Hello everyone,
I was first ‘sucked in’ to this forum when I was directed to a post I might find interesting – it was about a research organisation with EA endorsement that was straying into my area of work, mental health. I’m a UK doctor specialising in psychiatry, with some research experience. To be honest, I was baffled and a little frustrated by how far this organisation strayed from what I would expect from mental health research – hence the (perhaps overly) technical diatribe I launched into on a website I hadn’t visited before, about an organisation I hadn’t heard of prior.
However, that’s not usually my style, and once I took a step back from my knee-jerk reaction, I wanted to understand how people with the same goals could arrive at completely different conclusions. It’s led me to do a lot of reading, and I wanted to see if I could try on a makeshift ‘EA’ hat, with most of my philosophy knowledge gained from The Good Place, no economics experience, and see where it went.
What I wanted to understand:
- Where has the interest in ‘wellbeing’ arisen from, and what does it mean?
- What are ‘subjective wellbeing’ (SWB) measures, and are they useful?
- Are we at a point of putting monetary value on SWB (e.g. like QALYs) for the sake of cost-effectiveness analysis (CEA)?
- When people are in this space talking about mental health, are we talking the same language?
- Why are RCTs the ‘best’ evidence for subjective wellbeing?
- What would I come up with from my perspective of working within mental health for a way of comparing different interventions based on their intended effects on wellbeing?
a. Spillover effects
b. Catastrophic multipliers
- How does my guess stack up against existing research into wellbeing?
- How could my framework be helpful in practice?
- What would I be suggesting as research areas for maximal gains in wellbeing from my biased perspective?
I’m aware this might be well-trodden ground in EA, which would make me embarrassingly late to the party, and consequently a complete bore. To lay my cards firmly on the table, I did approach these questions from the perspective that mental health is desperately underfunded, I spend a lot of time with patients who are severely affected by mental illness and therefore I’m biased towards seeing ‘wellbeing’ as an opportunity to rebalance this scale and acknowledge the impact mental illnesses have on people. I also feel the term ‘mental health’ is used in a way which is often confusing and occasionally unhelpful or stigmatising.
This is not meant as an attempt to further an argument against any person or organisation; it will also not be high in tech-speak as this was the first lesson I learnt very quickly on my journey – while jargon is a useful shorthand for talking with people in the same field, as an outsider it is exhausting. This post does not reflect the attitudes or opinions of anyone but me – this is my personal quest for common ground and understanding, not a representation of ‘UK psychiatry’ – I’m speaking in an entirely personal capacity and, accordingly, I’m assuming I’ve gotten a lot of it completely wrong.
To make this less self-indulgent, I’ve arranged this post to follow that question-and-answer format. For the sake of transparency, this was how this work came to be: I started with a long piece of writing about my concerns with assumptions made about mental health interventions in low- or middle-income country (LMIC) settings. I then did a quick Google on the WELLBY and wrote a lot about the idea of asking people to rate their ‘satisfaction with life’ on a scale from 0-10 which was essentially just entirely critical. I subsequently wrote out my concept of wellbeing as a framework, and my recommendations for high-gain areas for wellbeing-directed funding. Then I realised this was arrogant and so spent a couple of days doing a non-scientific review of the current subjective wellbeing literature. After several further drafts, this behemoth was born.
For readability/skipability: I’ve cut out some of my tangents, left others in for comment (#4, #5), and this piece will go through my arguments for an evaluative framework as a way of collating/synthesising (subjective) wellbeing research until we have more robust data (#6, #8). It will also cover my quick literature review (#7). [To be clear, this is not a scientific method which should be given any weight – I was bored over a weekend and so this was the best I could do, it’s not my day job!]
I am completely open to other opinions and comments. It’s almost certain that I’ve missed some key information from my speed-run through EA and wellbeing research so it will not offend me to hear this is the case.
Where has the interest in ‘wellbeing’ arisen from, and what does it mean?
Wellbeing, as a construct, seems to refer to a state of thriving vs surviving (in a nutshell). From some of the psychology/philosophy papers I skimmed through, it seems there is relative agreement that it’s complex and people might judge their wellbeing in different ways:
- Evaluative wellbeing – how satisfied we are in life, how do we rate the quality of our lives
- Hedonistic wellbeing – do we have more ‘positive’ feelings in life rather than ‘negative’ ones
- Eudemonic wellbeing – do we have a sense of purpose in life, can we derive meaning from life
While it might be relatively easy to gauge some (hedonistic) aspects of wellbeing e.g. how do people feel on a day-to-day basis in terms of their emotional/mental state, other questions are clearly more difficult to answer without some thought and maybe experiencing an existential crisis or two.
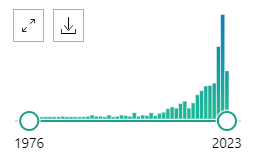
PubMed search results for papers including ‘subjective wellbeing’ in title or abstract/summary by date
From my quick literature review, the interest in wellbeing as a research area is a relatively recent phenomenon. There has been rapid growth in papers being published about subjective wellbeing from around 2020 onwards. I’d guess this is due to (1) the COVID-19 pandemic and lockdown restrictions making this a hugely important topic for public health officials and politicians, and (2) the recent interest in using wellbeing as an outcome when evaluating the effect of a broad range of policy decisions, which has subsequently driven interest in quantifying ‘wellbeing’ for use in cost-impact analyses.
Organisations like this one aim to bring wellbeing into the forefront of discussions for how governments, communities and organisations can improve people’s lives. Spending a little time on their website somewhat illustrates that this is not exactly straightforward: there are lots of factors which contribute to overall wellbeing, and a huge number of ways this information can be collected.
What are ‘subjective wellbeing’ (SWB) measures, and are they useful?
Subjective wellbeing measures are one way to capture the wellbeing impact from an intervention – you ask the people affected by the change to rate their wellbeing (using various tools) and you can compare these scores to those provided before the intervention to evaluate the overall gain or loss. This, however, opens debate into which questions are important to ask to get an idea about wellbeing – this complex concept with lots of theories and components. It also favours putting this information into a numerical form so you can compare scores before and after an intervention, which is much easier than trying to quantify impact from answers to questions like, “Do you feel your life has more meaning?”.
To capture information about national wellbeing in the UK, as part of growing interest in this area, a number of questions were added to national surveys (the ‘ONS4’). The four questions added:
- Overall, how satisfied are you with your life nowadays? 0=not at all satisfied, 10=completely satisfied (this question of Life Satisfaction sometimes crops up in research as ‘LS’)
- Overall, to what extent do you feel the things you do in your life are worthwhile? 0=not at all worthwhile, 10=completely worthwhile
- Overall, how happy did you feel yesterday? 0=not at all happy, 10=completely happy
- On a scale where 0 is ‘not at all anxious’ and 10 is ‘completely anxious’, overall, how anxious did you feel yesterday?
The last two questions can then be combined to give an idea of ‘affect (mood) balance’ – which I gather is important from some of the psychology research I read which argued that questions about affect shouldn’t reduce it down to unipolar constructs (e.g. happy vs sad) as this is not reflective of how people judge their overall wellbeing.
While a lot of interest has been devoted to using Life Satisfaction in UK policy as a singular measure of wellbeing for decision-making, I’m yet to be fully convinced of its value (more on this later). However, my personal thoughts aside, I’m not alone in thinking this isn’t the best way of measuring wellbeing. My quick literature review, which returned 286 relevant papers, included 41 different scales to gather information on subjective wellbeing (SWB), with several other papers including bespoke questionnaires designed for particular studies, or interviews with people to gather non-numerical (qualitative) data. Many studies combined different tools to capture different aspects of subjective wellbeing i.e. some tools are designed to just gather information on hedonistic wellbeing, or evaluative wellbeing, etc.
To me, as well, there is an issue with using purely subjective data for wellbeing. Perhaps this is my psychiatry bias coming into play, but while we elicit subjective information from patients, either by directly asking them e.g. how they are feeling, or indirectly through assessment of their thoughts and views on themselves; this is balanced against our ‘objective’ (i.e. external) evaluation as clinicians. Mental illnesses wreak havoc on our ability to think and perceive reality; either through distorting our perception of the world around us and ourselves; making us perceive our internal experiences as happening outside in the real world (e.g. hallucinations or delusions); or making our thoughts race, become disjointed, or slowed down.
While it is important to not dismiss patients’ subjective views, it’s not always appropriate to take them out of context. As an example, a patient experiencing mania might feel subjectively on top of the world and destined for greatness (10/10 Life Satisfaction) – they are, however, incredibly sick, their family is likely distraught, and they are at serious risk of harm if they don’t receive treatment - even if this would correlate to a lowered Life Satisfaction rating. Similarly, for people who might struggle to understand questions asking for a complex/abstract evaluation, it seems unfair to use standardised questioning to get an idea of their wellbeing; it’s arguably even more important to be flexible to ensure the information you’re gathering is useful and reflective of their experiences.
All of this to say, I have a feeling that while SWB data are helpful in some contexts, it’s important to use the information thoughtfully. Perhaps the huge number of SWB measures is reflective of this being a field in its infancy, still finding its feet, and there might be a future standardised and validated scale we can use to compare different interventions based on their wellbeing improvements. However, it’s equally possible to me that the number of tools reflects the different aspects of wellbeing which are most important to different researchers, different communities, or different groups of people. The future of subjective wellbeing research might be development of further tools for specific settings or people, or increased use of interviews to generate qualitative data if researchers want more in-depth understanding of the people they want to help.
