Content information: This post discusses that lives can be valued negatively by intended beneficiaries.
TLDR: GiveWell can include the sign of life quality variable in its analyses.
Centre for Pesticide Suicide Prevention (CPSP)
In January 2021, GiveWell recommended an approximately $7 million general support grant for the Centre for Pesticide Suicide Prevention (CPSP). The Centre supports the deregistration of pesticides commonly used in suicide.
GiveWell assumes that the Centre accelerates the pesticide deregistration by 9 years in each of the countries of operation. The number of lives saved is calculated as the difference between the numbers of lives saved in different policy scenarios weighted by these scenarios' probabilities and the counterfactual improvement in pesticide suicide rates, as extrapolated from past trends. 25,938 lives are expected to be saved.
The assumption that the intended beneficiaries would otherwise suicide can suggest that they value their lives negatively.
GiveWell assumes that as a result of the pesticide deregistration [edit based on a comment: and agricultural productivity decrease, the expected value of the program falls by 30%. The productivity decrease can be much lower than 30%, around low units of percent.] The effects of this estimated productivity decrease on the quality of the intended beneficiaries’ lives are not discussed.
CPSP-promoted pesticide bans would affect entire nations with large farming populations, who live in extreme and national poverty. A 30% decrease in yield can result in increased hunger levels and decreased income levels, which can negatively affect the health and quality of life of millions of people.
If the decreases in health and life quality cause a large percentage of farmers to value their lives negatively, support of CPSP can cause millions of people to live dissatisfied.
Thus, while CPSP is expected to save thousands of lives, it can also cause [edit: millions an unknown number of people] to live dissatisfied.
Malaria vaccination in Kenya
(Edit based on a comment: The 2022 World Happiness Report (WHR) (p. 19) estimates 'happiness'[1] in Kenya as 4.5/10.) The Measuring people’s preferences IDinsight survey (edit: which shows values lower than similar reports) cites 2.3/10 (p. 42). If the neutral point, “the point where someone is neither satisfied nor dissatisfied,” is above (edit: 2.3/10–4.5/10), reducing mortality in Kenya by malaria vaccination can save lives of dissatisfaction.
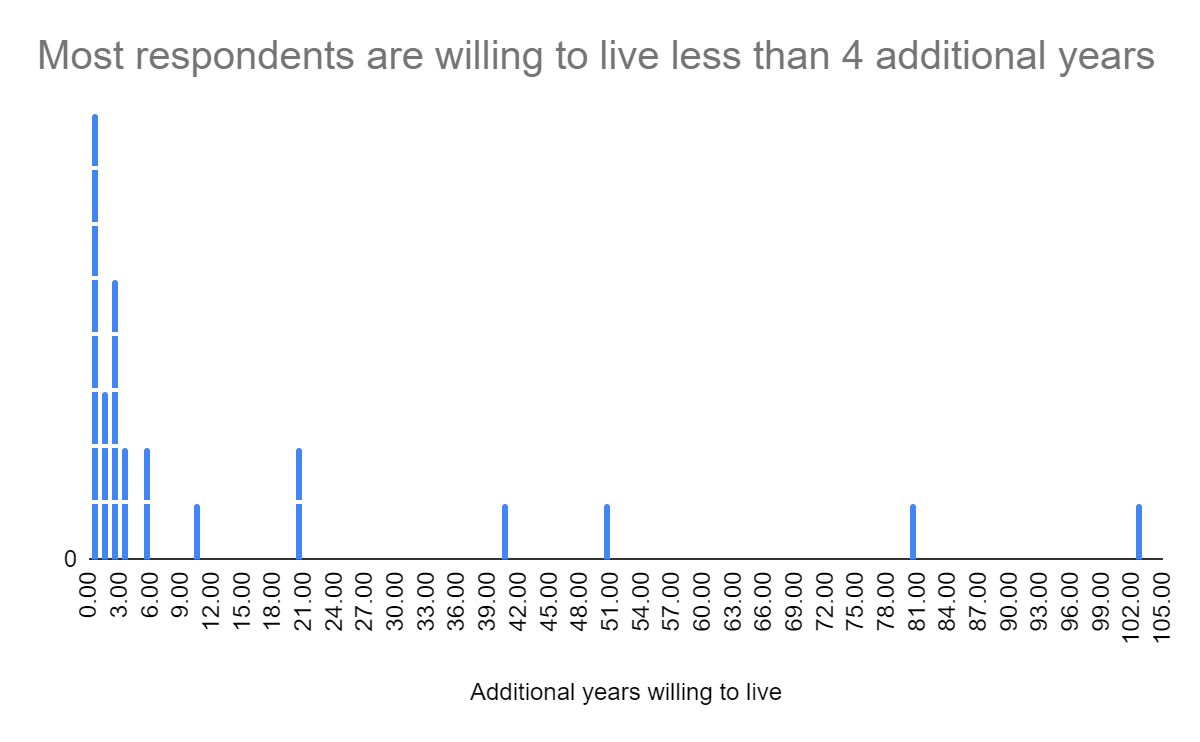
A small-scale (n=30) survey that I conducted in early 2021 in a Kenyan slum suggests that many respondents can value their lives negatively. Respondents were asked to label death and their quality of life on a visual analog scale (arrow) from the worst and the best imaginable situation. If worst corresponds to -1, death to 0, and best to 1, the average quality of life was -0.18, with a standard deviation of 0.40 (column AC). On average, respondents wanted to live 13 additional years (SD=26), while the median was 2 additional years.
