these can be surveyed e.g., via ILO Database on Occupational Safety and Health Agencies, Institutions and Organizations (INTEROSH) however the list appears to be rather limited.[7] Additional agencies can be found by browsing ILO country profiles.
Other Regional and national agencies, which occasionally deal with the topic of OSH (eg. trade organizations, industry-specific organizations etc.).
NGOs and charities: international charity examples are hard to find for a non-expert - one example might be: Workplace Health Without Borders. In addition, there are plenty of local charities all over the world, but the landscape is again difficult to survey without expertise. It should be noted however, that occupational health might not be a very popular charitable cause judging by number of charities alone:
Developed country example: searching the charity register of Charity Commission for England and Wales. Queried for a keyword “occupational” the database lists only 128 registered (mostly very local) charities out of more than 169 000 in the database (Source). Basic and imperfect as this example is, it lends credence to an observation that charities explicitly working on occupational health are relatively few and far between – however it is sure that health charities working on other causes inadvertently “pick up the slack” in OHS area.
Another example: Searching a US-based Charity Navigator database for a keyword “occupational” yields 21 charities with “Give with confidence” recommendation (out of 37 rated charities) with further 261 unrated charities (Charity Navigator states on its website that they have rated more than 195 000 charities overall).
Academia: While OHS is an established academic field,survey of papers released on the topic of occupational health and safety indicates that research on occupational health in general is visibly lacking in the least-developed countries, with the greatest deal of research conducted by developed countries. (Source).
General sentiment
The reports provided in the “Importance” section (and their respective press releases) offer several indications of high neglectedness of the occupational health and safety (OHS) worldwide:
Commenting on the joint 2021 WHO/ILO report Dr. Maria Neira, Director of the Department of Environment, Climate Change and Health at WHO noted “These almost 2 million premature deaths are preventable.[8] Action needs to be taken based on the research available to target the evolving nature of work-related health threats,”. Commenting on the same report Dr Tedros Adhanom Ghebreyesus, WHO Director-General said “It’s shocking to see so many people literally being killed by their jobs, (…) Our report is a wake-up call to countries and businesses to improve and protect the health and safety of workers by honouring their commitments to provide universal coverage of occupational health and safety services.” (Source for both comments).
Authors of the 2019 ILO report state in the Introduction: “It is a global imperative that these challenges [persistent work-related safety and health risks] are addressed with effective prevention strategies. Achieving effective prevention, however, remains a major challenge in addressing global occupational safety and health (OSH).”
Press release for the 2019 Mapping Risk report provides an informative summary on the state of OHS in many parts of the world: “While many countries around the world have signed on to international safety conventions and have laws and regulations in place, a new report from Lloyd's Register Foundation and Gallup finds that implementation and enforcement are weak in many countries. In addition, monitoring and gathering data on work-related injuries are "occasional, at best" in most countries. And globally, safety and risk data in general are patchy -- if these data exist at all.” (Source).
Other selected points to consider:
In general, the UN Sustainable Development Goals (SDGs) are at great risk of failing as of 2022 – the latest report on the matter does not directly address Target 8.8. however, the general sentiment on SDGs is: “(…) cascading and interlinked crises are putting the 2030 Agenda for Sustainable Development in grave danger, along with humanity’s very own survival. (…) The confluence of crises, dominated by COVID-19, climate change, and conflicts, are creating spin-off impacts on food and nutrition, health, education, the environment, and peace and security, and affecting all the Sustainable Development Goals (SDGs). The Report details the reversal of years of progress in eradicating poverty and hunger, improving health and education, providing basic services, and much more.” (Source).
Another report from European Trade Union Institute entitled “Occupational safety and health in 2040 - Four scenarios” (2017) is focusing on the future possible trajectories of OSH, primarily in Europe. On the situation in global OSH, it states: “OSH itself faces many challenges, longterm problems and open issues despite the many positive developments of the last two centuries. One of its significant features is that workers still die, suffer injuries and contract work-related diseases although in theory there is sufficient knowledge, experience, written rules, standards and laws in Europe and throughout the world. The knowledge which can lead to much higher levels of worker protection is not sufficiently implemented in workplaces.”
It should be noted that situation of the workers worldwide is multi-dimensional and different facets of occupational health and safety are to a varying degree connected to general economic empowerment, rule of law, protection of labor rights, unionization, general workplace safety culture and recently – to changes in occupational landscape from COVID-19. There are alarming developments in all of these areas (An example discussion), which are likely to contribute to further neglectedness in work-related health and safety.
