Content information: This post discusses that lives can be valued negatively by intended beneficiaries.
TLDR: GiveWell can include the sign of life quality variable in its analyses.
Centre for Pesticide Suicide Prevention (CPSP)
In January 2021, GiveWell recommended an approximately $7 million general support grant for the Centre for Pesticide Suicide Prevention (CPSP). The Centre supports the deregistration of pesticides commonly used in suicide.
GiveWell assumes that the Centre accelerates the pesticide deregistration by 9 years in each of the countries of operation. The number of lives saved is calculated as the difference between the numbers of lives saved in different policy scenarios weighted by these scenarios' probabilities and the counterfactual improvement in pesticide suicide rates, as extrapolated from past trends. 25,938 lives are expected to be saved.
The assumption that the intended beneficiaries would otherwise suicide can suggest that they value their lives negatively.
GiveWell assumes that as a result of the pesticide deregistration [edit based on a comment: and agricultural productivity decrease, the expected value of the program falls by 30%. The productivity decrease can be much lower than 30%, around low units of percent.] The effects of this estimated productivity decrease on the quality of the intended beneficiaries’ lives are not discussed.
CPSP-promoted pesticide bans would affect entire nations with large farming populations, who live in extreme and national poverty. A 30% decrease in yield can result in increased hunger levels and decreased income levels, which can negatively affect the health and quality of life of millions of people.
If the decreases in health and life quality cause a large percentage of farmers to value their lives negatively, support of CPSP can cause millions of people to live dissatisfied.
Thus, while CPSP is expected to save thousands of lives, it can also cause [edit: millions an unknown number of people] to live dissatisfied.
Malaria vaccination in Kenya
(Edit based on a comment: The 2022 World Happiness Report (WHR) (p. 19) estimates 'happiness'[1] in Kenya as 4.5/10.) The Measuring people’s preferences IDinsight survey (edit: which shows values lower than similar reports) cites 2.3/10 (p. 42). If the neutral point, “the point where someone is neither satisfied nor dissatisfied,” is above (edit: 2.3/10–4.5/10), reducing mortality in Kenya by malaria vaccination can save lives of dissatisfaction.
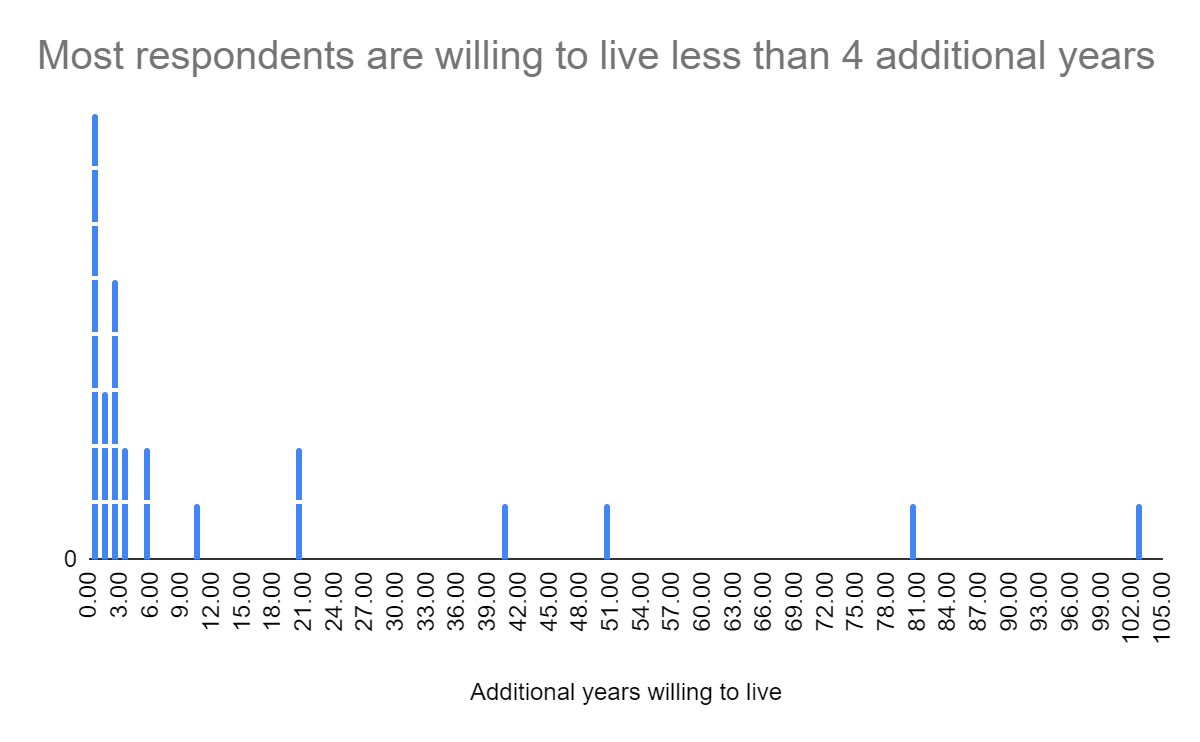
A small-scale (n=30) survey that I conducted in early 2021 in a Kenyan slum suggests that many respondents can value their lives negatively. Respondents were asked to label death and their quality of life on a visual analog scale (arrow) from the worst and the best imaginable situation. If worst corresponds to -1, death to 0, and best to 1, the average quality of life was -0.18, with a standard deviation of 0.40 (column AC). On average, respondents wanted to live 13 additional years (SD=26), while the median was 2 additional years.