The wording of the quality of life questions and their survey context can be assessed as leading, which can suggest low quality of data.
If you mai[n]tain your lifestyle and the future is what you expect it to be, how many more years starting from now do you want to live? You can say anything from 0 to forever.
Where do you place death on this arrow? Please put a line there and write "0." … Where do you place yourself on this arrow? Please put a line there and write "myself."
A local enumerator familiar with the area collected the data, while knowing that it is gathered for informational purposes only, without a possible benefit of answering in any specific way. While some (globally poor) respondents accepted a small stipend for their time (which is a custom in the area), many were happy to share their responses without a stipend. This can suggest that respondents answered relatively honestly, with little experimenter bias.
This survey shows that the quality of life in a Kenyan slum can be valued negatively by the respondents. The quality of life in areas of Kenya that are prioritized for malaria vaccination can be different in sign, for example due to urban-rural disparities. Further research on the expected sign of life quality of intended malaria vaccination beneficiaries (considering possible philanthropic and market co-interventions) can inform whether, when, and to whom GiveWell should recommend the scale up of this pilot.
Conclusion
GiveWell can consider incorporating a variable on the sign of the quality of life from the perspective of intended beneficiaries in their Centre for Pesticide Suicide Prevention and malaria vaccination analyses. The inclusion of this variable in GiveWell's analyses can inform whether programs that "save or improve" lives should be prioritized.
- ^
WHR "happiness" is a function of GDP per capita, social support, healthy life expectancy, freedom to make life choices, generosity, perceptions of corruption, and a constant (p. 19). Other possible aspects of happiness, such as family relationships and perceptions of fairness can be covered to a limited extent by this metric. I have not extensively reviewed the World Happiness Report methodology.
This will be huge if true. Fortunately it is probably not true. My guess is that you got the 30% figure from this quoted text:
My process is that I searched for "30%" in the linked article, here's the relevant excerpts:
(In context Givewell seems to assume a mean of 0.3% decrease in expected agricultural productivity, and a median of 0%. This is >=100 times lower than 30%)
I genuinely appreciate the reasoning transparency and epistemic legibility illustrated in your article that made it easy for me to pinpoint the presumed error.
TLDR: Sure, the 30% seems quite high, although if the price of alternative fertilizer is around double, it could be accurate for many subsistence farmers.
I have the 30% from this cited text and the BOTEC. In the sheet, 30% seems to be subtracted from the overall cost-effectiveness that considers qualitative adjustments (E77 in "Calculations"). "Calculations" E58 specifies 70% adjustment due to -30% due to risk of agricultural harm ("Assumptions" E36). This 70% multiplies other qualitative adjustments (E60), which multiply the cost-effectiveness before qualitative adjustments (E76) to get cost-effectiveness after adjustments (E77).
The number does seem high, though, especially considering that substitutes seem available. However, it may also be accurate, if farmers are able to afford less fertilizer due to its higher price. One Acre Fund (OAF) RCT-based analysis cites about 50% improvement in yield (in a different region) when farmers are given a loan to purchase (and trained to use) fertilizer and improved seed variety (fertilizer:seed cost is about 2:1[1]). Based on anecdotes from The Last Hunger Season, some farmers cannot afford fertilizer.