Worst-case scenario
One scathing expert opinion from 2018 entitled “Occupational health: a world of false promises” is particularly worth discussing separately being perhaps the harshest criticism of global OHS efforts of all other criticisms found during the desk research – even if the claims of the paper are exaggerated, they offer an informative exercise in viewing global OHS through the “worst-case scenario” lens. The most important points of the paper can be summarized with the following quotes:
On ineffectiveness of international OHS standards: “While international standards appear to obligate employers to provide occupational health and safety procedures, and to pay for occupational injury and disease, inadequate prevention, absence of worker protections, and a failure to provide compensation make a mockery of these standards.”
On large number of people having no legal OHS protection: “Occupational health and safety laws cover only about 10% of workers in developing countries.[9] These laws omit many major hazardous industries and occupations. Progress in bringing occupational health to the industrializing countries is painfully slow. In the poorest countries, there has been no progress at all.”
On international aid not acknowledging OHS: “Often ignored is the reality that a single occupational injury or illness can tip an entire family into poverty. The UN Universal Sustainable Development Goals (USDG) emphasise the need to prevent catastrophic illness from tipping families into poverty but has a blind spot in that it does not recognise occupational causes of such catastrophic illness and injury--if it did, it would emphasise prevention of workplace illness and injury. USDG calls upon developed countries to assist the development process in developing countries, particularly the least developed countries and to deliver on their long-standing pledges to commit 0.7% of their Gross National Income (GNI) to official development assistance programs, again without explicit mention of occupational health and safety.”
On the most vulnerable being the most likely to suffer additional burden from inadequate OHS: “The workers most vulnerable to workplace injury and disease are those with the least secure employment, low incomes, long hours, virtually no unionization, and inadequate diets, housing, transport, and access to broader health care or social security nets. Migrant workers, seasonal workers, indigenous workers, women,[10] and child workers are the most likely to be exposed to hazardous and toxic work, financial and sexual exploitation, environmental pollution, systems of workplace organization injurious to heath [sic], and social deprivation.”
On inadequate UN funding and response: “The United Nations (UN) budget is just large enough to create a public relations effort suggesting that the problem is being addressed, which it is not. This largely paper program provides an opportunity for most countries to simply agree to the principles, and to essentially ignore the problem.”
On ineffectiveness of academia: “Academic institutions use the developing world as a place for clinical and research training, again with little or no effect on worker protections and occupational health. Global Health is in danger of becoming a funding stream that generates ‘global health’ programs and institutes that may do research and training in poor countries, but whose essential purpose is to capture a share of the funder market for their institutions, staff and students.”
On effects of WHO programs: “The WHO produces a blizzard of paperwork that states virtually every possible goal of an international program of occupational safety and health, none with any measured effect.”
On effects of ILO Conventions and Recommendations: “The ILO adopts two kinds of standards: Conventions and Recommendations.[11] Only Conventions can be ratified and thus become legally binding on member states. (…) Ratification [of a Convention] by member countries is entirely voluntary. No sanctions are provided against member countries that do not ratify conventions, and there is usually no time limit set for ratification. Moreover, even if a country has ratified a convention, the ILO cannot enforce compliance. Ratifications are made by a disappointingly small percentage of ILO member states”.
General sentiment of the paper is additionally summarized in the abstract: “We find that United Nations agencies, WHO and the International Labor [sic] Organization (ILO), are faced with the global problem of inadequate worker protections and a growing crisis in occupational health. The WHO and ILO are given monumental tasks but only trivial budgets, and funding trends show UN agency dependence on private donations which are far larger than funds contributed by member states. The WHO and ILO have limited capacity to make the necessary changes occupational health and safety demand.”
Financing of international OHS aid programmes
To at least partially comment on the claims given in the “Worst-case scenario” section, it is valuable to give at minimum a cursory overview of funding of the major international institutions and programs committed to OHS:
ILO: Over the past ten years (2012 – 2022) total annual ILO budgets were usually in-between 0.2 and 0.3 billion USD, with some recent uptick (0.4 billion USD in 2021, 0.68 billion USD in 2022 so far) (Source).