At the very least, I think it’s reasonable to say that at the moment, it would be unwise to compare different SWB measures when this doesn’t appear to be validated as offering useful information. With wellbeing having a wide scope, and SWB measures still a growing area of research, it might be comparing apples and oranges to compare different SWB outcomes for different interventions.
Are we at a point of putting monetary value on SWB (e.g. like QALYs) for the sake of cost-effectiveness analysis (CEA)?
For the purposes of policy decision-making, there is interest in converting wellbeing impacts to an equivalent monetary value so it’s possible to make a judgement on whether or not the intervention was worth the money, and allow for different interventions to be compared e.g. which intervention can provide the best return (in wellbeing) for the cost. This is an approach which is already used for other metrics e.g. the value of a Quality Adjusted Life Year (QALY).
The UK Treasury has been looking into whether SWB can be used in a similar way with the WELLBY. This discussion paper suggests an approach which values one WELLBY at around £13,000; the equivalent of a one-point change in Life Satisfaction per year, using the 0-10 scale. It also goes into some of the complexities in using Life Satisfaction in this manner, especially converting this 0-10 scale of ‘satisfaction in life’ to the 0-1 scale used in the QALY between death and living a year with no health problems. While you could argue the QALY is only capturing a few areas of wellbeing, and it’s useful to have a broader perspective when wanting to measure how a change has helped people, it seems a bit tricky as a concept when considering settings where people are dying in significant numbers from preventable/treatable illnesses. It’s worth keeping in mind that the countries considering using the WELLBY (UK and New Zealand) would not fit that category, and this was an interesting read about the intricacies of using life satisfaction in CEAs in LMICs in terms of how you calculate the cost of a WELLBY for countries with different average LS, life expectancy and income (GDP).
I haven’t seen many arguments about estimating WELLBYs to direct funding or to compare different interventions. In general, it seems that the argument for WELLBYs is to collect SWB data before and after implementing a change, and use this to inform arguments about cost-effectiveness in terms of wellbeing; which in itself then requires careful work to ‘covert’ the WELLBY to a monetary value based on the country you are working within. This is good for interventions which aren’t just health-based where the QALY is not really capturing what you’re trying to do. It seems collecting robust SWB data (especially as this is a new field) and using wellbeing as one way to communicate the impact of an intervention is the recommended approach, rather than trying to use a ‘cost per WELLBY’ metric to compare different interventions. I haven’t seen much data to argue this is appropriate, and haven’t found many papers reporting Life Satisfaction in a range of settings from similar-style interventions to be able to support doing this (yet).
While for policy decision-making this perhaps isn’t a big deal, it clearly is a problem for people within EA who are interested in wellbeing as a way of measuring the ‘most good’ that can be done across a range of challenges and settings.
When people are in this space talking about mental health, are we talking the same language?
This is just a quick note to avoid confusion – there are lots of discussions about ‘mental health’ which have nothing to do with ‘mental illness’ and it’s important to avoid conflating the two to avoid misunderstandings. I suppose, to me, it’s a bit like this: generally speaking, smoking is bad for your health, it would be considered health-promotion to encourage people to stop smoking and dissuade young people from picking up the habit, however I couldn’t argue that not smoking or stopping smoking prevents lung cancer, emphysema and heart disease. Smoking greatly elevates your risk of all three, but you can live a perfectly healthy life and be unlucky. Similarly, while there are lots of things I can argue are good or bad for one’s (mental) health, that is a completely separate conversation from what is an effective treatment for a mental illness.
Generally, these mental health-promotion interventions are based around considering health as holistic (mental, physical and cognitive i.e. healthy mind/healthy body/healthy brain) so exercise, eating well, etc are generally good. Others are around avoiding stress e.g. workplaces offering flexible hours, mindfulness sessions, etc. You can make arguments about how mindfulness and exercise might promote (mental) health and wellbeing, but you’d have to show these are effective treatments for e.g. depression to make any argument they help people with a mental illness. Similarly, giving people without a diagnosed mental illness evidence-based treatments for mental illness to help their wellbeing would be odd. It’s a bit like telling non-smokers with lung cancer to stop smoking to get better.
I can see why mental illnesses have been used in the discussions I’ve seen on SWB, not only due to confusing terminology which uses ‘mental health’ and ‘mental wellbeing’ somewhat interchangeably, but also based on how ‘hedonistic wellbeing’ (positive vs negative emotions) is measured and how this might be over-simplified i.e. suggesting treating depression promotes happiness, or treating anxiety disorders reduces anxiety. I’m strongly against this approach because, simply put, these are complex illnesses which are more than simple emotions. A few examples: PTSD is an anxiety disorder, but rarely manifests in constant worry (hypervigilance, intrusive thoughts, numbness, etc – yes); someone with agoraphobia able to remain at home will not be living in terror day-to-day but may be extremely disabled due to their illness; for a diagnosis of depression being ‘low in mood’ is not even a requirement, etc. I do think mental illnesses have a massive impact on wellbeing, but not solely due to their effect on affect/mood balance.
Why are RCTs the ‘best’ evidence for subjective wellbeing?
I think, for evaluative purposes, the concept of randomised-controlled trials (RCTs) being the ‘best’ evidence to answer a research question is flawed when considering the need for subjective wellbeing approaches. While, in the hierarchy of evidence, RCTs are better than other types of studies, it’s important to clarify what ‘best evidence’ means, rather than taking that at face value.
Let’s say I’m doing an RCT on how well psychoanalysis (intensive psychotherapy offered five times a week) improves depression in working-age adults. My interest is in proving psychoanalysis works in treating depression. I recruit 100 people with depression and offer 50 of them psychoanalysis, the other 50 I offer ‘sham’ psychoanalysis (a placebo). Because I need them to stay on the trial to complete the study, I might offer them incentives, be really nice to them, or I’ll work within a company that’s happy for me to monopolise their time. Because I want to make sure it’s the psychoanalysis that’s having an effect on depression, I might exclude people that might complicate the picture (e.g. I might not want people already having therapy, or people misusing substances, etc); for the safety of participants who have kindly volunteered, I might not include people really sick with depression as they need immediate care.
I’ll randomly assign people into treatment or control groups as this usually makes the groups roughly similar and allows me to compare them fairly e.g. I wouldn’t want the groups to be all men vs all women, etc. I’ll also want to make sure (ideally) nothing else happens over the trial period to change how depressed they are because I need to ensure any benefit is due to my intervention and not some other reason (e.g. I can’t have the company give a raise to a bunch of people in my treatment or control group).
I’ll collect lots of measures of depression at the end, and let’s say it’s worked, I make people 10x better. I can do a CEA on this to argue everyone in the UK should have this amazingly effective treatment. I’d have to allow for the fact we know people do better in a trial than in the real world (because I’ve tried to stop them dropping out and chosen my participants carefully). I’ll begrudgingly accept it’s likely to be half as effective, people only get 5x better. But, even then, it’s worth doing and I roll it out across the UK.
It’s a complete failure.
It’s not really that the treatment isn’t as effective, although I find that too. The problem is I’ve spent a bunch of money on training and providing accessible psychoanalysis but no one is attending. Because, obviously, most people cannot attend therapy that frequently with work commitments, or won’t pay a babysitter to allow them to come. Maybe they prefer the free once-weekly therapy available in the UK, even if it is a bit less effective than psychoanalysis. The therapists I’ve quickly trained to do this work are burning out, and suddenly people are getting worse because their therapist has dropped them. The people that are attending are not very depressed (likely because their illness and their lives are allowing them to come five times a week for therapy) and so my treatment effects become less impressive because there is only so much you can make someone with mild depression less depressed vs the gains in my RCT when people had moderate/severe depression.
In this example, the RCT is still good evidence for psychoanalysis being an effective treatment for depression (i.e. it shows the intervention works). The CEA similarly might have been well reasoned. People are just messy and, outside of a ridiculous example like this, it's hard to predict how the treatment works in the ‘real world’ (i.e. the application). While in a RCT we need to reduce the amount of ‘noise’ to be sure any effect is due to our intervention, if a treatment is highly impractical or unacceptable, it’s not just the effect will be less good, it might not be effective at all.
This is particularly relevant in settings where it’s harder to predict all the unintended consequences (positive or negative) of an intervention. If wellbeing is an argument for subjectivity (vs objectivity obtained from RCTs), you need as much noise as possible: it weights qualitative evidence and observational studies much more highly. You have to accept there is a huge amount that is unknown in thinking about adapting a trial to the real world of another country, and simply reducing the likely treatment effect by an arbitrary number is an unhelpful approach without this work.
In other words – collecting real-world feedback on the intervention from the people most affected by it is helpful to understand their perspective on the ‘most good’ which can be done in their community. How much subjective wellbeing should be understood alongside other metrics is veering into dangerous philosophical territory for me e.g. if an intervention improves mortality in a country, but it negatively affects everyone’s wellbeing, is it still doing good, or how much should that down-grade estimates of goodness? Alternatively, is it right at all for anyone else to say what ‘doing good’ is in another community? Perhaps ‘wellbeing’ allows for a more complex construct of ‘good’ which reflects the philosophy of those affected rather than risk imposing an external set of values.