The wording of the quality of life questions and their survey context can be assessed as leading, which can suggest low quality of data.
If you mai[n]tain your lifestyle and the future is what you expect it to be, how many more years starting from now do you want to live? You can say anything from 0 to forever.
Where do you place death on this arrow? Please put a line there and write "0." … Where do you place yourself on this arrow? Please put a line there and write "myself."
A local enumerator familiar with the area collected the data, while knowing that it is gathered for informational purposes only, without a possible benefit of answering in any specific way. While some (globally poor) respondents accepted a small stipend for their time (which is a custom in the area), many were happy to share their responses without a stipend. This can suggest that respondents answered relatively honestly, with little experimenter bias.
This survey shows that the quality of life in a Kenyan slum can be valued negatively by the respondents. The quality of life in areas of Kenya that are prioritized for malaria vaccination can be different in sign, for example due to urban-rural disparities. Further research on the expected sign of life quality of intended malaria vaccination beneficiaries (considering possible philanthropic and market co-interventions) can inform whether, when, and to whom GiveWell should recommend the scale up of this pilot.
Conclusion
GiveWell can consider incorporating a variable on the sign of the quality of life from the perspective of intended beneficiaries in their Centre for Pesticide Suicide Prevention and malaria vaccination analyses. The inclusion of this variable in GiveWell's analyses can inform whether programs that "save or improve" lives should be prioritized.
- ^
WHR "happiness" is a function of GDP per capita, social support, healthy life expectancy, freedom to make life choices, generosity, perceptions of corruption, and a constant (p. 19). Other possible aspects of happiness, such as family relationships and perceptions of fairness can be covered to a limited extent by this metric. I have not extensively reviewed the World Happiness Report methodology.
Thank you. This actually makes a lot of sense. The farming improvements (although could be different in different areas and studies) are astounding. For example, One Acre Fund increases farmers' annual income by about $100 or 50%, for the cost of about $25/farmer in 2021. Bednets have an equivalent nominal impact for about a fifth ($5) of the price.
Sidenote: the lower % improvement suggests that AMF serves relatively affluent farmers (with average annual incomes of $633 ($76/12%*100%), which can have twice to five times the real value) (unless the $76 is real value).
The agricultural productivity can increase because people are less sick and more productive. Also people could have a greater capacity to seek better farming practice information, livestock could be less ill (if bednets are used to cover livestock), and fishers could have better equipment.
Also, children could be able to help with chores rather than occupy parents or older siblings to care for them. Reduced treatment spending can be also substantial. Assuming that malaria treatment costs $4 and a bednet prevents 2 cases of malaria per year, then a family with 5 children (who would be treated if they get malaria) can save $40/year, which can a substantial proportion of their income.
In terms of attendance, bednets can have limited effects (about an additional week of school per year?).
That is about 10 days/year. If a bednet prevents half of the cases, that is 5 days or a week.
The impacts on enrollment can be relatively larger due to the increased farming income and reduced treatment cost if education expenses are substantial. For example, if education costs $100/year, then an additional child can be educated. If education expenses are close to zero, then malaria does not affect enrollment.
The quality of education or its relevance to employment is not directly addressed but can be addressed indirectly by enrolling a child in a better (higher paid) school.
Reducing mortality can have positive impact on savings and investments due to the reduction of funeral costs, which can constitute a large proportion of a family's annual income.
I am not familiar with the research on long-term health improvements. I imagine that early treatment of cases that would be more severe, especially for young children, is a key factor. Prevention reduces the rate when this would be needed.
--
Ah hah hah, yes, it is "net-positive life" but perhaps not life quality. Let me show you some of these videos:
People in a slum, possible abuse and neglect in spousal relationships, FGM, FGM and family, some parents decide that their child cannot live, and sending family members for life-long shrine work.
These are just arbitrary examples that show abuse, neglect, and addiction, mostly from countries that AMF does not operate in. It is possible that similar situations exist in some areas of countries of AMF operation.
The argument that in these situations, people can feel worse than if they were dead.
On a positive note, there are also very chilled environments where lovers get married as well as officials who support consideration based on reasoning.
Although currently you do not consider life quality factors, you could use these factors to put pressure on governments to advance legislation and governance that prevents dissatisfied lives, such as by banning FGM, forced marriage, or ritual servitude.
Even if additional measures are needed to improve life quality, considering these factors can be a statement that AMF, a large player, communicates. Implementing an somewhat sophisticated metric (such as a weighted average with some exponents) can engage officials in calculating what legislation and agreements would net them the most nets (haha), rather than using blame or other negative motivation to achieve the same result.
Preferring life satisfaction (or its proxies) statistics and expert estimates can have positive effects on governance/institutional decisionmaking of AMF partner countries and regions, such as the development of government networks of people familiar with the concepts (and interested in the improvements) of life quality measures and the government's interest in quantifiable impact.
Not to bother you anymore, but if a government decides to give its 1 million nets to its worst slum and leaves the people who seem to have all they need (except maybe bednets) uncovered, that's actually equally great as vice versa, and better if malaria rates in the slum are 10% higher than those in the countryside, because more children will be able to survive and people will have more for daily spending. Right.