The price difference between the highly hazardous pesticides and alternatives is not stated, although pesticides constitute only 7.5% of input costs. However, the document (pp. A-12 - A-13 or 58-59 in the pdf) cited by GiveWell that gathers statistics on farm inputs considers relatively high costs for farm labor and land rent which in the case of subsistence farmers can be neglected (thus the cost would be much higher than 7.5%). There is also very high variance among states in India. Some states seem to use much less fertilizer (e. g. 2.5% of seed costs in Mizoram) than others (39% of seed costs in Andhra Pradesh). Thus, it is unclear to what extent any increases in fertilizer price affect yield.
Further, GiveWell cites that
Farmers in "The Last Hunger Season" were not trained in fertilizer use prior to the OAF program. It can be that farmers who pay attention to using fertilizer correctly will do so even if another type is offered and vice versa. India's growing network of rural e-centers with agricultural information can provide appropriate fertilizer information. In other countries of CPSP operations, farmers may be less informed. Thus, any decrease in agricultural productivity due to unfamiliar fertilizer use can be limited.
A professor conducted research on the substantiation of sentiments on counterfeiting. It could be possible that when a new type is introduced, farmers will be suspicious. This can be temporary or have limited effect (trust in local retailer not brand).
(More costly) fertilizer can also substitute other items that increase life quality, such as food, education, or health. Thus, even if a higher cost does not lower yields, the -30% (or other) adjustment could still be valid due to the effects of counterfactual spending.
I understand that GiveWell is assuming a 0.3 agricultural productivity decrease high estimate and 0 or 0.01 low estimate. The high estimate is used, while numbers with 0 decrease are cited next to the adjusted ones, possibly due to high uncertainty about the complex effects on agriculture.
So far, I only considered the effects on smallholders. Effects on industrial farms may be much more substantial, even if the price difference is in the order of percent. I assume that in India, most farms are subsistence. That should be 85% (by land holdings?) in Uttar Pradesh. I further assume that industrial productivity is about 5-10x that of subsistence farm (about 1/2-1/3 of land can be used in subsistence compared to commercial and productivity can be about 2-3x lower). This would suggest that commercial farms produce about as much (Fermi estimate) as subsistence farms (15%*5=75%≈85% or (15%*10=150%≈1.8*85%).
In areas where subsistence farmers use little chemical fertilizer, productivity decrease can be negligible (and much lower than that in commercial agriculture). Conversely, in regions where smallholders spend significant proportions on fertilizer, they can be affected disproportionately more than industries. The former suggests that the median would be close to 0 and mean would be the average of the commercial effects and 0 (e. g. 2% if commercial outputs fall by 4%). The latter can suggest a median value of >30% and mean value of the half of that.
The median would be 30% and mean around 0 if few farmers constitute a large majority of output and are relatively unaffected, while the majority of smallholders are affected significantly. This is what makes intuitive sense, upon the assumption that industrial agriculture largely outperforms subsistence in output and can flexibly (with negligible per unit cost) switch to alternative (or is already using it). However, this can be a biased perspective based on the knowledge of US and other developed economies' agriculture. While the rapidly industrializing India is the largest nation among CPSP partners, other beneficiary countries can be less industrialized.
Secondary effects from forgone commercial agriculture taxation (as well as any decreases in International competitiveness of beneficiary nations) that can support large proportions subsistence farmers could be discussed.
Lower fertilizer use could lead to higher rents accrued to farmers, if their product is sold as organic with a premium.
Another consideration is that CPSP on its previous website cited investigating the possible negative effects on agricultural productivity in Sri Lanka (listing this on the website can suggest a significant concern). This can be considered in conjunction with GiveWell's cited enthusiasm and great fit of the professor who leads the project/applied for the grant (he could be motivated to gather and interpret evidence in a way that highlights benefits and unhighlights risks).
The effects of highly hazardous pesticides on agricultural productivity (and the impact on populations) will depend on the
Guessing these values, measuring productivity in real local currency units and considering effects only on smallholders, based on the above discussion, the decrease can have a mean of 0.04 with SD=0.02 and be normally distributed, with possible other distributions based on country or region.
One Acre Fund provides $75-80 loans for fertilizer and seeds. 10kg of improved corn seeds costs 70,000 UGX. 10-15kg is needed for an acre (used 100,000 UGX or about $25). Based on the book and confirmed by Global Partnerships, the average farm size is about one acre. $25/$75=1/3, so about 1:2.