UN Sustainable Development Goals (SDGs): it is difficult to assess how much funds were contributed to OHS under SDG framework since a) OHS is in varying proportions included in different SDGs and programs b) different programs often target more than one goal at a time c) The number of programs; number of funding sources; funding amounts and funding structure for different programs and SDGs - all are very extensive and require expert knowledge to investigate. It is likely though, that financial needs of OHS programs are not met, even if there are trillions USD going into SDGs yearly.[12]Recent report by Joint SDG Fund indicates great unmet financial needs of the SDGs: “Even before the COVID-19 pandemic, SDG financing was falling short of expectations, with an estimated annual gap of $2.5 trillion. The landscape further deteriorated with the pandemic, where the Organisation for Economic Co-operation and Development (OECD) estimated that the annual SDG financing gap in developing countries alone could increase by $1.7 trillion in 2020”.
WHO: “The current approved Biennium Programme Budget[13] for 2022-2023 is for US$ 6.72 billion” (Source). The exact funding for OHS is difficult to disaggregate for similar reasons to UN SDGs funding.
Based on these points, it is likely that global OHS spending under the largest international programs cannot be effectively tracked and identified beyond the mark of few billion USD globally per year. Perhaps the funding does not go much higher than that, however it is difficult to ascertain without expert disaggregation of UN Sustainable Development Goals. Judging by the above, it is likely that there still exists room for additional funding – however this too needs to be investigated in more detail. This estimate does not contain regional and national-level programs, as well as NGO spending which all should be added up to produce a total estimate of OHS spending worldwide.
Discussion
Despite major, international organizations, governmental bodies, charities (albeit relatively not very numerous) and academia acting in the field of global occupational health and safety, the general sentiment is that there is still a great need for improvement, especially in the developing world (by very own admission of several high-profile expert sources). Also, it is likely that the most harm is preventable using already available methods from the general body of OHS knowledge such as: safety laws, standards, education, safety protocols, supplies and equipment, health services, work organization practices, guidelines for OHS practitioners etc. These are not being utilized due to a combination of factors such as: inadequate OHS services and prevention; poor implementation or enforcement of laws; insufficient OHS research, data collection and expertise (especially in developing countries); lack of funds, general poor situation of many populations in the developing world, other issues being prioritized etc.
In the worst-case scenario there is a grave risk of existing interventions and organizations being largely ineffective – international standards and agreements being violated or unobserved[14]; interventions and protections not reaching the most vulnerable at all; OHS being not addressed under general international aid and other interventions; existing programs failing to deliver the expected results; general OHS landscape being underfunded or funding incentives being misaligned; actors in OHS sphere lacking adequate means of implementing and enforcing their recommendations etc.
As a back-of-the-envelope calculation, it is somewhat likely that the worldwide annual spending for global OHS under major global programs does not exceed few billion USD. However, the general sentiment still indicates that this can be improved given the magnitude of OHS challenges worldwide, especially in developing countries. Likely there are avenues to utilize more funding.
As discussed in the “Importance” section, there are many issues with assessing the true impact of global work-related deaths and ill health – by proxy, this is also an argument indicating neglectedness of the issue, especially since it is related to such a basic dimension of human life as work. It is likely that to some extent this is caused by how large and complex of an issue the global OHS is, however many actors in the OHS sphere themselves comment on the general challenges to understanding the big picture (as shown in several quotes thus far).
Also, the exact topic of OHS received little explicit attention from the EA community (little to no discussion of OHS in the EA Forum, little to no acknowledgement in popular EA books and introductory materials etc.) which is puzzling given general interest of EA community in the field of global health and development. Broadly speaking, the issues of global OHS exhibit similarities to general issues of global health and wellbeing (in causes, importance, neglectedness etc.). It is likely that some of the negative work-associated health effects are addressed via other discussions and interventions - for example related to lead exposure, South-Asian air quality, general poverty alleviation and global aid policy - without explicitly mention of the work-related context. Even if so, acknowledging the work-related perspective is still valuable for better understanding of the risk factors, harms – and possible effective interventions to reduce them.
Sources of uncertainty
Global landscape of prevention and treatment of work-related negative health outcomes is a complex one, with multitude of actors, so it is difficult to paint a complete and accurate picture of their roles, effectiveness, funding amounts and sources for a non-professional in the global OHS field. Further expert interviews (especially with experts on WHO and UN programs developing world OHS, as well as academic and NGO landscape) and research of paywalled journals are recommended to gain a better understanding of the neglectedness in global OHS.
