I agree with you that practising medicine is not very impactful, and that community building in medical schools in some countries (e.g. Australia/DE) is useful. However, I think you're way overoptimistic about the value of a medical degree. Since that's our disagreement, that'll be the focus of my comment. Most of it will be line-by-line reactions to your arguments, and then I sum up a bit, and comment on outreach at the end.
Line-by-line comments
Impact of EAs after med school is more robust to EA meta risks (e.g. cause X existing, EA running out of funding,...) than when specializing earlier during university on cause areas (80%)
Specialising into EA is very non-robust to new cause areas, because it is a severe narrowing that happens early. And how many more billions do EAs have to make before you stop worrying about it running out of funding?
Is becoming a doctor a high impact career path? No, I personally don't think so
I'm not sure it's a matter of personal opinion. Greg has convincingly argued the opposite.
In contrast to specific knowledge of pathologies, the fundamental knowledge treated in med school of natural sciences, biological sciences but also sociology/psychology will likely be highly relevant for all of the above cause areas.
A medical degree is about 1/4 as dense in fundamental science as a science degree, because it only makes up about half of the non-clinical years, which in turn make up only about half of the program.
Furthermore, it is possibly taught with better signal-to-noise ratio than in other degrees as med school has to focus on the parts of the knowledge relevant for translational (i.e. practical big-picture) applications in humans and medical systems. (again, with large variation)
Most of the EA roles need biomedical science, and there's much less of this in med than in a science degree, because the medical degree is busy teaching you how to be a doctor. What's not spent on clinical medicine is often spent on memorising things that are not very broadly relevant, like anatomy, pharmacology, maybe medical ethics, medical law. So I would say the signal-to-noise is much worse.
This kind of big-picture thinking and problem-solving is fundamental in medicine and in my experience often overlooked in other hyperspecialized degrees, despite being highly relevant for any impactful EA endeavor.
Basically every degree can arguably give you special translational skills that help you to be a good EA. Math, law, and philosophy degrees "teach you how to think". Med, engineering, and business "teach you how to solve problems". But what is actually relevant is usually science and computer science.
a PhD usually takes another 3-5 years after Bachelor/Master studies in other career paths.
This is not the right comparison. A medical degree doesn't help you to do many of the things that a doctorate does.
in some careers [a medical degree] will offer a notable amount of additional credential boost just by being considered 'a physician’ or even ‘a doctor’ such as e.g. in public or political work
It's not actually that useful in my experience, especially outside Australia/DE. People care a lot more about whether you can actually do the job.
All three of these are largely independent of the specific choice of your degree if you are the type of person open to networking and meeting people outside of university classes, so I would say that the choice of the city/town that you will be studying in matters more than the degree itself.
But all things being equal, it's much better to build a network of people who study higher-impact topics.
'Standard EA advice'[4] for high school graduates (never go to med school, go do something more directly relevant for known x-risks) is currently based on a lot of assumptions: - we are right about the current setting of priorities and cause areas - we have not missed any further cause X
It definitely doesn't rely on these assumptions. If we new that the most impactful causes would by currently unknown to us, I think they would be more likely to be far away from med, which is a relatively narrow field. Think of previous crucial considerations: AI risk, anthropics, simulation argument. Not things that are particularly amenable to approach by a medic!
- EA will continue being able to pay all people wishing to do so for work in niche and formerly neglected causes
It doesn't assume EA will be able to pay all. But EA will be able to fund most who are smart enough to be admitted to a medical degree in Australia or Germany. The contrary was reasonable to worry about a decade ago, but the funding base has grown and diversified so much since then that it's really not defensible anymore.
- EA will continue being able to raise funds faster than people
Even if we gather a lot more people, we could allocate them to do things like policy that are funding-neutral and very useful, before we allocated people toward med.
indefinitely have quasi-unlimited funding by a handful of software dev philantropists (which assumes:)
The crisis would have to reduce the holdings of half a dozen billionaires by 95% all at once. And even then, there's things like Founders Pledge, GWWC pledge, and finance people, that also collectively hold billions of dollars of wealth. Not plausible.
While I generally remain cautious while optimistic when eyeing the above, I would propose that a medical degree and the breadth it provides can make your positive impact more robust...
No, once again, medicine is a very narrow degree.
Furthermore, the incredible job safety of a medical degree always offering a comfortable plan B can be a source of confidence when later engaging in high risk high reward career paths such as EA-aligned charity or biotech entrepreneurship.
In my experience, all that was useful was to earn a year's runway, and funds or . I spent about two years doing that. Then, I had to leave Australia to study. I maintained my medical registration for another year, by travelling back and practising briefly, but around that point it became clear that I was not going back to it. If I could have the time again, I would definitely have tried harder to apply for funds to drop out of my medical degree and study something useful. All up, this would have saved me about six years. Now that we are in an environment of such persistent and robust funding abundance, there is really no excuse!
Summing up on Medical Degrees
First, let's look at your summary, then I'll give mine.
So - Is going to medical school generally a high impact choice? What I have been aiming to show is that it is not as clear-cut. If medical school prepares you for a high impact career or not will largely depend on the country, city and specific university that you are doing it in: the extent to which course content is transferable to high impact careers, the workload, the extent to which you will be forced to study irrelevant knowledge (largely specific pathologies), the degree which you can be getting in the end, the opportunities for extracurricular activities, the networking opportunities.
I would say the main advantages of medicine are that you'll meet some smart students (some network), and a steady income stream. But it's far worse than the best courses. It's a narrow course, with less than average transferable knowledge. So it provides you with less optionality than, for example, a science degree. The workload is among the highest, so you will have fewer opportunities for EA-related pursuits. The content usually has less elective material than other courses, so you will be forced to study more irrelevant material. Your network will be suffering from these problems too, so they will be somewhat less likely to pursue high-impact roles than the smartest kids from a science degree.
For folks who are already in a medical degree and are very into longtermist EA, I think it depends to a fair degree how suited you are to working on biosecurity. If you are, then you might want to finish the degree. If you're not, you might not - you should check that you're not going to run into visa-related problems, but instead you could pursue a direct-work role, a startup project, or a masters degree. Other caveats include that you often need an undergraduate degree to enter a masters program, and to get a visa for some countries, so this is worth checking into, and existing with a BMedSci is often desirable, if possible.