There is the additional issue that RCTs are expensive to run and therefore present a barrier for researchers in LMIC settings to produce this 'best evidence', which seems like an issue when aiming to reduce assumptions in CEAs. To me, personally, there seems to be an under-recognition of the problems in relying on externally-funded RCTs to produce this evidence. Firstly, it almost inevitably involves applying assumptions to drastically different cultures – in terms of mental health, this is particularly problematic given how culturally-bound mental illnesses are in terms of experience, understanding and expressions of distress; as well as approaches to treatment. In some cultures, physical/spiritual symptoms are much more common than our more psychological formulations of difficulties; and psychotherapy is not always acceptable or even desirable as a treatment. Secondly, it appears to ignore the power dynamics at play when a wealthy ‘outsider’ pitches up in a remote community to conduct research.
As another detour from reality, let’s imagine I don’t live in London. I live in a tiny village and I’m hit by a devastating flood. I’m sleeping on a camp-bed in the local community centre – I’ve lost everything and I’m in a very dire situation. Suddenly, Elon Musk arrives in a helicopter and hands me a designer raincoat (worth £200). His assistant asks me a few weeks later if that was helpful and if I’m glad I have the raincoat. I would probably answer yes, because by then I’ve found some use for it, and I don’t want to upset the team handing out expensive raincoats. I might even say it’s the best thing ever because I’m hoping he’ll come back and offer me something else. However, if he had asked me initially if I wanted £200 or the raincoat, of course I would take the money – and I would find it slightly irritating if he then pulled a face and told me the weather forecast for next week to suggest I would be better off taking the raincoat.
To return to reality once more, I can see the argument for RCTs for mental health interventions in LMICs – it's worth seeing if treatments are similarly effective in these settings when the bulk of evidence is otherwise derived from non-LMICs. It might allow for some gauge of cultural acceptability if provided in a non-coercive manner and would also allow researchers to collect SWB data as one of the outcome measures to argue for cost-effectiveness. However, this is not the only way of gathering this information, and to define the ‘best’ evidence, this is not a simple matter of hierarchy.
What would I come up with from my perspective of working within mental health for a way of comparing different interventions based on their intended effects on wellbeing?
How satisfied are you with your life, on a scale from 0-10?
As I’m talking to some EA folks, my ‘prediction’ is there’s a mix of people who had a gut response to that question (including a complete reluctance to answer at all), those who puzzled over that initial response, those consumed with guilt for any instinctive rating deemed ‘too low’ given an acute awareness of others’ suffering, and those who suppressed any immediate response and set in motion a internal moral philosophy machine to answer the broader question of what is satisfaction, how do we self-evaluate? [Now I've spent some time on this forum - I give you 80% odds every EA reading fits at least one category, with the known variable giving a confidence estimate highly increases the chance of someone wanting to object to prove me wrong and now struggling with the trap I’ve laid which has created a scenario, regardless of outcome, where I’m 100% right… and down-valued my goodwill from EA with this joke by 0.85]
I suppose I’m trying to recreate real-world conditions for how people respond to that question with some mild impatience or irritation in the person asking i.e. as part of a survey, or lumped in other outcome measures in an RCT, or even being asked by a stranger. Perhaps a reliance on comparable, numerical metrics produces a certain absurdity. I’m trying to imagine having a conversation with someone I care about to ascertain their wellbeing, and following that up with “yeah, sure, but on a scale from 0-10?”. Or possibly, from my experience in medicine, the face a patient makes if they are rolling around, screaming in agony, and someone asks for a pain rating out of 10. We accept a range of responses to mean '10', but a pain scale is at least useful in other contexts.
My gut response to the same question about life satisfaction (“I don’t know, about 7/8?”) seems to put me in good company amongst survey respondents in the UK where average Life Satisfaction is 7.54, but does that mean we have comparable wellbeing? Is it just the British approach to any similar question ("How am I? Good, thanks."). I struggled to imagine what the difference between a 7 or 8 would be, and if I answered the same question next year with no changes in my wellbeing, it might therefore be +/- 1 based on a coin-flip. While I can remember a 10, I’m struggling to know how I’d keep at a 10 on repeated measures to determine wellbeing or whether that is even desirable to me i.e. if I took a pill that made me feel like that way constantly, what effect would that have on my life? Similarly, my growing devaluation of this question could easily provoke a ‘f**k you’ response if I was asked uncaffeinated. Apparently £2 spent in buying me a coffee before asking next year nets a good 5 points – I’m cheap at £0.40 a WELLBY. Obviously, responses are more valuable when taken across a sample or population… but are they? It seems taking averages loses meaning too.
It doesn’t really matter, as a full roll-out of Life Satisfaction scores for the purposes of WELLBYs is under consideration, so I’ll wait to see the value in the data collected to be proved wrong. However, my feeling is it’s unlikely to produce helpful information alone, and if I was going to guess what makes up ‘overall wellbeing’, I might use the qualitative nature of my interactions with patients (and qualitative research in general) to identify key concepts. For the sake of comparison to QALYs etc, I would probably agree it’s sensible to keep 0 at death, and use 1 as a year lived at ‘baseline/average wellbeing’. I suppose the same way that being in peak physical fitness is a ‘bonus’ for a QALY, living an enlightened high-wellbeing life is a bonus for my scale.
The key concepts
Health - Illness will reduce wellbeing from your normal baseline, both in terms of the acute illness and the years spent with this illness that prevents return to baseline
- Where the duration of untreated illness can affect prognosis, the immediate impact should be weighted much more severely than considered over the long-term e.g. duration of untreated psychosis is a negative prognostic factor in predicting recovery in schizophrenia - it is much more effective to reduce the duration of untreated psychosis (immediate) than treatment in the longer term to promote long-term wellbeing
- Some illnesses produce highly unpleasant symptoms that are likely to affect someone’s day-to-day enjoyment of life e.g. pain, fear, fatigue, etc. I don’t think it’s appropriate to relate this uniformly to severity e.g. through symptom measures. I would favour ‘daily symptom burden’, which will be affected by access to effective treatment – if treatments are broadly ineffective, or not available to people, it allows different weighting here.
- To explain my reasoning, anxiety disorders (mild/moderate/severe) appear exponential in Disability Adjusted Life Years (DALY) weighting – a measure of impairment. Someone with agoraphobia may be housebound (significant loss of function) due to extreme fear of the outside world, but provided they are able to avoid leaving home they will not be living in fear. In other anxiety disorders e.g. generalised anxiety disorder, it is not possible to escape the anxiety (and you can't use fast-acting anxiety-relief treatments to mitigate this), even if it doesn't meet the same level of terror someone with agoraphobia might face if forced to leave the house.
- Someone constantly experiencing 3/10 pain daily despite pain relief might rate their overall wellbeing worse than someone experiencing 8/10 pain once a week who can relieve this with their morphine prescription, despite being lower on the pain scale
- In short – Daily symptom burden = how bad are the symptoms, how prevalent are they, and can you get any relief from them?
- In looking at ‘ill health’ in general, it might be worth considering if certain illnesses have a compounding effect (i.e. if you get X illness, is this worse because you already had Y), or multi-morbidity in mitigation to ensure problems aren’t double-counted i.e. if two conditions result in loss of a person’s left arm, these shouldn’t be added together as you don’t have two left arms).
- Overall, for wellbeing, it’s understanding ‘poor health’ as (1) having a mental/physical illness (with the expected effects on life expectancy as my scale uses 0 as death), (2) unpleasant daily symptom burden.
Autonomy - The ability to maintain control and independence of one’s body/self and make choices in life which reflect one’s beliefs and values.
- The disability weight used in the DALY gives some idea of the ‘unpleasantness’ or undesirability of an illness/impairment which seems useful as a measure of the impact of a new diagnosis and it reflects broadly how people feel they will cope i.e. it should be a good measure of the short-term impact of an illness and how relatively feared/undesirable/distressing it is.
- However, the effect on wellbeing in the longer term has to allow for adaptation and deterioration, as well as recovery to baseline. Some conditions have a poor prognosis with further impairments and therefore a constant, subjective feeling of loss (e.g. progressive MS). Other people adapt to impairments with time and I feel it is wrong to imagine they cannot obtain high levels of wellbeing. Rather than saying someone with a disability will be X% worse off over the course of their lives as a static measure, it instead puts the onus on doing what we can to promote their access to the same opportunities. It would therefore weight the impact of a disability worse in resource-poor settings where people are not provided means to adapt.
- Ideally this would be informed through qualitative feedback from people with the illnesses in question in different settings to understand short-term vs long-term ‘impact’.
- Other examples I would imagine that drastically decrease autonomy might involve exposure to inescapable forms of violence and abuse (e.g. domestic violence, persecution), inability to exercise bodily autonomy (e.g. access to contraception)
- I suppose ‘lack of autonomy’ would include other aspects of being able to freely make decisions - this is seen in different ways e.g. people feeling trapped on benefits or trapped in jobs due to economic insecurity, being barred from education, or unable to afford/access healthcare. It is also a consideration for people requiring hospitalisation (particularly over the long term), institutionalisation, or incarceration.
Security - Confidence in having basic needs met (food, water, shelter, care).
- I would extend this to the benefit of having close confiding relationships if desired (an emotional/social sense of security).
- I would also imagine that childhood experiences of insecurity have ongoing effects in how people judge security throughout their lives, and leads to varying responses to real or perceived threats to that security – as an example, it’s thought that adverse childhood experiences are common in the aetiology of all mental illnesses, but it’s thought that neglect of a child’s physical/emotional needs (e.g. if parents are not able to respond appropriately due to mental illness, substance misuse, or exposure to violence) can lead to problems throughout adolescence and adulthood in personality difficulties and disorders.