Also, for a non-expert it is difficult to completely accurately gauge the general sentiment and urgency in the field – the examples provided in the “General sentiment” section make a case for neglectedness and for plenty of room for improvement. However, further research is needed to more objectively and measurably evaluate the claims made by experts, especially the ones outlined in the “Worst-case scenario” section, including claims on near complete non-effectiveness of international bodies and programs such as The UN Sustainable Development Goals. Additional research to either confirm or deny the allegations contained in the “worst-case scenario” paper would be very useful, since this trajectory appears to be much worse than other critical but less extreme views of the global OHS issues.
The neglectedness might be also hard to estimate because there are multiple and varied risk factors and adverse health effects resulting from work – it is possible that other discussions (in EA community or elsewhere) and other interventions already take stock of some of the work-related harms, however without explicitly relating them to work. This would have to be evaluated on a case-by-case basis by systematically researching how different causes of work-related death and ill health are already addressed by other interventions.
Tractability
General interventions aimed at improving the field of occupational health and safety (OHS)
Firstly, general possible interventions for improving OHS as a field must be discussed. As presented in the previous sections OHS worldwide is troubled by a lack of a complete picture of harms, together with a level of neglectedness and unfulfilled potential. To remedy this, the reports cited previously suggest e.g.:
Further, more granular research into the worldwide burden of work-related deaths and disease (e.g., WHO/ILO Joint 2021 report).
Work on anticipation of new OHS risks (Quote from a recommendation in 2019 ILO report, p. 56: “In recent years, foresight processes have emerged, particularly in Europe, which aim to identify and prioritize research and innovation to deal with the type of changes identified in this report. These include practices such as forecasting, technology assessments and future studies, which enable the identification of potential work-related safety and health risks and the development of effective preventative actions”).
Greater incorporation of OHS education into general education (ibid.)
Promotion of the importance of OHS for general public health (ibid.)
Advocacy for further creation and improvement of national and international labor standards (where lacking) and increase in their enforcement (ibid.)
Increasing OHS outreach to small and medium enterprises (Quote: “Engaging the private sector is key, especially to help reach out to micro, small and medium enterprises (SMEs). There has been substantial growth in the proportion of SMEs and their position overall in the economies in many countries. SMEs are estimated to generate over 50 per cent of new jobs globally and hire more workers than large enterprises in most developing and emerging countries. Many of these workers are employed in the informal economy. Therefore, SMEs have great potential to contribute to worker safety and health and wellbeing, as well as economic and social development. Nevertheless, employment in SMEs is too often in low-paid, low-skilled jobs that lack decent working conditions”). (ibid.)
General strengthening and improved funding of global institutions and programs (can be inferred from several reports).
Notably the OHS landscape is shifting across the globe with changes in digital and remote work, platform (gig) work, automation, nanotechnology, change in demographic patterns (related to age, gender, migration etc.), changing environmental circumstances (due to climate change etc.) and other variations. For a detailed overview of opportunities and challenges see 2019 ILO report.
One avenue of possibly effective intervention is further research for “future proofing” of global OHS via additional investigations on:
Importance (current assessment and future trends).
Neglectedness (current assessment and trends).
Sources of uncertainty (identified elsewhere in the paper).
Reasons for current failings of the global OHS.
Efficacy of remedies suggested by the global OHS experts (such as the ones outlined above and possibly others).
“Future proofing” is even more important given that negative impact of COVID-19 has likely increased the level of global OHS insecurity and introduced new challenges (as well as reintroduced some of the old ones).
Opportunities for effective interventions by new philanthropic actors (Discussion)
Large Importance of the problem of global OHS (greatest in the developing world) and worrying indications of Neglectedness support intuitions that there is a considerable potential for tractable direct interventions and related grantmaking. Apparent ineffectiveness of international and local actors might be on the other hand also taken as a proxy measure of how difficult it is to make tractable difference in worldwide OHS (if the efforts are already underway and they appear to have many problems, perhaps it is due to high difficulty/low tractability). However, this can be also said for other areas such as global poverty, in which there is evidence for a number of possible effective interventions after all. In general, the problem of OHS is intertwined with the problem of global poverty and other problems of the developing world – however, assuming a work-related optic might uncover effective interventions which were missed previously, when researched from other angles.
It is likely that niche effective interventions can be found going forward on a case-by-case basis - candidates for effective interventions can arise from evaluating:
Work-related risk factors such as occupational exposure to vapors, gases and fumes; exposure to long working hours; occupational asbestos exposure. Regarding the asbestos exposure example: An interesting model, success story and source for ideas is LEEP (Lead Exposure Elimination Project) supported by Givewell and Charity Entrepreneurship (also incubated by the latter).