I should be clearer. Givewell did not assume a 30% decrease in agricultural productivity anywhere. The 30% reduction is to total expected value of the intervention from a 0.3% (by my inference, not directly stated) reduction in agricultural productivity.
This also seems inaccurate/misleading. From Page 40 of the report:
There are two issues with your summary, one minor and one serious:
That said, I did not consciously realize that average life satisfaction numbers are so low in Kenya/Ghana. This is helpful context for me, and makes the value of poverty alleviation efforts more visceral.
Thanks that makes sense! I did not realize that the average in Kenya for the IDInsight surveyed sample is 2.3. I appreciate my correction being corrected.
The IDInsight n from poor people surveyed in Kenya is 954 in case this is relevant to you. Appendix 1, Page 58 in the report.
woohoo thanks.
I was a bit confused about how the report said 4.5 for Kenya while IDInsight said 4.66 for WHR. My current guess was that 4.5 was for "happiness" while 4.66 was for "life satisfaction." However I could not find life satisfaction numbers in Kenya on a quick skim in WHR, will encourage other data sleuths to pick up the slack if desirable!
If we take both the 2.3 and 4.5 numbers at face value (and I'm not sure we should, but I don't have strong ideas otherwise for how to make donation decisions in the near future otherwise), one plausible interpretation is that average Kenyans are significantly happier than the poorest Kenyans. This will all else equal favor consumption and growth interventions over lifesaving measures (though of course there are many other considerations in place).
Yup, assuming causality.
I would be careful about simply increasing consumption and growth. More marketing (including that which highlights negative/abusive cultural aspects) could enter areas where identities are otherwise based in emotional navigation of relationships, which can be understood as deeply satisfying (these identities would be lost with increased societal attention paid to current globally competitive marketing).
Perhaps, this would start from an income level that would not be reached even with income doubled a few times, but, considering very affordable products, the Belt and Road Initiative, and growing marketing analysis and capacity in rapidly growing countries in Asia, growth without co-interventions can lead to an increased consumption of 'aggressively' marketed products, which may not increase one's life satisfaction.
This paper on cultural combination ('syncretism') from the South African University of Pretoria. There is little on the possibility of 'disturbing' pictures or arguably sexist bias-based and objectifying/physically judging advertisements becoming popular among some people. It is unlikely that the people affected by the marketing (even non-customers) would be interacting with humans of different cultures (but rather see the ads which do not respond to human emotional expressions).
People could be reporting an 'objective' life satisfaction, based on status portrayed in the ads, without emotional introspection. It is possible that they would not report dissatisfaction, because that would mean decreased competitiveness, which, based on some advertisements, could be associated with one's vulnerability or undesirable situation/identity. This is just a hypothesis.
Also, the lives of the poorer persons can be worse because of the norms that they grow up in (for example, threatening of neighbor's life for $3, sending children to work or beg from a very young age, defaulting on a group loan, ... vs. going to different neighbors for humble meals weekly, trying to put children through school, vetting microfinance firms and contemplating the EV of an income-generating asset lease).
The argument is that if you increase the (for instance) children's who grew up begging income, it does little for them because of their upbringing (it may be difficult for them to form enjoyable relationships because they are used to a lot of unwelcomingness). A better approach would be education in locally relevant skills so that they can be (considering the situation) welcome since a young age.
An alternative thinking is that the people who had limited opportunities when they were young would be super grateful for the improved opportunities and will educate their children so that they do not experience low life quality rather than approaching them as people would approach a begging child (illustrative example of gratitude of situation improvement - actually life saved - from an island I've seen). This suggests that the present adult generation should be targeted with consumption increase programs rather than children educated. Saving lives, at least by caring individuals sincerely interested in the saved people, can be actually also valued.
Still, at least some budget should probably be allocated to the "other considerations," just to make sure that it is not that, for example, men who beat their wives and women who would perpetuate the normalization of beating are not just going to get more colorful washing baskets with 'women overpowering men by using the product' for the women. I argued similarly here.
The 4.5 is footnote 30 in the HLI summary.
This is a bit of a digression, but I would generally recommend against
a) linking the original source directly if you've only read the summary (instead you should probably cite/link the summary first), and
b) (although this is more work) generally trusting summaries for data/figures without doing quick epistemic spot checks on on the quality of the summaries.
a) While in formal writing, there are specific formats of citing others' citations, in this context, I decided to link the report directly, alongside with this comment thread that reads
In this comment, the HLI's Estimating moral weights page (with the footnote) to which I referred several times in this thread is not referenced, because I assumed that those who read this thread carefully are already familiar with the page and those who are quickly skimming do not need to be distracted by that link.