Thoughts on Medical Student Outreach
I think outreach to medical students is not a bad idea. If you're going to allocate 3% of EA's outreach efforts to Harvard, then you probably should allocate at least 0.1% of efforts to medical students in Germany and Australia, or something. The point is that in these countries, there is a nationwide school-leaving grade, and the most competetive courses tend to be medical degrees, so they attract a lot of top talent - the sort of people who would go to Harvard or Oxford if they were born in those respective coutnries. Naturally, many of these folks will be interested in EA ideas, and could benefit from being connected to them. And biorisk is something they can help with (although by my reckoning it seems >30x less important than AI risk), along with perhaps other brain-related topics. But it's tricky, because you're naturally pitching these students on something that goes quite against-the-grain for their cohort - leaving their degree, leaving their field, and so on. Much moreso than what we ask of computer scientists, for example. But still, it seems worth a shot.
Great to hear that you agree with most of the post (two out of its three main points), let me focus on the disagreements regarding the impact potential of choosing to go to med school:
As far as I can see, you raise three general points of disagreement. (do let me know if you don't feel like I represented your points well)
Disagreements based on personal experiences with studying medicine in Australia
Disagreements regarding the value/transferability of knowledge taught in med school for high impact work
Disagreements regarding the relevance of EA meta risks (funding dependencies, cause X, etc.) and whether a medical degree actually makes you resilient against these
Regarding 1) Disagreements based on personal experiences with studying medicine in Australia:
I think some of the negative aspects you describe about med school are very important but might not be general to all medical degrees. I'll give some personal examples just to show that I disagree that your descriptions are generally accurate, of course you might actually be right in the majority of cases.. I do not have a good intuition if the median medical school internationally is more similar to the one that you describe or to the counterexamples I offer!
You write of highest workloads, few electives, all for a medical degree with no doctorate. (and that networking opportunities suffer from all that) I see how all of this is generally sub-optimal for high impact career paths, such as the research career in AI safety that you're currently pursuing.
Credentials
This is not the right comparison. A medical degree doesn't help you to do many of the things that a doctorate does.
In Germany, as an option additional to the medical degree ('Staatsexamen') , most medical schools offer a Dr. med. (MD) degree track and some offer an advanced MD/PhD track (e.g. here). Both of these are considered a doctorate and are a very good foundation on which to build a career in research/academia or to go into industry. (given sufficiently good grades on either, with the MD/PhD generally being more valuable)
Electives and workload
15% of my modules are wholly elective, two further semesters offer longitudinal electives. I am sure that a lot of degrees offer way more, but I consider general workload being reasonable to be even more important.
Because, in my experience the workload is actually not that high in some medical schools, such as mine. A lot of my friends/acquaintances studying fundamental/applied sciences degree at elite universities such as Oxford or ETH Zurich have much higher workload. This means that the majority of my time is 'elective' in that I currently have enough of it to use it for 1) being main organizer and founder at my uni, 2) a research assistant job at a lab and for 3) things such as writing this post (and I am currently actually in the most time-intensive year). I know that this would not possible to this extent in all other courses that I could be doing.
2) value/transferability of knowledge taught in med school
It is hard to say how much of the disagreement here arises from uni to uni differences in course structure and how much is more about theories of value of knowledge.
First, regarding uni to uni differences: Of the 40 modules during my 5 theoretical years, only 9 focus on specific pathologies (and related pharmacology, etc.). A lot of the rest does contain knowledge on pathologies, pharmacology, etc. but always embedded in a general, translational framework which furthers understanding of the human. It might be that this is more focus on transferable knowledge than in the median course.
Re theories of value of knowledge: Since you focus mostly on transferable knowledge for research: From the experience that I gathered so far, academic research requires deep specialization in very specific methods researching very thin slices of reality, all of which with a depth that goes far beyond any course curriculum. This means that learning and special knowledge beyond uni material will always be necessary for academic research. While fundamental science degrees may arguably make this easier (especially the more fundamental the research is), knowledge from a medical degree will rarely make this further work impossible! It would be interesting to know how much harder you'll have it with a medical degree and thus how big this cost is but right now I am not convinced it is big enough to make me update! (The fact that you did manage to specialize in AI safety at FHI, Oxford with a medical degree is a nice anecdote in this regard that I couldn't help noticing)
Furthermore, over here there is the option of specializing into research and starting your doctorate as early as 2-3 years into the course, which could arguably make your specialized knowledge & fit for a specific research direction by the end of med school much better than that of someone with a general fundamental science degree. This is again of course something that will vary from uni to uni.
Lastly, when it comes to potential high impact career paths outside of research such as policy, entrepreneurship, (industry?) I suspect that we have a similar general picture:
Some more specific degrees could have arguably been an even better fit in terms of knowledge, but some aspects could yet again be in favor of the medical degree: e.g. translational understanding and firsthand experience of health systems on all levels, trained social skills, credentials of being a doctor (which is might be more of a thing in fields outside academia), job/income security allowing for time for other things etc.
And of course, the last point about income/job security is dependent on:
3), Disagreements regarding the relevance of EA meta risks (funding dependencies, cause X, etc.) and whether a medical degree actually makes you resilient against these:
Funding
You might be right that there's nothing to worry about in being dependent on EA funding due to historic successes in getting funds and the funding diversity you speak of. However, my own prior is generally quite low when it comes to placing trust in getting funds without problems, even when being 'smart enough to be admitted to a medical degree'. I've got some more to say about this topic but I to some more research/thinking on this specific aspect and then write another post discussing it in a more general context!
Cause X / Resilience
I think you might have changed my mind on this point while I was writing this reply. Here are my thoughts: Regarding the question of how well a medical degree prepares you for cause X:
I agree that we can not assume that a medical school graduate is magically better suited for cause x, however I personally believe that EA right now is too focused on narrow quantifiable causes (due to inherent uncertainty of anything that's broader) and focused too little on general resilience-building. (Here are my rough thoughts regarding this)
I was going to say here that while potential future high impact resilience building efforts don't necessarily have to relate to medical fields, a broad degree such as medicine will be more likely to be valuable for them than a narrower one such as a specific fundamental sciences degree. However I think you raised a good point in that some fundamental science degrees such as e.g. physics or biology are actually broader than medicine in important ways and might thus arguably be more valuable/applicable to future high impact resilience building efforts. (at least in my current abstract understanding of the term)
This is something that I would like to think more about and that I will reserve my judgement on for now!
I hope I could give some more perspective as to why we disagree on some points, overall you did cause me to update regarding my views on a medical degree resilience, potentially causing me to update on the value of spending time to apply for unis abroad after all! Let's see! ;)
PS:
I'm not sure it's a matter of personal opinion. Greg has convincingly argued the opposite.