Time-direction - Having the ability to spend time in ways people value or find meaningful.
- People are not just 'living to work' or so over-burdened with responsibility they cannot utilise time for themselves how they wish e.g. social activities, interests; and they have the freedom to make trade-offs to reflect their priorities.
- Similarly, people being able to feel connected to a cause or community greater than themselves is important for people to find a deeper meaning in life and have a sense of purpose and fulfilment.
Equality/justice - Belief we are in control of our destinies and society rewards efforts and skills fairly.
- I think, as social creatures, we judge ourselves and our position in life compared to others and are therefore sensitive to ‘unfairness’. I think this plays out repeatedly in multiple ways across society, and generally inequality will act to decrease wellbeing e.g. I imagine in communities with high economic inequality or prevalent discrimination/unequal opportunity, this will decrease life satisfaction.
- While I think the impact is greater in the disadvantaged group, it can also reduce wellbeing in the advantaged group, because by profiting from an unjust society, there can be concern one’s circumstances can be lost if not based on factors within your control or your achievements are not reflections of your abilities e.g. if I slept with my boss for a promotion, those around me will feel this was unfair (I didn’t get this opportunity/salary bump through hard work or aptitude at my job) and will likely lead to a strong decrease in job satisfaction amongst my colleagues (why bother trying when promotions are handed out like this?). On the other hand, while I’ve benefited from the promotion, I would question if I could have gotten it on my own merits, worry about my competency and be very sensitive to mistakes or criticism. I might worry I could lose my job if I get a new boss and it’s discovered I'm actually incompetent.
How this feeds into a 0-1 scale? I’d suggest a matrix approach is helpful – even if SWB data aren't available to argue for wellbeing as a whole (either because it doesn't exist yet, or uses tools other than the supposed 'common currency' of Life Satisfaction, or uses qualitative information), this will allow what is known from existing research to be incorporated in these judgements while avoiding trying to combine SWB measures together, and produce an overall value of 'wellbeing impact'. Taking the above, I feel this could accurately reflect the benefits to society from broader interventions other than health alongside health-focussed interventions.
For interest's sake, I tried thinking of mental illnesses along these lines. From most to least impact on wellbeing, I'd probably put it in this order (non-exhaustive list):
Schizophrenia/Schizoaffective disorder (with further higher rating in first episode psychosis) > Bipolar disorder type 1/Severe depression with psychosis > Severe personality disorder/Severe depression > OCD/PTSD/Eating disorders > Moderate to severe generalised anxiety disorder/Moderate depression/Bipolar type 2/Agoraphobia/Social Phobia > Mild depression/Mild to moderate generalised anxiety
The DALY disability weighting (limited list/different language):
Acute schizophrenia > Severe depressive disorder > Residual schizophrenia > Severe anxiety disorder > Bipolar disorder (manic episode) i.e. type 1 > Moderate depression > Anorexia/Bulimia > Mild depression > Moderate anxiety > Residual bipolar disorder > Mild anxiety
So, it doesn’t seem to be just arriving at the same answer in a more complicated way. However, there are a couple more things I would add if understanding the effects of (mental) illness on wellbeing.
Spillover effects
I’ve seen the term ‘emotional contagion’ used now and then when talking about household spillover i.e. how are other members of the household impacted by an illness, or benefit from this person receiving an intervention. I think it’s more helpful to take a systems-approach to understand the ‘spillover’ effects on wellbeing, which could similarly be modelled on the same framework. It reflects, then, the role that someone fulfils in their household and therefore the impact on the household if they become ill i.e. are they the main breadwinner, do they have caring responsibilities, do they have dependent children, is there a social ‘safety net’ if they are unable to work or fulfil their usual duties in the home. Is someone else having to pick up extra hours to pay rent, or reduce their hours to stay home and provide care, can they no longer enjoy life or engage in activities because their role in the home has changed?
Again, based on my brief comment above, we have to weight heavily impacts on children, particularly in their early years, where adversity will have enduring effects on their wellbeing throughout their lives.
A catastrophic effect multiplier – despair
While slightly cautious of mentioning this topic in a broader discussion of mental health [this bit will be talking about suicide and physician-assisted suicide, as well as electing not to pursue life-prolonging treatments], I think it is important in discussions of subjective wellbeing. While it’s difficult to imagine what types of people have maximal wellbeing, with 0 being ‘death’ on my proposed wellbeing scale, it seems there are many people who do judge their lives as equivocal or worse than death when contemplating or attempting/completing suicide. I don’t think that should then produce negative ratings below zero on my proposed 0-1 scale, but if an illness or societal adversity predictably increases rates of suicide, the overall effect on wellbeing considered in these situations should have a catastrophic multiplier applied to reflect this causes a number of people to make negative evaluations (i.e. to bring the wellbeing measure closer to 0).
I think this is more helpful than including suicide in estimates of premature mortality of various illnesses, where otherwise ‘mental illness’ is rarely questioned as an attributing factor compared to others, or ‘untreated/undiagnosed’ mental illness is speculated upon when no diagnosis exists (either colloquially or through these data being sought in the first place). I think it is harmful to perpetuate either this understanding of suicide, or mental illness. Aside from all the research demonstrating suicide is not predictable in anyone, or preventable by improving access to mental health services/treatments (aside from lithium, interestingly, this does appear to prevent suicide, seemingly on an ecological scale). It also seems to fail on face validity alone in countries that permit euthanasia, where psychiatric illnesses impacting judgement are screened for in referrals. If wishing to end your life was uniformly symptomatic of a mental health problem, and assuming this is not eugenics in action, there would be no demand or uptake of these services.
Instead, I think suicide is best understood through the concept of current subjective wellbeing + prediction of future subjective wellbeing x belief we can change our future (i.e. current SWB + hope vs despair). My interpretation of wellbeing already incorporates viewing not only one’s current state but a view of one’s future (i.e. health, autonomy, equality), but it’s important to recognise that these concepts should be defined separately here for the purposes of applying 'despair' as a multiplier. If someone’s current wellbeing is critically low, they view their future as continued/worsening suffering and have the belief this cannot be changed, this appears to correlate to how people make decisions to end their lives. Conversely, it might allow some understanding for how people persevere even in incredible adversity – they maintain hope things can improve and that this can be brought about by their actions, or perhaps are more resilient to factors compromising wellbeing or naturally optimistic in predicting/valuing the positive impact of future events.
Despair therefore can be an effect multiplier in known conditions which increase risk of suicide, as well as conditions that could plausibly result in critically low wellbeing, negative evaluations of the future, or lack of control over the future, when this information is not clear. E.g. in thinking about health, these evaluations could arise from illnesses that produce a large negative impact on wellbeing and/or have a deteriorating prognosis which leads to a particularly grim view of the future; for which there is no treatment, palliation or support to induce any hope things can improve.
I prefer this as a catastrophising modifier on the effect of illnesses/societal adversity rather than incorporating it into the framework as another concept because I don’t believe it arises independently, and I think it is harmful to categorise people seeking physician-assisted suicide or not agreeing to life-prolonging treatments as ‘lacking wellbeing’. To do so would go against my view on death and dying. Thinking about someone approaching the natural end of their life: there is nothing that can be done to change this, and predictions of the future become increasingly certain. It would be deeply wrong to characterise this as ‘despair’ or suggest people with life-limiting illnesses therefore cannot rate their lives with high satisfaction or experience high wellbeing. I’d argue that when the otherwise prospective approach to self-evaluations of wellbeing is no longer appropriate, this reverses to a retrospective view, where we evaluate our satisfaction based more on our current subjective wellbeing and take on an increasingly retrospective view on what we have done, our impact on the world, and take comfort in what we are leaving behind.
How does my guess stack up against existing research into wellbeing?
I searched PubMed for original studies looking at predictors of subjective wellbeing. I searched for “Subjective” + “Wellbeing” which yielded 699 results. I did an abstract-only review (i.e. looked only at the summaries of papers written by the authors) for studies which looked at a variable/factor and how this related to SWB. I couldn’t include papers which used SWB to explain a relationship between two other variables, or those which produced conflicting results on different SWB measures for the purposes of what I was doing. This left me with 286 relevant abstracts in total.
I picked out information on the country the research originated from, the SWB scores used, the factor the study looked at and if there were any important moderating/mediating factors the researchers found e.g. while variable X was associated with low wellbeing, we found lots of this effect could be accounted for by variable Y. I didn’t pull out information about the size of the study or the effect size as this was an abstract-only review, and I can’t make comments about how robust any of these studies were. [Again, this is why ‘abstract-only reviews’ are not a useful research tool, but it seemed like the least biased way of collecting information, and I only had a weekend.]