I am keeping in mind that this is the Change Our Mind contest. Citing HLI could be read as an intent to convince GiveWell to implement HLI's framework, which they are familiar with, by repetition. WHR allows readers to form and update their opinions based on data which does not intend to change GiveWell's mind. Thus, WHR can change the mind of an evidence-based decisionmaker better.
Further, historically, GiveWell has used top statistical evidence to make its recommendations. WHR enjoys similar level of comprehensiveness as RCT-based research, while HLI's research is more speculative. Thus, WHR can allow GiveWell to change their mind more consistently with its fundamental values than HLI's research.
b) I have not checked the Report, but rather deferred to HLI's standards of citing statistics. I reviewed some papers cited by HLI and did not find inconsistency (other than the vague sample size interpretation as further above in this thread). This can be understood as a form of a spot check.
Nevertheless, I searched for the statistic in the 2019 WHR. (I used the search function for "4.5" and "Kenya".) "Kenya (4.509)" is cited as the value on p. 29 of the WHR pdf (pp. 26–27 of the document). I added the page reference.
This actually leads me to the methodology of the WHR. It seems like 'happiness' is a function of (pp. 26–27):
Although this can cover many aspects of happiness, other factors which could influence this metric (including by changing its sign), such as the normality of abuse or parental acceptance/rejection, do not seem to be included. WHR 'happiness' can thus measure governance quality and public cooperation rather than seek to understand intended beneficiaries' quality of life. However, further research is needed.
I also added a note on the interpretation of this metric.
Thanks for this. Understanding how prospective beneficiaries value their lives is difficult but important work. It seems a reasonable assumption that people who attempted suicide would lead negative lives. However, I think we can do better than resting on this assumption, and I think deeper analysis suggests this assumption is false.
Here's CPSP's answer on their FAQ in response to 'Should people who want to kill themselves be allowed to die?':
As a start, most people who have a non-fatal suicide attempt don't attempt again. This article suggests the broad pattern following a first non-fatal suicide attempt is ~70% don't attempt again, 20% attempt but don't succeed, and 10% commit suicide.
I couldn't find much that was directly relevant to long-term quality of life, but this very small French study looked at 29 adolescents who had attempted suicide, and followed up 10 years later (with significant potential for selection bias - only two thirds could be traced and of those, two thirds responded). Over 75% said they were happy in their personal lives, over 50% were satisfied or very satisfied with their professional lives, and 2/3rds had no significant psychiatric problem reported. 17% had an ongoing chronic psychiatric problem, and 14% were in-between these groups.
This study looked followed up physical trauma cases in adults - they found 65 patients who had the trauma due to a suicide attempts, and followed them up at 6+/- 3 years. 14% had died before follow-up, none due to suicide and all were reported as coping well by next-of-kin. 3 patients couldn't be traced and 2 declined follow-up. Psychosocial measurements of follow-up patients suggested a majority had decent functioning, with around 20-25% experiencing severe impairment of some kind. None had re-attempted suicide.
I suspect that the key determinant of quality of life after attempting suicide is mental illness, especially depression, and not the suicide attempt itself. But I'm uncertain about this, and even more uncertain given both the literature and my clinical training are based on a high-income country context - things could be very different in low/middle-income countries or those in absolute poverty.
Thank you. I think so. I think that in high-income contexts, depression can relate to one's loneliness and use of social media that use negative-emotions marketing as well as abusive/neglecting/rejecting family relationships (that the media (and people influenced by them) can draw from (and make one to assume as reality)).
In many low-income contexts, it can be argued that people are not as lonely, because agreements are based on community accountability (which requires mutually enjoyable or overall approved emotional navigation) rather than sound rule of law and business relationships are founded in friendship (gaining customers for undifferentiated goods). Also, in low-income countries family can play a key role. Forced marriage, female and child abuse norms, FGM, limited family planning can all worsen one's mental health.
The key difference between high- and low-income countries can be that in high-income countries the negative perception of one's relationship-related situation and limited enjoyment of others is motivated by media, while in low-income countries perceived due to actual and 'necessary' abuse (e. g. someone has to be beaten to make bidis because otherwise productivity would not increase).