A very small fraction of MDs are admitted to joint MD-PhDs. A medical degree is the only one that can come with optional extras - in many other degrees a similar fraction of students would be publishing papers with supervisors. And the PhD that a medic does will not necessarily be as relevant as those of a computer scientist. Basically, it seems like a way of avoiding an apples-with-apples comparison.
15%-elective is terribly little.
Note that the workload may skyrocket in the clinical years
Regarding (2) transferability: I believe you're overthinking it. From a zoomed out view, medical classes are approximately useless, and this talk of a specialised class becoming useful by being "embedded in a translational framework" is basically waffle.
You understate the case for the usefulness of useful subjects. If I'd studied computer science for undergrad, I could've got where I am now 5+ years earlier. Even dropping out of medical school could have accelerated things. In such a scenario, I could've been a somewhat more credible applicant for things like top professor positions than is currently the case. (Of course, skill is the main thing, but getting promptly educated, and building a stellar CV at a young age does help, vs studying irrelevant subjects).
Regarding (3) funding
my own prior is generally quite low when it comes to placing trust in getting funds without problems, even when being 'smart enough to be admitted to a medical degree'.
What kind of evidence would make you update your prior? Many funders say they are willing to fund any person doing excellent longtermist work, and many orgs are continually growing and hiring. To take one extreme example, $50k fellowships are being given out to interested teenagers. It's a movement that's >10 years old, with its funding-base growing double-digits per year. If you're smart enough to get into a German medical degree, and dedicated, then it should be possible to do excellent work...
A very small fraction of MDs are admitted to joint MD-PhDs. [...] in many other degrees a similar fraction of students would be publishing papers with supervisors. And the PhD that a medic does will not necessarily be as relevant as those of a computer scientist. <
It being a small fraction doesn't make it less viable for an EA approach to studying med school. Every EA approach to uni will incorporate some tight admission rate..
It might not be relevant for AI safety but it will be super relevant for e. g. neartermist EAs or EAs that don't rank AI risk as high and want to focus on biorisk.
I believe you're overthinking it. From a zoomed out view, medical classes are approximately useless, and this talk of a specialised class becoming useful by being "embedded in a translational framework" is basically waffle.<
We do not have 'medical classes'. We have classes on systems of the body: foundational classes (biochemistry, molecular biology, physics, physiology)
and classes that incorporate practical info, where you would argue they're approximately useless such as pharmacology. I disagree that they are entirely useless as it teaches you on a daily basis how the fancy science translates to practice, a skill that I will continue to argue is highly important (and at the core of any problem solving inside and beyond academia) and a skill that a pure fundamental science degree is 'approximately useless' for.
funding
Fair points, as I said, I reserve my judgements here for now..
Thanks for writing this. (I admit to skimming parts.)
Two things that I think are also worth mentioning:
Having an MD provides substantial job security, at least in the US. If a doctor takes a year off to pursue a risky project, they can return to medicine if it doesn't work out. I think in most other fields, a random one-year gap could make it hard to return to the workforce at a similar level.
It's relatively easy to scale (most types of) medical practice up and down. Some PCPs only have two clinic days a week; some surgeons only operate once. You can make a decent living practicing medicine part-time, which can free up time to work on other projects, even without pay.
This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
Disclaimer: Although I work on the Groups Team at CEA, I’m writing this in a personal capacity, and this post does not constitute an endorsement by CEA.
Agency - the realisation that you really can just do things.
TL;DR
Biosecurity needs people (of any background) who are agentic and have a high execution velocity and track record....
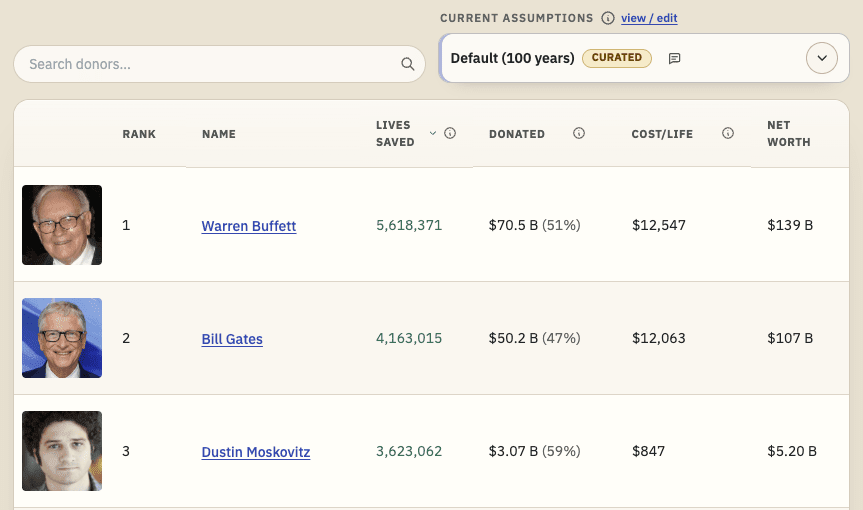
TL;DR: I'm releasing a website that ranks philanthropists according to EA principles and research, and allows users to re-rank the list using their own assumptions. I'd like feedback and help making it better. I'd especially like ideas for how to make the results more trustworthy. Funding may be available.
I recently built Impact List (impactlist.xyz), a site which ranks people by their positive impact via donations.
The goal is t...
Full Disclaimer - Since the writing of this post I have significantly changed my opinions on global priorities, most affected by changes to my epistemic and moral views. I currently believe that opportunities/risks from misaligned superintelligent AGI dominate relative importance of global priorities and have thus updated away from recommending medical school as a high-impact college degree. For that reason, I am myself currently planning to transfer out of medical school - I am planning to soon write a more detailed post on my reasoning and advantages of transferring aimed at members of the EA med student community, DM me now if you're urgently curious.
Intro
TLDR:
Is Medical School High Impact? I think there are three independent questions to this that are all important & which I will discuss in this post. To give an overview, here are my related core claims/conclusions regarding these questions and my level of confidence in them: [1]
Is becoming a doctor a high impact career path?
Becoming a doctor and just doing clinical practice is generally not a high impact career path (95%)
Doing medical school ≠ becoming a doctor & doing clinical practice (99%)
Career change in medical school due to EA med school community building ≠ people still doing clinical practice but more effectively (99%)
Is going to medical school generally a high impact choice?