General findings
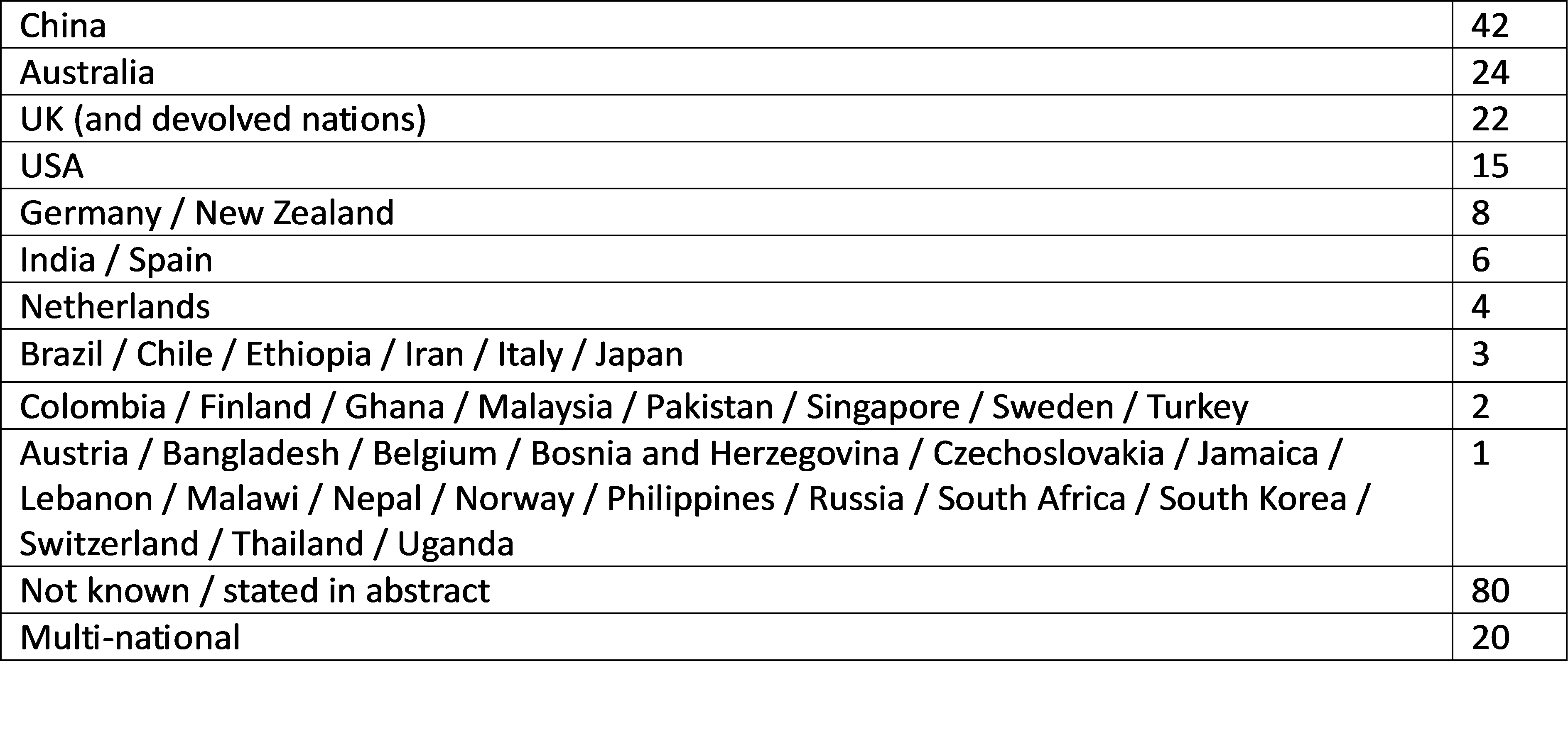
Firstly, I mentioned earlier on that this is a recent area of research interest. It’s important to also mention that, therefore, it’s influenced by early-adopters of this work i.e. the countries that developed an interest in SWB measures and so produced a lot of research from the get-go are over-represented in the available research. As wellbeing is highly subjective and context-dependent, this should be kept in mind when understanding the direction of research and how we draw conclusions from what's currently available. Where the country information was available in the title or abstract, here is the number of studies by country:
For anyone who prefers a visual representation of the research share for single-nation studies:
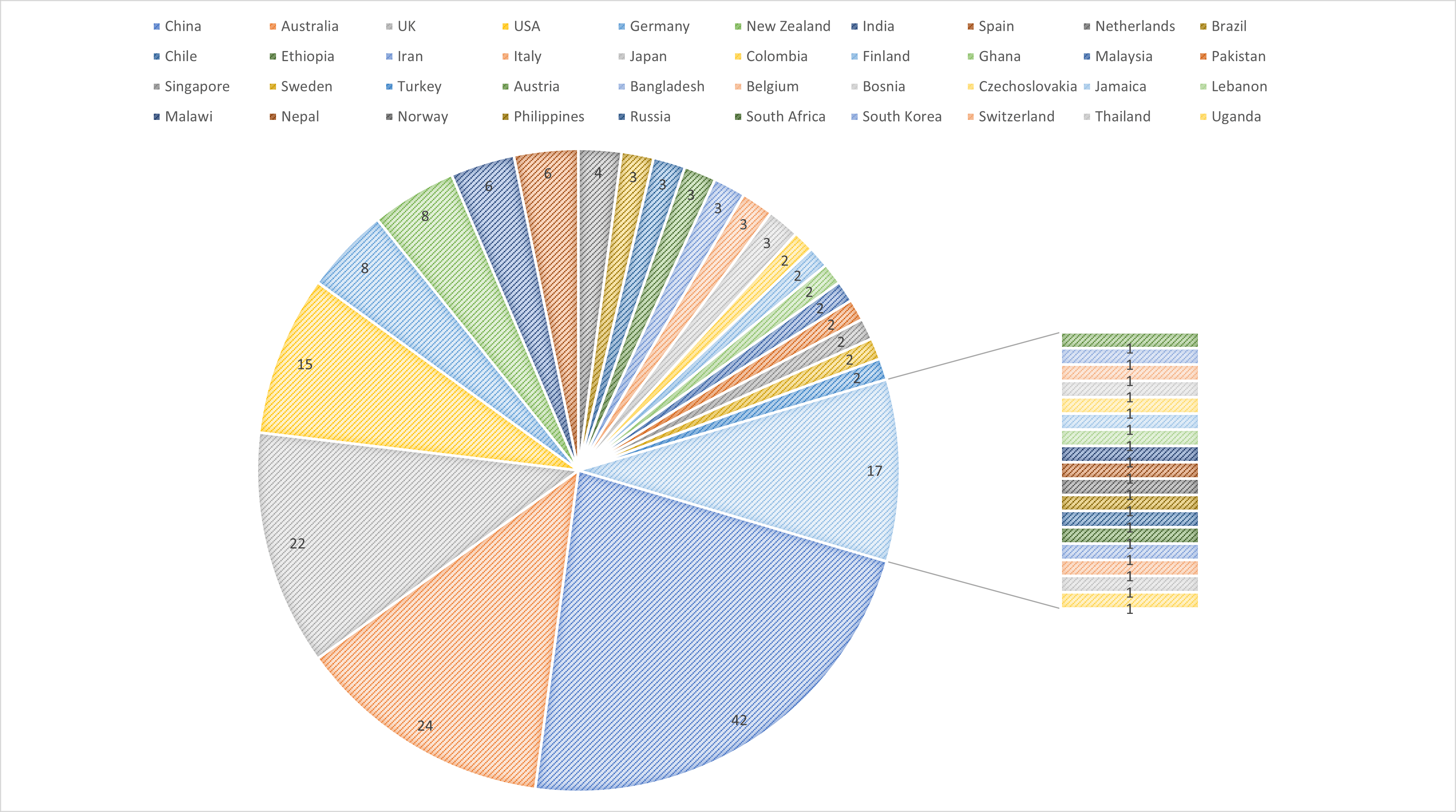
As well as this being one of the prettiest pie charts I’ve ever made, it demonstrates a few countries hold a lot of wellbeing research territory at present.
In case anyone skipped me talking about this in an earlier section, in these 286 studies, I found 41 different SWB scales being used, and a number of studies using bespoke questionnaires or interviews collecting non-numerical (qualitative) data to describe subjective wellbeing. Lots of studies used more than one SWB measure.
It’s worth mentioning that many of these studies were focussed on very specific groups e.g. rural-to-urban older adult migrants, or specific ages e.g. adolescents, or specific circumstances e.g. mothers of children <18y with autism spectrum disorder. How useful any of this information is taken out of that context is debatable, but I found it interesting to see what the researchers thought might be related to wellbeing, to judge my finger-in-the-air style guesswork that otherwise is based on a ‘trust me, bro’ of my clinical experience.
What also became clear to me from wading through these abstracts, is that it’s difficult to really tease out a ‘causal’ relationship i.e. to say XYZ results in better or worse wellbeing. To give an example, there were a fair few studies which found that physical activity was related to greater SWB. Does this mean exercise improves wellbeing? It might also mean that people who have good wellbeing are more likely to engage in exercise. If it was just about activity, should we expect manual labourers, service industry workers, cleaners, etc to therefore have higher wellbeing as they have active jobs? Or, is it that people who regularly exercise have a higher income/socio-economic status, or just aren’t sick and therefore able to exercise – and perhaps it’s just that wealthy people with no health problems are likely to have high wellbeing, whilst also engaging in regular exercise.
In simple terms, lots of variables can coincidentally relate to higher SWB, some might interact with other variables (i.e. have a greater impact on wellbeing as a system vs the sum of their parts), and some are likely unhelpful taken out of context with other issues we know impact wellbeing.
The non-scientific literature review
I took my proposed framework and saw what studies were out there to validate it. Some concepts I think could be debated into where they fit in the matrix – it’s my best approximation but, as an example, ‘low SES’ spans multiple domains in terms of autonomy, security, time-allocation and equality.