A related thought is that if (low-paid and unpaid) productive people in low-income contexts suicide, the productivity decreases, ceteris paribus.
An EA who studies India's media commented that the show of suicide in the TV is banned, because it increases suicide rates.
My small-sample study shows that some people can perceive their life quality below death, wish to live 0 additional years, and still live. I did not research suicide but the local enumerators, an elder, and an educator have not commented on it.
It can be hypothesized that the willingness to suicide is a part of a 'dialogue' between the 'abused' and the 'abuser,' used as a means to argue for more favorable treatment. It can be a statement that it is unacceptable to, for example, beat people for no perceived reason. Related concepts are described in The Wretched of the Earth by the psychiatrist Frantz Fanon.
The ability to suicide can increase people's willingness to 'lead this dialogue,' which would otherwise be unthinkable, and thus (at least 'during the discussion') lower their quality of life. It can be assumed that this will have limited benefits, since external education and investment rather than internal redelegation of tasks is needed to highlight enjoyable cultural approaches and enable productivity without (human) abuse.
This would suggest that limiting the use of highly highly hazardous pesticides can improve the mental health of people (there is no need to feel emotions that intend to lead to the improvement of their situation when they can themselves very little about it). However, it can also be argued that once people know about suicide, but are prevented from it, their mental health decreases even more significantly, because they are perceiving the 'trap' of having to live in an abusive situation without the ability to affect this for themselves or future generations.
I am actually not describing depression as you may be understanding it: "persistent feeling of sadness and loss of interest," which can occur when (I am not medically trained and am only suggesting ideas rather than intending to describe a medical condition) people feel uncompetitive/without the ability to become competitive, not needed/without unique skills (not considering individuals), or not bought in on the meaningfulness of hobbies/without developed interests.
I am describing 'depression' that is based in one's knowledge of being abused due to one's identity and inability to do anything about it, having urgent (family) issues that no close ones help with and one cannot resolve (for example, my research suggests that people would give up, on average 78% of their remaining life if 'people around them cared about each other's problems' - but in context, people would give up large fractions of their life even for nutritious food, insurance, etc), cultural limited presence of/training in love, and limited prospects for improvement of one's family situation.
Perhaps, the anecdotes on the CPSP website can be understood as 'weird' by people around the 'story tellers.' Most people understand the situation and just go with it. Suicide causes issues to the family.
Thus, the "assumption that people who attempted suicide would lead negative lives" should hold, if one looks at the situation from the perspective of one in the situation who assumes that their emotions can lead to a change or authority/peer understanding or from the perspective of someone not 'at peace' with the situation. This assumption would not hold if people are at peace with their roles/situations and depression is defined as the limited need to emotionally negotiate relationships.
I emphasize that I just wrote some ideas, which can be not indicative of anyone's perceptions, based on my limited understanding of the intended beneficiaries and non-beneficiaries as well as understanding of some resources. Persons and their attitudes are individual. When I hypothesize a commonality, it can not hold true, can apply only to some, be taken out of context, and have other interpretations.
Thanks for your entry!
Sleeping under a bednet or getting a malaria vaccine are optional activities; people are free to choose to do that or not. (This is not quite accurate for children, where the decision probably lies with their caretakers.)
In post-distribution surveys, AMF consistently finds that most nets are being used as intended. People know that the nets protect against malaria. They also know the sickness, probably had it before, probably know someone who died from it. So it's an informed choice.
Based on this kind of observation, it seems to me that most people want to live. My personal, subjective, moral view is that it would be wrong to assign a different moral weight to their lives.
Let me challenge you here. Suppose that in a community inspired by Tsangano, Malawi, where people used 71% of nets which they freely received, the quality of life is -0.2 with an SD of 0.3 (normally distributed). 60 km away, in a place visually similar to Namisu, Malawi (where people used 95% of nets), the quality of life is 0.3 with an SD of 0.2. Each community has 2,000 people (who need about 1,000 nets). You have only 500 nets.
Who are you going to give the nets to?
Further challenge: You also have a pre-recorded radio show that improves farmers' agricultural productivity by coaching them to place only 1 grain 75 cm apart and cover with a few cm of soil rather than scattering the grain. This can increase people's productivity by an average of 20%. The airtime for the show in one community costs as much as 500 nets.
Are you going to forgo any nets and buy the show?
Are you subjectively assigning equivalent moral weights to the lives of the people in the two hypothetical communities?