Medical school generally can work as a foundation for a lot of (non-clinical) high impact careers (90%)
Cost/value of medical school (trading time against knowledge, experience, network, credentials) significantly varies among countries/med schools which is a deciding factor in if it can be a high impact choice (80%)
Med school can be a high impact choice under some circumstances for some EA students looking to maximize their impact (80%)
(I am not saying that medical school generally is the best or among the best choices for all students looking to maximize their impact. I think it depends on specific circumstances of the specific curriculum, city, world models etc.)
Impact of EAs after med school is more robust to EA meta risks (e.g. cause X existing, EA running out of funding,...) than when specializing earlier during university on cause areas (80%)
Is EA community building in medical school high impact?
Community building in some medical schools can be a high impact/cost-effective use of EA money (80%)
and it is high impact in all medicals schools (65%)
and it can be high impact even under the assumption that medical school generally is not among the best university course choices for high impact careers (75%)
Why I am writing this & possible bias
I am founder of High Impact Medicine Berlin and medical student, whose aim is to maximize their impact. The validity of my current life choices sort of depend on med school being one of the best paths towards maximizing impact, so I am likely biased. I think I can still offer convincing reasons of why med school can be high impact under some circumstances, which I want to outline in this post.
I have been thinking and discussing around this topic for a while and I write this post motivated by the recent discussion on the impact of the newly founded High Impact Medicine (HiI-Med) movement & the points raised by Gregory Lewis in response to therecent post on HiI-Med.
Is medical school high impact?
To start, I think it is crucial here to differentiate three questions which are different from each other (yet interrelated):
Is becoming a doctor a high impact career path?
Is going to medical school generally a high impact choice?
Is EA community building in medical school high impact?
Is becoming a doctor a high impact career path?
No, I personally don't think so, if we take becoming a doctor to mean 'pursuing only clinical practice as a career' and high impact career path to mean 'one of the (top 1% - 0.1%) best possible career paths in terms of long-term positive impact'.
Gregory Lewis has written an excellent post series on this topic in 2012:
Is going to medical school generally a high impact choice?
The default choice after medical school
Most people going to medical school will go on to become doctors and pursue clinical practice. The primary purpose of medical school is to provide the education/formation for this. In this sense, medical school is generally not a high impact choice.
However, becoming a doctor after medical school is not obligatory and many people choose to pursue career paths after medical school which do not incorporate clinical practice. There are many med school graduates outside clinical practice doing high impact work within and outside EA.
We can frame this as the default career path after graduation being low impact, with EA-inspired deviations from the default path potentially offering higher or high impact careers. In this light, the situation at medical school is essentially similar to all other potential university degrees, where the default/modal career path also won't be high impact. Things get interesting if we consider how well medical school 'prepares' you for high impact careers relative to other university courses.
How well does medical school prepare you for high impact careers?
Does medical school offer a good foundation for work in high impact careers? Is medical school among the top choices when enrolling for a university degree?
I think it depends.
I model university as a trade of time against knowledge, skills/experience, network and credentials. Let's assume that generally, it is worth going to university to make this trade to some extent for many/most people aiming to maximize their positive impact. How good is this trade when choosing med school and the relevant question is, how good is it in comparison with choosing an alternative university course?
Knowledge, Skills & Experience
Generally, medical degrees primarily aim to teach the normal functioning of the human body (physiology), the variety of ways that it can break/dysfunction (pathology), the ways to diagnose and treat that with an evidence-based approach grounded in biological and clinical research.
Beyond that, there is a lot of variation between countries and between universities. Some have a broader focus on physiology and the underlying biochemistry and biology while other programs will focus on early specialization on specific groups of pathologies. Furthermore, the quality and the extent to which a course focuses on e.g. societal/sociological/institutional factors for human health or scientific/clinical research can vary a lot, too.
Of course, there is large variation on the specific contents of curricula across all other degrees, as well. Therefore, it is hard to generalize comparisons, which is why I will just be giving a general overview of which high impact cause areas can be relevant with a medical background and how much transferable knowledge med school can offer for these.
Transferable Knowledge
There are many cause areas that are tightly related to 'medicine':
Medical Cause Areas
For EAs focusing on direct, tangible impact it offers global health which is arguably the biggest nearterm cause area next to animal welfare and includes neglected tropical diseases (e.g. malaria), infectious diseases (e.g. pandemic prevention, AIDS/HIV) , parasites (e.g. deworming), chronic pain and mental health, malnutrition, toxins and pollution (e.g. Vit A supplements, lead metal elimination).
For the long-termists it can offer most notably the space of pandemic prevention, bio-risk, GCBRs, bioweapons, bioterrorism, man-made pandemics, etc. which is currently considered one of the two highest priority cause areas next to AI safety.[2] Beyond that medicine is closely related and even fundamental to all research that deals with individual human functioning and human health, e.g.mind enhancement, research regarding human quality of life andwell-being,consciousness research, and so on.
Now, how much of the knowledge gained in med school vs alternative degrees will be relevant when working in high impact careers on high-impact cause areas?[3]
Irrelevant Knowledge
I think it is fair to say that a significant part of the knowledge taught in med school focuses on specific pathologies and their treatments, most of which can be discarded when starting a career around one of the above cause areas. No one working on pandemic prevention will need the specifics of diagnosing and treating some obscure skin disease. Of course, a lot of the specific knowledge of any degree will likely become irrelevant when specializing in a specific career; But there are a number of degrees that arguably do a better job in preparing you for direct cause area work, e.g. a computer science degree for AI safety work. So how well does medical school compare to these top degrees?
It again, depends on the curricula and the testing requirements of the specific med schools / university courses and on how much they force you to devote your time to studying things that you know will likely be irrelevant. I have made the personal experience that it doesn't have to be too large of an amount and that making this trade can be worth it, but this will strongly depend on the specifics.
Fundamental Knowledge
In contrast to specific knowledge of pathologies, the fundamental knowledge treated in med school of natural sciences, biological sciences but also sociology/psychology will likely be highly relevant for all of the above cause areas. Furthermore, it is possibly taught with better signal-to-noise ratio than in other degrees as med school has to focus on the parts of the knowledge relevant for translational (i.e. practical big-picture) applications in humans and medical systems. (again, with large variation)
Translational Problem Solving
I think that it is this translational component which can make med school a uniquely good preparation for some high impact careers, because in a way EA shares a common principle with medicine: The mere generation of descriptive knowledge and understanding of things is not enough and actually irrelevant per se, it is about the translation of this knowledge to practical applications that actually improve outcomes within a highly complex and multidimensional background.