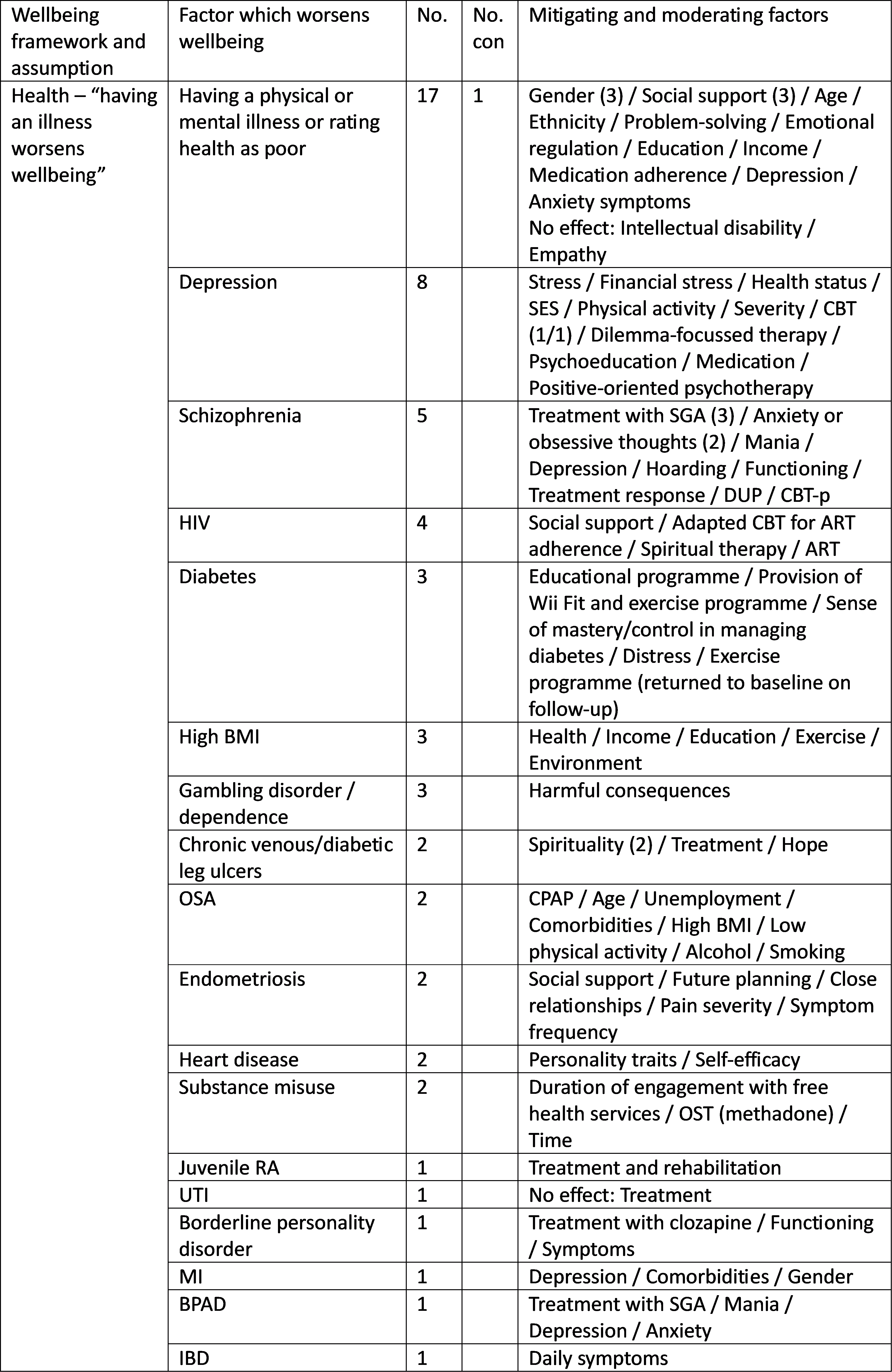
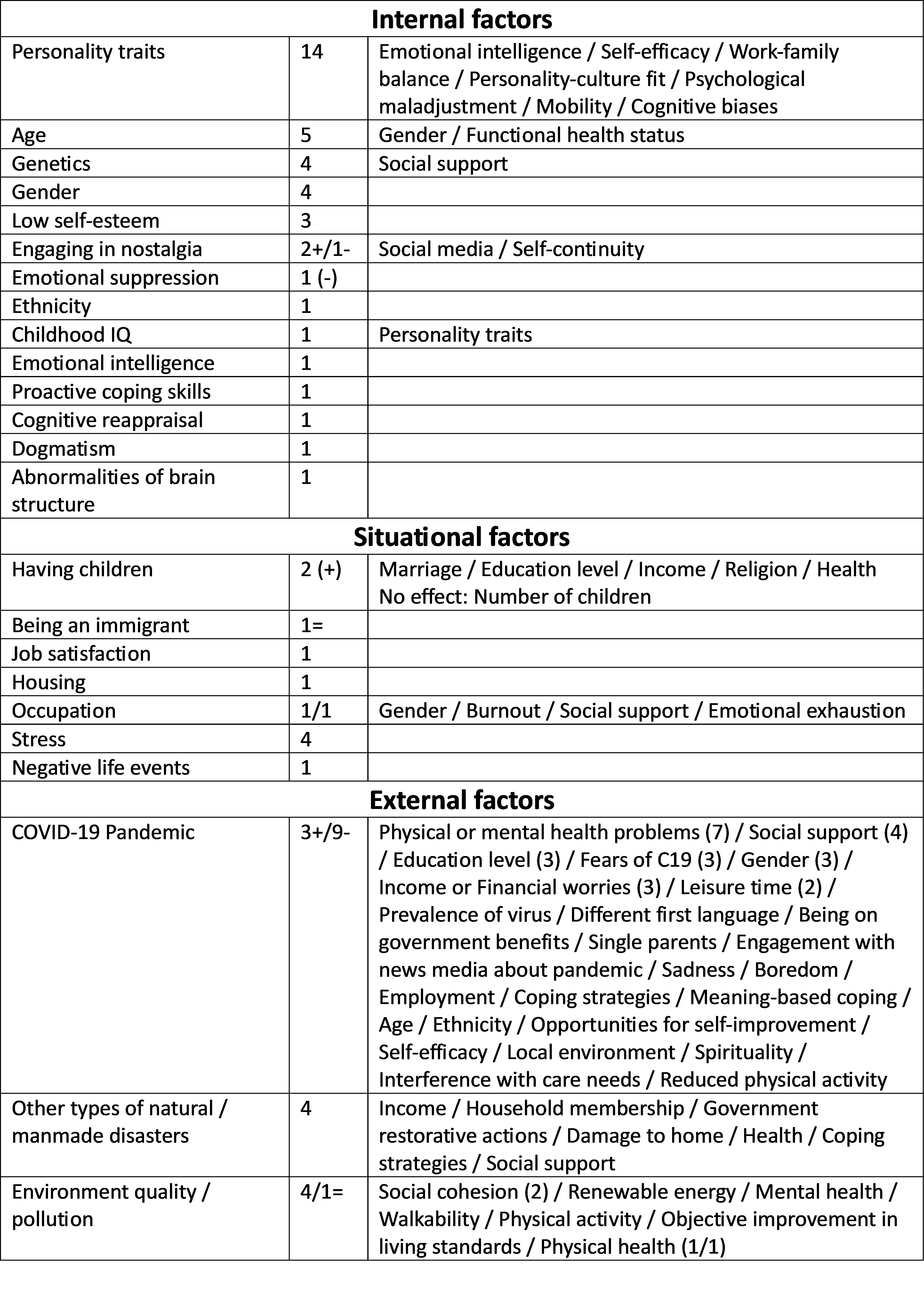
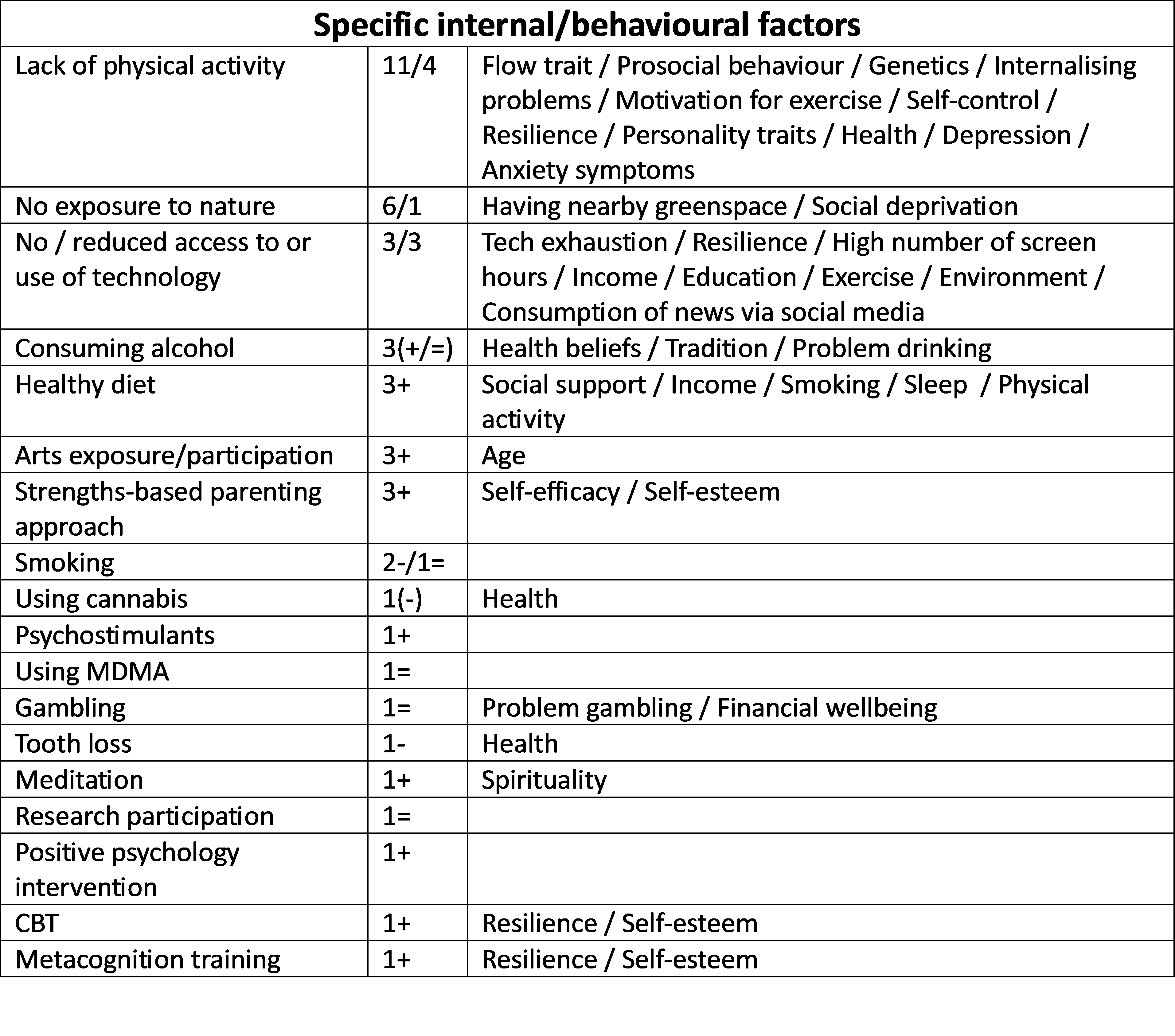
Here is a summary of the 286 studies, with the number of studies which identify the same factor as worsening wellbeing (No.), the number of studies showing conflicting results/no effect (No. con) and any mitigating/moderating factors.