Associated negative health effects e.g., neck and back pain, respiratory diseases and circulatory diseases. For an example overview of a cause area of low-back pain see this EA Forum post. As stated in the post “Open Philanthropy has awarded grants for pain research.”
Of special interest are risk factors directly and intrinsically related to work – such as ergonomic factors, which are not likely to be previously studied in the context of Effective Altruism and using its methods.
These intervention candidates can either take the form of completely new interventions or already existing interventions which are scalable and can absorb additional funding.
Organizations in the OHS sphere point out that it is the best – and usually possible too – to prevent occupational harm in the first place. Oftentimes preventive measures are more cost-effective, in some cases many times more so, than treating ill health and limiting other negative effects (e.g., economic, social etc.) after the damage is already done. Many of these OHS measures such as regulations, standards, education, safety protocols, safety supplies and equipment, health services, work organization practices, guidelines for OHS practitioners etc. already exist in the developed world and are successfully deployed (some remaining challenges notwithstanding). In principle, increasing the adoption of these measures in the developing world might allow to reap the benefits of using well-researched, already present and potentially highly scalable methods (akin to global health and wellbeing interventions).
Sources of uncertainty
OHS (both globally and in developed countries) is a very complex field with many areas to improve, therefore only a high-level overview of tractability is provided – additional research (including expert interviews, research of further academic papers, calculating specific effectiveness estimates etc.) is needed to narrow down the parts of the problem which should be addressed in the first place as well as to find more examples of possibly effective interventions. Only then it is feasible to investigate specific cost effectiveness estimates for the selected, most promising interventions.
Additional investigation of cost effectiveness of different interventions requires expert knowledge of Effective Altruism methods and OHS itself. Detailed estimates on cost-effectiveness of existing OHS methods (especially when applied in the developing world) need to be further research or produced where unavailable.
To further the knowledge on why existing efforts in OHS seem to have problems additional research and expertise on the topic of international aid, global poverty and failures in OHS in general is needed. This will lead to better understanding of tractability.
This overall result is cited in executive summary of the report and seems to have been produced by combining the best available estimates – 2014 estimate for fatal occupational accidents and 2015 estimate for fatal work-related diseases. Overall number of 2.78 million of work-related deaths is in no point in the report stated to be an annual estimate for 2017. Interestingly, the executive summary (likely erroneously) states that “We estimated 2.78 million deaths occurring annually across the countries being attributed to work, higher than the 2.33 million deaths estimated in 2014” – this suggests that 2.33 million estimate is for 2014 and that 2.78 million estimate is more recent. Contrary to that, page 11 of the report states (seemingly correctly): “There was an estimated 2.78 million fatalities compared to 2.33 million estimated in 2011.” [not 2014, as in previous quote]. In the end it is most likely that 2.78 million work-related deaths figure is for 2014/2015 while 2.33 million is for 2010/2011 as these are the numbers in the Table 4.
Another example: ILOSTAT, statistics department for ILO gives another set of figures and statistics on its website – these figures for some territories are as old as 2010 and for many indicators and countries they lag behind the annual update cycle.
From foreword of 2021 joint WHO/ILO report: “In 2016, we agreed to produce a single unified methodology and a single set of joint estimates on the work-related burden of disease and injury. In 2019, we further strengthened our partnership by signing a Collaboration Agreement to produce these estimates regularly.”
For example, in Poland the database lists two organizations while the government website lists seven, although it must be noted that the agencies listed on a government website often – in addition to OHS – deal with other facets of work (e.g. labor laws) or deal with OHS in a certain context (e.g. mining, nuclear energy etc.). This might be because of ILO purposefully including only the biggest actors in the database; however, the point still stands that a single, comprehensive list of national-level actors is hardly available.
Less extreme but still worrying estimate is given by WHO: “In many countries more than half of workers are employed in the informal sector with no social protection for seeking health care and lack of regulatory enforcement of occupational health and safety standards.” (Source for both quotes).
This is an interesting discrepancy with WHO/ILO joint 2021 report, which stated that it’s men who are disproportionally affected by poor OHS, however this is probably due to different methodologies and different dimensions of harm being discussed.
“To achieve the Sustainable Development Goals, annual investment requirements across all sectors have been estimated at around $5-7 trillion.” - Source.
"The Programme budget is a critical tool for Member States to set and approve the priorities of the Organization, define the targets to be delivered, and to monitor their achievement." (Source). Even if WHO mobilizes or directs other funding the Programme budget seems to indicate the general order of magnitude of funding that WHO commands.