Having in-depth understanding of the functioning of specific sub-systems of cellular energy metabolism is incredibly interesting, but the impact of this knowledge is largely based on the interplay of the biochemistry with pharmacology, physiology, social interactions and psychology all the way up to sociological and economic factors.
This kind of big-picture thinking and problem-solving is fundamental in medicine and in my experience often overlooked in other hyperspecialized degrees, despite being highly relevant for any impactful EA endeavor. Of course, the extent to which a particular med school aims to teach the art of this thinking, again, varies wildly from country to country and from uni to uni.
Time and Credentials
Completing medical school takes a long time, usually 6 years. A bachelor in Europe usually takes 3 years, a master usually takes another 1.5-3 years. This means that someone just doing a bachelor will be done three years ahead, someone doing bachelors and masters up to 2 years. However, many people graduate medical school with doctorate degrees such as MD, MD/PhD or Dr. med. - whereas a PhD usually takes another 3-5 years after Bachelor/Master studies in other career paths.
This means that a medical degree right after high school, without completing another undergraduate degree first (which is possible in many European countries) may be one of the fastest ways to complete a university degree and get a doctorate. (in some countries, medical school does not finish with a doctorate, though)
Degrees
Respective durations
total duration
BSc/BA +PhD
3 + 4 to 5 years
7 to 8 years
BSc/BA + MSc/MA + PhD
3 + 2 to 3 years + 4 to 5 years
9 to 11 years
Dr.med. or MD/PhD (German Track)
6 years
6 years
BSc/BA + MD (US track)
3 + 4 years
7 years
Furthermore, the time intensity of the degree will vary widely as well. Some medical schools routinely require students to study 60 hours per week and more (I bet there's extreme upper limits to that for some US med schools) while for other schools an average of 20-30hrs per week (plus some cramming before exams) will suffice.
In my experience, medical school can be a relatively 'cheap' way to get a doctorate - and in some careers will offer a notable amount of additional credential boost just by being considered 'a physician’ or even ‘a doctor’ such as e.g. in public or political work.
Network
A very simple model of the predictors of the degree to which the average person you will meet during university studies is interesting could be 1) prestige of the uni 2) size of the city and 3) the distance that people were willing to put between themselves and their hometown / percentage of expats. (with the three probably being strongly intercorrelated)
All three of these are largely independent of the specific choice of your degree if you are the type of person open to networking and meeting people outside of university classes, so I would say that the choice of the city/town that you will be studying in matters more than the degree itself.
Value Drift
In my experience, medical school can be quite a hive-mind with the overwhelming majority of students in your classes mostly talking about medicine and clinical practice both on campus and in their free-time. While I assume it is not uncommon in most degrees that people mostly talk about their degree and don’t care too much about more overarching topics (e.g. philosophy, geopolitics, latest developments in science and technology), I feel like that might be particularly pronounced in medicine for a variety of reasons.
Furthermore a medical degree will prepare you for clinical practice and so that is what is expected of you as a medical student. That is what most of your fellow students will be doing in summer internships, that is what you will be getting great offers for, that is what most of your fellow students will be doing after medical school. The path of least resistance is clearly to also just start clinical practice after graduation - and then keep doing it.
Furthermore, in my experience a big factor of why some people do not end up doing clinical work after med school is that they do not enjoy interaction with patients. However, if you do end up enjoying patient interaction and the emotional tangibility of the impact you have in the clinic, having to give that up for abstract high impact considerations can be hard.
It thus requires effort, will-power and energy to make the extra effort and not start / leave clinical practice after graduation. This can be an important argument against starting medical school as I believe value drifting into clinical practice is a serious risk for a med school EA wanting to maximize their impact.
Robustness of a med school degree's expected impact to implicit EA risks
'Standard EA advice'[4] for high school graduates (never go to med school, go do something more directly relevant for known x-risks) is currently based on a lot of assumptions:
we are right about the current setting of priorities and cause areas
we have not missed any further cause X
EA will continue being able to pay all people wishing to do so for work in niche and formerly neglected causes (which further assumes:)
EA will continue being able to raise funds faster than people
indefinitely have quasi-unlimited funding by a handful of software dev philantropists (which assumes:)
no major economic crises cancelling holdings of said philantropists
no major shift in public perception of EA and no EA PR crises
no major wars cancelling holdings of said philantropists
no major wars reshuffling geopolitical world order and threatening US dominance
no environmental crises (e.g. runaway climate change) reshuffling geopolitical world order
etc etc
etc etc
A large part of EA endeavours and a lot of EA standard advice are currently based on the current world order and EA track record of incredible success continuing and/or assumptions about AI timelines being correct, which poses some risk.
While I generally remain cautious while optimistic when eyeing the above, I would propose that a medical degree and the breadth it provides can make your positive impact more robust to these EA meta risks than many other EA-inspired uni trajectories. (you are more independent from e.g. EA orgs, EA funding, EA worldviews) This could be one of your most important considerations when choosing a degree focusing on impact, depending on how confident you are in some of these EA meta-assumptions.
Furthermore, the incredible job safety of a medical degree always offering a comfortable plan B can be a source of confidence when later engaging in high risk high reward career paths such as EA-aligned charity or biotech entrepreneurship.
Lastly, if you are confident that AGI will be coming for us within the next two to four decades, med school will not be high impact. (just like most other areas of study besides those related to AI safety)
So - Is going to medical school generally a high impact choice?
What I have been aiming to show is that it is not as clear-cut.
If medical school prepares you for a high impact career or not will largely depend on the country, city and specific university that you are doing it in: the extent to which course content is transferable to high impact careers, the workload, the extent to which you will be forced to study irrelevant knowledge (largely specific pathologies), the degree which you can be getting in the end, the opportunities for extracurricular activities, the networking opportunities. Furthermore,your assumptions about the world generally and about EA such as our AI timelines or funding security of the movement could also be highly relevant to the expected utility for high impact careers in some cases.
In my case, I was privileged to be able to choose which medical school’s offers I wanted to accept: There are some med schools that I personally would not have chosen with the goal of maximizing my impact for a variety of reasons. If I had not had this privilege (and if I had only had an offer for medical schools not among my favorites) I would likely not have decided to study medicine in Germany.