(disclaimer: I work for AMF, but this is my personal opinion)
Yes, we have to prioritize. No, life quality seems the wrong metric for prioritization.
A few practical responses to the challenge first: AMF funds bednets at the scale of countries or provinces, that is, a few million nets at a time. This allows for efficient distributions that leverage economies of scale. Prioritization takes a number of factors into account, such as malaria prevalence (which might have an effect on the bednet use rate). Life quality metrics are currently not a factor for prioritization, as far as I know.
Re the challenge: I think you'd have to consider that life quality goes up as a result of the intervention. It might go up more in areas that start from a lower baseline than in areas where people are already better off. It's important to note that bednets (or, for that matter, most interventions) are not purely life-extending interventions. They have a variety of other benefits:
A final question: you keep using net-negative lives in your examples, yet people are accepting help, voluntarily. This seems to indicate net-positive life quality. How do you think about that?
Thank you. This actually makes a lot of sense. The farming improvements (although could be different in different areas and studies) are astounding. For example, One Acre Fund increases farmers' annual income by about $100 or 50%, for the cost of about $25/farmer in 2021. Bednets have an equivalent nominal impact for about a fifth ($5) of the price.
Sidenote: the lower % improvement suggests that AMF serves relatively affluent farmers (with average annual incomes of $633 ($76/12%*100%), which can have twice to five times the real value) (unless the $76 is real value).
The agricultural productivity can increase because people are less sick and more productive. Also people could have a greater capacity to seek better farming practice information, livestock could be less ill (if bednets are used to cover livestock), and fishers could have better equipment.
Also, children could be able to help with chores rather than occupy parents or older siblings to care for them. Reduced treatment spending can be also substantial. Assuming that malaria treatment costs $4 and a bednet prevents 2 cases of malaria per year, then a family with 5 children (who would be treated if they get malaria) can save $40/year, which can a substantial proportion of their income.
In terms of attendance, bednets can have limited effects (about an additional week of school per year?).
That is about 10 days/year. If a bednet prevents half of the cases, that is 5 days or a week.
The impacts on enrollment can be relatively larger due to the increased farming income and reduced treatment cost if education expenses are substantial. For example, if education costs $100/year, then an additional child can be educated. If education expenses are close to zero, then malaria does not affect enrollment.
The quality of education or its relevance to employment is not directly addressed but can be addressed indirectly by enrolling a child in a better (higher paid) school.
Reducing mortality can have positive impact on savings and investments due to the reduction of funeral costs, which can constitute a large proportion of a family's annual income.
I am not familiar with the research on long-term health improvements. I imagine that early treatment of cases that would be more severe, especially for young children, is a key factor. Prevention reduces the rate when this would be needed.
--
Ah hah hah, yes, it is "net-positive life" but perhaps not life quality. Let me show you some of these videos:
People in a slum, possible abuse and neglect in spousal relationships, FGM, FGM and family, some parents decide that their child cannot live, and sending family members for life-long shrine work.
These are just arbitrary examples that show abuse, neglect, and addiction, mostly from countries that AMF does not operate in. It is possible that similar situations exist in some areas of countries of AMF operation.
The argument that in these situations, people can feel worse than if they were dead.
On a positive note, there are also very chilled environments where lovers get married as well as officials who support consideration based on reasoning.
Although currently you do not consider life quality factors, you could use these factors to put pressure on governments to advance legislation and governance that prevents dissatisfied lives, such as by banning FGM, forced marriage, or ritual servitude.
Even if additional measures are needed to improve life quality, considering these factors can be a statement that AMF, a large player, communicates. Implementing an somewhat sophisticated metric (such as a weighted average with some exponents) can engage officials in calculating what legislation and agreements would net them the most nets (haha), rather than using blame or other negative motivation to achieve the same result.
Preferring life satisfaction (or its proxies) statistics and expert estimates can have positive effects on governance/institutional decisionmaking of AMF partner countries and regions, such as the development of government networks of people familiar with the concepts (and interested in the improvements) of life quality measures and the government's interest in quantifiable impact.
Not to bother you anymore, but if a government decides to give its 1 million nets to its worst slum and leaves the people who seem to have all they need (except maybe bednets) uncovered, that's actually equally great as vice versa, and better if malaria rates in the slum are 10% higher than those in the countryside, because more children will be able to survive and people will have more for daily spending. Right.