I also think that there are some universities internationally offering university degrees that are preferable to most medical schools, e.g. I would probably trade my course in Berlin for a Harvard undergrad given scholarship funding of the latter. But I think that a degree in medicine can be preferable to a lot of other top choices under the circumstances outlined above, e.g. I rejected King's College London's Biomedical Sciences program to study medicine at Charité Berlin.
Is EA community building in medical school high impact?
Let’s assume that the central driver of impact of EA community building in universities are high impact career changes. (e.g. a programmer doing AI safety instead of mobile gaming as a result of their EA uni group’s outreach)
An EA med school group convincing med students to switch to a high (expected value) impact career and not pursue clinical practice will therefore have a positive impact.
But, can we already consider community building achieving that ‘high impact’?
Why do I ask this question? Well, in a lot of cities medical schools are separate from the general universities - often being completely independent. E.g. in Berlin there is the ‘Charité Universitätsklinik’ which is a large hospital with an integrated medical school whose students are practically completely independent of the other three big universities (Humboldt-, Freie & Technische Universität Berlin). Charité has ~7000 medical students, ~660 of which graduate every year. This means that every year hundreds of graduates will have never heard of EA (and therefore be unlikely to consider high impact cause areas) if we do community building only at the general universities and not specific to separate med schools.
In other cities, however the medical school might not be separate from the main university and therefore it might arguably be lower impact to found an EA med school group than a general EA university group.
Well, is it?
To return to the questions, I think the case for the first question is pretty clear and largely independent of the debate if med school is an optimal choice when choosing a degree with a focus on impact.
Potential for impact generally
The knowledge, network, experience and credentials of a med school graduate allow work on a variety of high impact cause areas
Community building in med school will raise the number of graduates pursuing careers in high impact cause areas -> impact
Comparing leverage
Even - if we assume that leverage and time spent working after graduation of a med school graduate is lower than that of an alternative degree’s graduate - once they’ve finished med school the EV of them working on a high impact cause area is still very big, as cause area is the main factor of a career’s impact.[5]
Furthermore, arguably the leverage of an average med school graduate is higher than that of an average alternative degree’s graduate due to strong pre-selection by med schools, possibly raising average competence. Additionally, in my experience a good portion of students choose medical school based on a desire to have impact on people's lives and do good - which might make them more open to the idea of doing good effectively, possibly improving community building success rates.
Depending on how high a bar we set for cost-effectiveness and our beliefs about leverage after med school, community building in some med schools could certainly be considered high impact (i.e. among the most cost-effective of all possible community building projects in terms of impact per $ [6]).
Of course, the bottom-line impact of community building in a particular med school will again depend on the specifics of studying there, the expected leverage of its graduates and might thus significantly differ between med schools. I think that community building in the med schools with the best fit for later EA cause area work will be comparable in cost-effectiveness to other high impact community building across the world.
Furthermore, I even think that generally community building at all med schools could be relatively cost-effective when looking at EA’s current talent-constrictions and other groups that EA is currently funding[6]. (e.g. non-student population outreach - with arguably smaller likelihood of high impact career changes, less time left working and less leverage due to less time for increasing cause area related career capital)
Interesting Caveat
One interesting thing to note is the chance of having negative impact due to people not dropping out of medical school as a result of EA med school community building. Let’s assume that 1) medical school significantly diminishes people’s ability to do impactful work and 2) that a significant amount of med students would discover EA, subsequently drop out of med school and do a superior alternative degree thereby increasing their ability to have impact. If we assume this, community building at medical school might actually 3) keep some people in the medical degree that they would otherwise quit, diminishing their leverage and causing negative impact.
I do not think that this objection strongly affects the impact of a EA medical school group since I do not generally agree with 1 and do not think that 2 is a large factor.
Furthermore, I am not sure about 3, that EA medical school groups generally lower the amount of people questioning their degree: In my experience, people have thought about dropping out more rather than less as a result of EA medical school community building (and especially subsequent exposure to EAGx conferences)
I think it is high impact.
While the default career path after medical school is not ‘high impact’, a high impact career after med school is certainly possible. Furthermore medical school might plausibly pre-select for people valuing altruism and impact and also for some factors beneficial to direct work due to relative competitiveness and perceived .
This means that community building in medical school that results in high impact career changes can be high impact and arguably even higher impact than 'unspecific' EA community building at a general university not targeting specific degrees.[7] Furthermore, this leaves me quite optimistic about the impact of a movement such as High Impact Medicine and has been my key motivation back in April to launch High Impact Medicine Berlin, the first local chapter of HI-Med in Germany.
Conclusions
My core aim in this post has been primarily to disentangle three related but independent claims surrounding medical school:
Is becoming a doctor a high impact career path?
Is going to medical school generally a high impact choice?
Is EA community building in medical school high impact?
Furthermore, I have tried to focus on and provide a more nuanced answer to the latter two questions, which I think might be important for some people. To wrap up, here again are my core claims/conclusions and my level of confidence in them related to these points: [1]
Becoming a doctor and just doing clinical practice is generally not a high impact career path (95%)
Doing medical school ≠ becoming a doctor & doing clinical practice (99%)
Career change in medical school due to EA med school community building ≠ people still doing clinical practice but more effectively (99%)
Medical school generally can work as a foundation for a lot of (non-clinical) high impact careers (90%)
Cost/value of medical school (trading time against knowledge, experience, network, credentials) significantly varies among countries/med schools which is a deciding factor in if it can be a high impact choice (80%)
Med school can be a high impact choice under some circumstances for some EA students looking to maximize their impact (80%)
(I am not saying that medical school generally is the best or among the best choices for all students looking to maximize their impact. I think it depends on specific circumstances of the specific curriculum, city, world models etc.)
Impact of EAs after med school is more robust to EA meta risks (e.g. cause X existing, EA running out of funding,...) than when specializing earlier during university on cause areas (80%)
Community building in some medical schools can be a high impact/cost-effective use of EA money (80%)
is high impact in all medicals schools (65%)
can be high impact even under the assumption that medical school generally is not among the best university course choices for high impact careers (75%)
Please note that the following is largely based on experience from studying at Charité Berlin, which does not necessarily generalize to all med schools. (Charité might actually be a uniquely good fit for an EA approach to studying at med school; I try to account for this by refraining from generalizing and stating the importance of considering the specifics of the particular med school.)
The modal value advice a high school graduate will get when talking to people at an EAG / EAGx conference or highly engaged EAs in general (this may only be my own subjective experience) or when looking at 80k most important causes.
I am assuming that: expected impact of a career change = importance of target cause area x time working after graduating x leverage (involves career capital, knowledge, personal fit etc.) I am assuming that the first factor will range over many more orders of magnitude than the other two.
Disclaimer: I do not (explicitly) know how much a high impact career change for an average student is currently priced at within the most cost-effective uni outreach groups. I also do not know how leverage differences are accounted for by current community building cost-effectiveness models - e.g. the ‘value’ of an Ivy League graduate career change vs. a small town art student graduate career change. I trust current community building grant evaluators to identify high impact community building opportunities well enough to use current recipients of community building money as a suitable community building standard to measure against. Please correct me if I am wrong on this.
I do agree though, that ‘specific’ EA university community building that e.g. focuses on only public health or machine learning courses could be yet higher impact than med school (due to even stronger pre-selection for skills directly relevant to cause area work)


I agree with you that practising medicine is not very impactful, and that community building in medical schools in some countries (e.g. Australia/DE) is useful. However, I think you're way overoptimistic about the value of a medical degree. Since that's our disagreement, that'll be the focus of my comment. Most of it will be line-by-line reactions to your arguments, and then I sum up a bit, and comment on outreach at the end.
Line-by-line comments
Specialising into EA is very non-robust to new cause areas, because it is a severe narrowing that happens early. And how many more billions do EAs have to make before you stop worrying about it running out of funding?
I'm not sure it's a matter of personal opinion. Greg has convincingly argued the opposite.
A medical degree is about 1/4 as dense in fundamental science as a science degree, because it only makes up about half of the non-clinical years, which in turn make up only about half of the program.
Most of the EA roles need biomedical science, and there's much less of this in med than in a science degree, because the medical degree is busy teaching you how to be a doctor. What's not spent on clinical medicine is often spent on memorising things that are not very broadly relevant, like anatomy, pharmacology, maybe medical ethics, medical law. So I would say the signal-to-noise is much worse.
Basically every degree can arguably give you special translational skills that help you to be a good EA. Math, law, and philosophy degrees "teach you how to think". Med, engineering, and business "teach you how to solve problems". But what is actually relevant is usually science and computer science.
This is not the right comparison. A medical degree doesn't help you to do many of the things that a doctorate does.
It's not actually that useful in my experience, especially outside Australia/DE. People care a lot more about whether you can actually do the job.
But all things being equal, it's much better to build a network of people who study higher-impact topics.
It definitely doesn't rely on these assumptions. If we new that the most impactful causes would by currently unknown to us, I think they would be more likely to be far away from med, which is a relatively narrow field. Think of previous crucial considerations: AI risk, anthropics, simulation argument. Not things that are particularly amenable to approach by a medic!
It doesn't assume EA will be able to pay all. But EA will be able to fund most who are smart enough to be admitted to a medical degree in Australia or Germany. The contrary was reasonable to worry about a decade ago, but the funding base has grown and diversified so much since then that it's really not defensible anymore.
Even if we gather a lot more people, we could allocate them to do things like policy that are funding-neutral and very useful, before we allocated people toward med.
The crisis would have to reduce the holdings of half a dozen billionaires by 95% all at once. And even then, there's things like Founders Pledge, GWWC pledge, and finance people, that also collectively hold billions of dollars of wealth. Not plausible.
No, once again, medicine is a very narrow degree.
In my experience, all that was useful was to earn a year's runway, and funds or . I spent about two years doing that. Then, I had to leave Australia to study. I maintained my medical registration for another year, by travelling back and practising briefly, but around that point it became clear that I was not going back to it. If I could have the time again, I would definitely have tried harder to apply for funds to drop out of my medical degree and study something useful. All up, this would have saved me about six years. Now that we are in an environment of such persistent and robust funding abundance, there is really no excuse!
Summing up on Medical Degrees
First, let's look at your summary, then I'll give mine.
I would say the main advantages of medicine are that you'll meet some smart students (some network), and a steady income stream. But it's far worse than the best courses. It's a narrow course, with less than average transferable knowledge. So it provides you with less optionality than, for example, a science degree. The workload is among the highest, so you will have fewer opportunities for EA-related pursuits. The content usually has less elective material than other courses, so you will be forced to study more irrelevant material. Your network will be suffering from these problems too, so they will be somewhat less likely to pursue high-impact roles than the smartest kids from a science degree.
For folks who are already in a medical degree and are very into longtermist EA, I think it depends to a fair degree how suited you are to working on biosecurity. If you are, then you might want to finish the degree. If you're not, you might not - you should check that you're not going to run into visa-related problems, but instead you could pursue a direct-work role, a startup project, or a masters degree. Other caveats include that you often need an undergraduate degree to enter a masters program, and to get a visa for some countries, so this is worth checking into, and existing with a BMedSci is often desirable, if possible.
Thoughts on Medical Student Outreach
I think outreach to medical students is not a bad idea. If you're going to allocate 3% of EA's outreach efforts to Harvard, then you probably should allocate at least 0.1% of efforts to medical students in Germany and Australia, or something. The point is that in these countries, there is a nationwide school-leaving grade, and the most competetive courses tend to be medical degrees, so they attract a lot of top talent - the sort of people who would go to Harvard or Oxford if they were born in those respective coutnries. Naturally, many of these folks will be interested in EA ideas, and could benefit from being connected to them. And biorisk is something they can help with (although by my reckoning it seems >30x less important than AI risk), along with perhaps other brain-related topics. But it's tricky, because you're naturally pitching these students on something that goes quite against-the-grain for their cohort - leaving their degree, leaving their field, and so on. Much moreso than what we ask of computer scientists, for example. But still, it seems worth a shot.
Hi Ryan, thank you for your comment!
Great to hear that you agree with most of the post (two out of its three main points), let me focus on the disagreements regarding the impact potential of choosing to go to med school:
As far as I can see, you raise three general points of disagreement. (do let me know if you don't feel like I represented your points well)
Regarding 1) Disagreements based on personal experiences with studying medicine in Australia:
I think some of the negative aspects you describe about med school are very important but might not be general to all medical degrees. I'll give some personal examples just to show that I disagree that your descriptions are generally accurate, of course you might actually be right in the majority of cases.. I do not have a good intuition if the median medical school internationally is more similar to the one that you describe or to the counterexamples I offer!
You write of highest workloads, few electives, all for a medical degree with no doctorate. (and that networking opportunities suffer from all that) I see how all of this is generally sub-optimal for high impact career paths, such as the research career in AI safety that you're currently pursuing.
Credentials
In Germany, as an option additional to the medical degree ('Staatsexamen') , most medical schools offer a Dr. med. (MD) degree track and some offer an advanced MD/PhD track (e.g. here). Both of these are considered a doctorate and are a very good foundation on which to build a career in research/academia or to go into industry. (given sufficiently good grades on either, with the MD/PhD generally being more valuable)
Electives and workload
15% of my modules are wholly elective, two further semesters offer longitudinal electives. I am sure that a lot of degrees offer way more, but I consider general workload being reasonable to be even more important.
Because, in my experience the workload is actually not that high in some medical schools, such as mine. A lot of my friends/acquaintances studying fundamental/applied sciences degree at elite universities such as Oxford or ETH Zurich have much higher workload. This means that the majority of my time is 'elective' in that I currently have enough of it to use it for 1) being main organizer and founder at my uni, 2) a research assistant job at a lab and for 3) things such as writing this post (and I am currently actually in the most time-intensive year). I know that this would not possible to this extent in all other courses that I could be doing.
2) value/transferability of knowledge taught in med school
It is hard to say how much of the disagreement here arises from uni to uni differences in course structure and how much is more about theories of value of knowledge.
First, regarding uni to uni differences: Of the 40 modules during my 5 theoretical years, only 9 focus on specific pathologies (and related pharmacology, etc.). A lot of the rest does contain knowledge on pathologies, pharmacology, etc. but always embedded in a general, translational framework which furthers understanding of the human. It might be that this is more focus on transferable knowledge than in the median course.
Re theories of value of knowledge: Since you focus mostly on transferable knowledge for research: From the experience that I gathered so far, academic research requires deep specialization in very specific methods researching very thin slices of reality, all of which with a depth that goes far beyond any course curriculum. This means that learning and special knowledge beyond uni material will always be necessary for academic research. While fundamental science degrees may arguably make this easier (especially the more fundamental the research is), knowledge from a medical degree will rarely make this further work impossible! It would be interesting to know how much harder you'll have it with a medical degree and thus how big this cost is but right now I am not convinced it is big enough to make me update! (The fact that you did manage to specialize in AI safety at FHI, Oxford with a medical degree is a nice anecdote in this regard that I couldn't help noticing)
Furthermore, over here there is the option of specializing into research and starting your doctorate as early as 2-3 years into the course, which could arguably make your specialized knowledge & fit for a specific research direction by the end of med school much better than that of someone with a general fundamental science degree. This is again of course something that will vary from uni to uni.
Lastly, when it comes to potential high impact career paths outside of research such as policy, entrepreneurship, (industry?) I suspect that we have a similar general picture:
Some more specific degrees could have arguably been an even better fit in terms of knowledge, but some aspects could yet again be in favor of the medical degree: e.g. translational understanding and firsthand experience of health systems on all levels, trained social skills, credentials of being a doctor (which is might be more of a thing in fields outside academia), job/income security allowing for time for other things etc.
And of course, the last point about income/job security is dependent on:
3), Disagreements regarding the relevance of EA meta risks (funding dependencies, cause X, etc.) and whether a medical degree actually makes you resilient against these:
Funding
You might be right that there's nothing to worry about in being dependent on EA funding due to historic successes in getting funds and the funding diversity you speak of. However, my own prior is generally quite low when it comes to placing trust in getting funds without problems, even when being 'smart enough to be admitted to a medical degree'. I've got some more to say about this topic but I to some more research/thinking on this specific aspect and then write another post discussing it in a more general context!
Cause X / Resilience
I think you might have changed my mind on this point while I was writing this reply. Here are my thoughts:
Regarding the question of how well a medical degree prepares you for cause X:
I agree that we can not assume that a medical school graduate is magically better suited for cause x, however I personally believe that EA right now is too focused on narrow quantifiable causes (due to inherent uncertainty of anything that's broader) and focused too little on general resilience-building. (Here are my rough thoughts regarding this)
I was going to say here that while potential future high impact resilience building efforts don't necessarily have to relate to medical fields, a broad degree such as medicine will be more likely to be valuable for them than a narrower one such as a specific fundamental sciences degree.
However I think you raised a good point in that some fundamental science degrees such as e.g. physics or biology are actually broader than medicine in important ways and might thus arguably be more valuable/applicable to future high impact resilience building efforts. (at least in my current abstract understanding of the term)
This is something that I would like to think more about and that I will reserve my judgement on for now!
I hope I could give some more perspective as to why we disagree on some points, overall you did cause me to update regarding my views on a medical degree resilience, potentially causing me to update on the value of spending time to apply for unis abroad after all! Let's see! ;)
PS:
I agree, I updated the wording on this
Just to rebut a few points there.
On (1) credentials/electives/workload:
Regarding (2) transferability: I believe you're overthinking it. From a zoomed out view, medical classes are approximately useless, and this talk of a specialised class becoming useful by being "embedded in a translational framework" is basically waffle.
You understate the case for the usefulness of useful subjects. If I'd studied computer science for undergrad, I could've got where I am now 5+ years earlier. Even dropping out of medical school could have accelerated things. In such a scenario, I could've been a somewhat more credible applicant for things like top professor positions than is currently the case. (Of course, skill is the main thing, but getting promptly educated, and building a stellar CV at a young age does help, vs studying irrelevant subjects).
Regarding (3) funding
What kind of evidence would make you update your prior? Many funders say they are willing to fund any person doing excellent longtermist work, and many orgs are continually growing and hiring. To take one extreme example, $50k fellowships are being given out to interested teenagers. It's a movement that's >10 years old, with its funding-base growing double-digits per year. If you're smart enough to get into a German medical degree, and dedicated, then it should be possible to do excellent work...
It being a small fraction doesn't make it less viable for an EA approach to studying med school. Every EA approach to uni will incorporate some tight admission rate.. It might not be relevant for AI safety but it will be super relevant for e. g. neartermist EAs or EAs that don't rank AI risk as high and want to focus on biorisk.
We do not have 'medical classes'. We have classes on systems of the body: foundational classes (biochemistry, molecular biology, physics, physiology) and classes that incorporate practical info, where you would argue they're approximately useless such as pharmacology. I disagree that they are entirely useless as it teaches you on a daily basis how the fancy science translates to practice, a skill that I will continue to argue is highly important (and at the core of any problem solving inside and beyond academia) and a skill that a pure fundamental science degree is 'approximately useless' for.
Fair points, as I said, I reserve my judgements here for now..