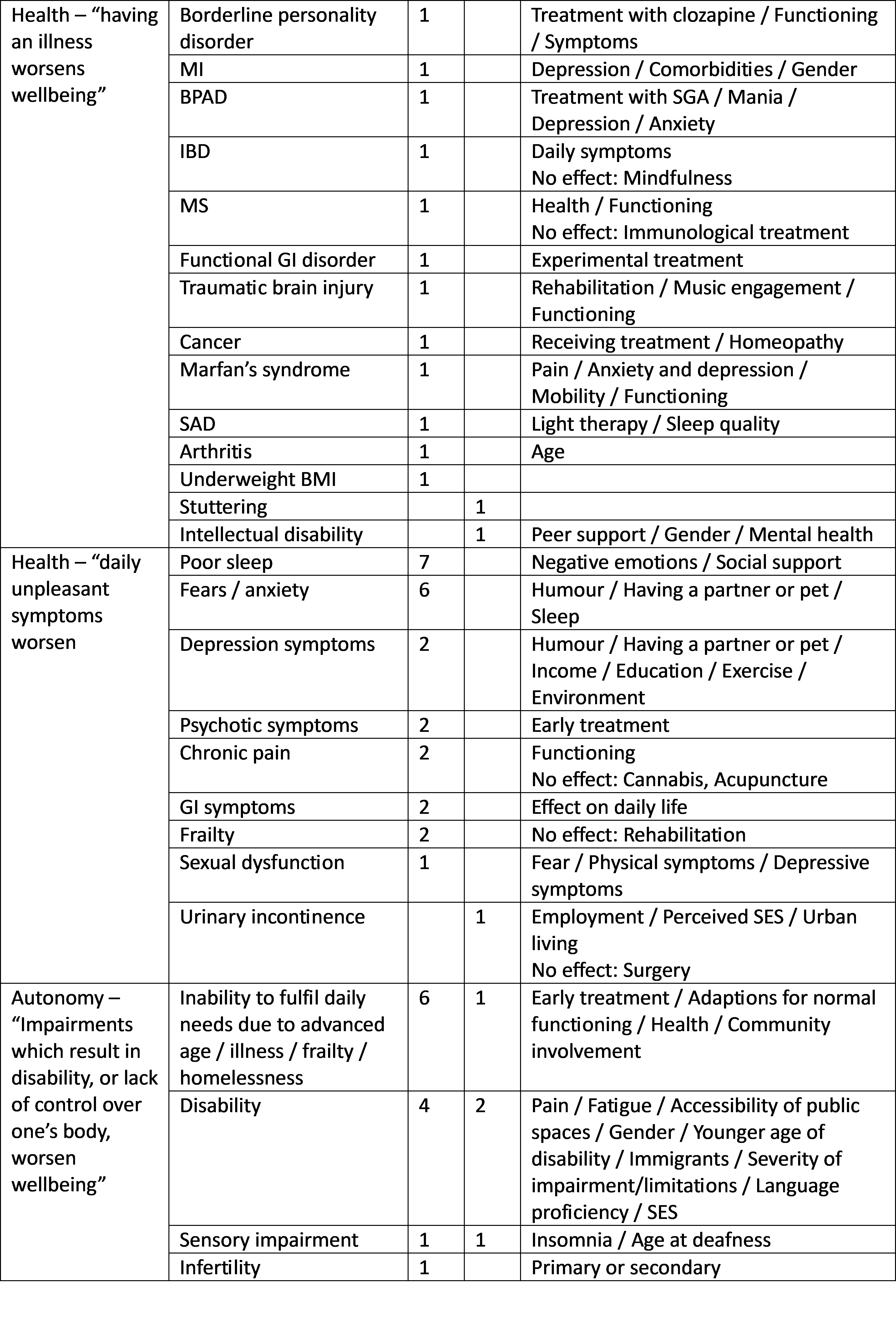
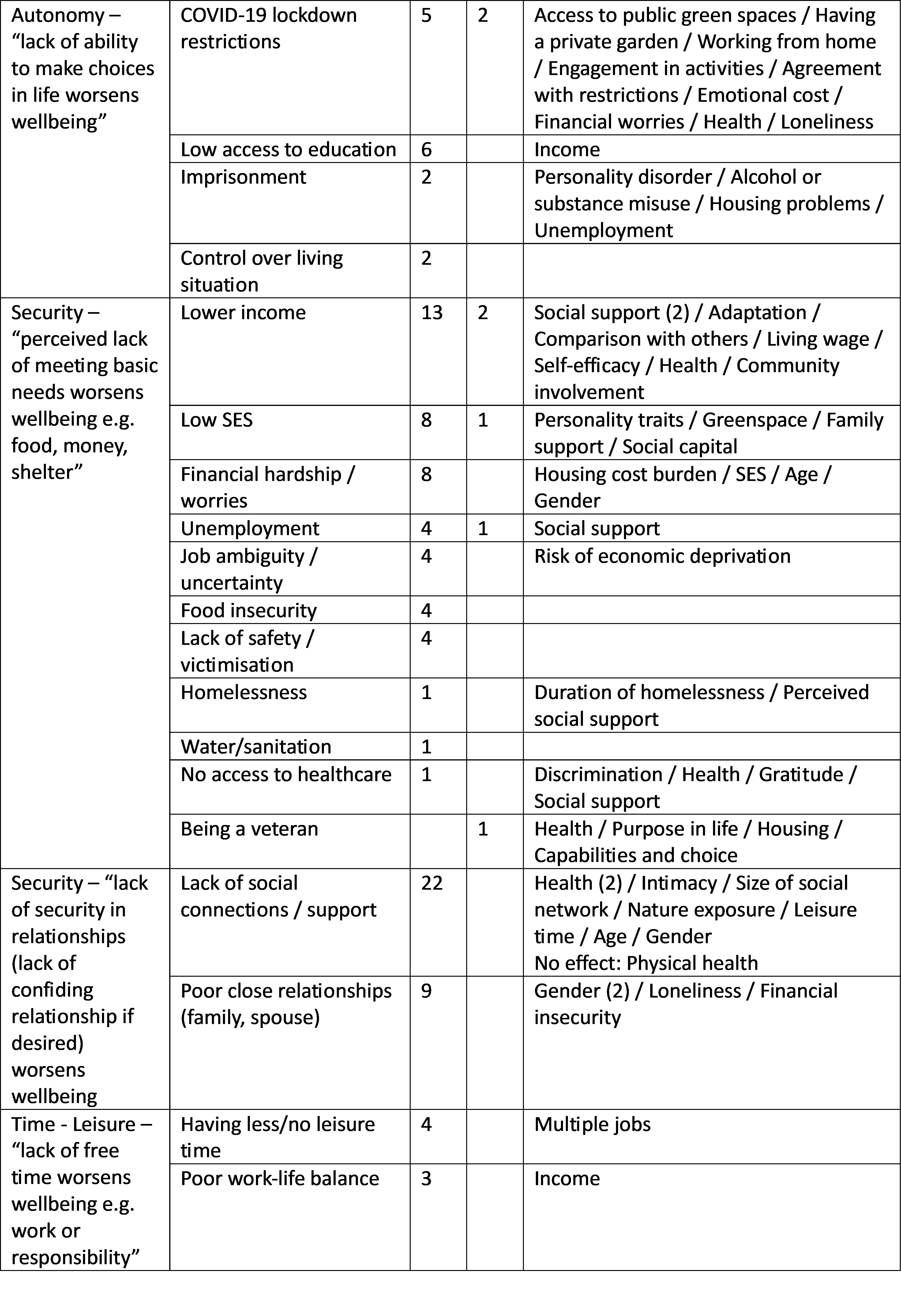
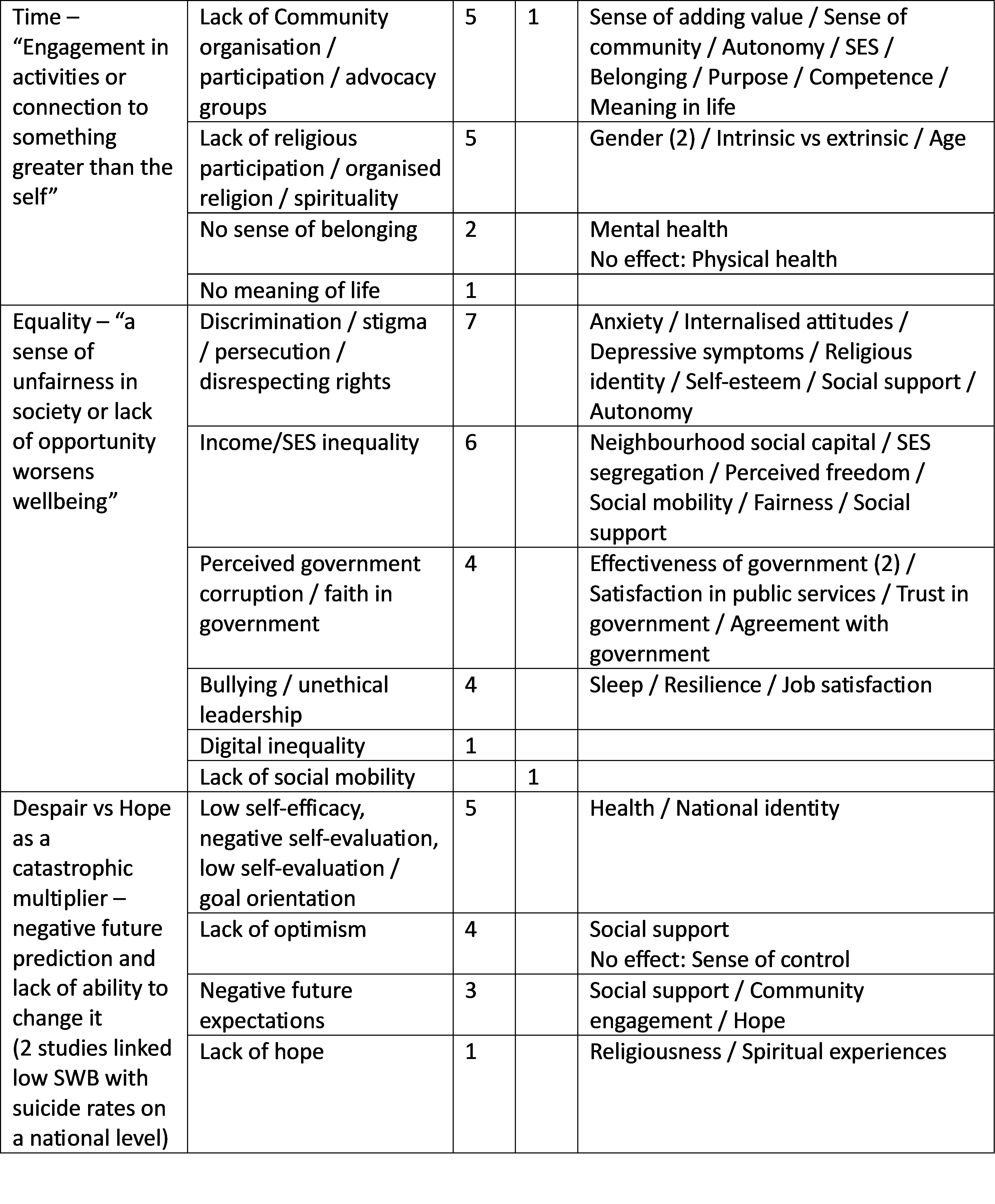
A number of studies identified relevant factors for considering spillover effects:
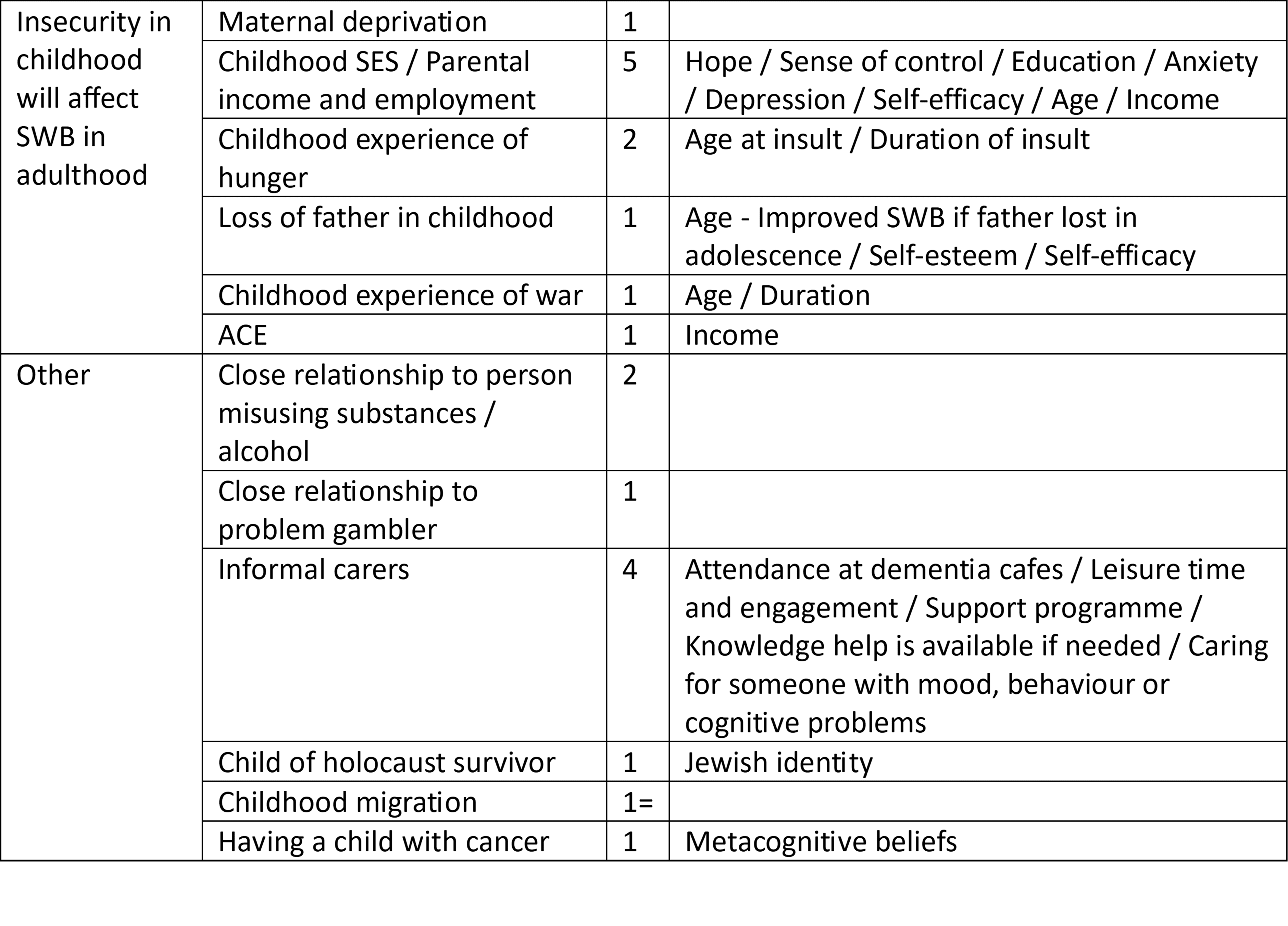
Of course, there was a large number of factors which didn’t fit my matrix that appeared in research:
So, for the sake of transparency, I did alter my matrix following this research in one domain – while I had included leisure time in my initial framework, I hadn’t considered having time for purposeful or meaningful activity. For readability, I altered my ‘guess’ in this regard but this was a post-review addition. It was a blind spot, and I think it was based on my own biases i.e. as a doctor, I perhaps take it for granted I find my work meaningful. I know 80000 hours may disagree, but it doesn’t change the way I perceive my work, how I derive value from my job, and generally think working in medicine, in psychiatry in particular, and in the NHS, reflects my personal values. It’s easy to take for granted, but being able to spend my work hours in this way is perhaps a privilege others cannot enjoy.
Perhaps less overt biases are coming into play, but finding the factors which didn’t neatly fit my matrix (after correcting that oversight) did not lead me to doubt myself. I’m not arguing any of that work is invalid or irrelevant, but for the purposes of the matrix, I didn’t feel bad for excluding them. Happy to be challenged, but here’s (quickly) why:
- It seems plausible to me that due to innate/genetic factors people have traits or overall ‘good wellbeing’ genes which means they are naturally prone to rate their wellbeing higher. This, as well as other immutable characteristics (e.g. age) aren’t changeable if considering wellbeing interventions.
- Other internal factors e.g. coping skills, emotional intelligence, I felt could be related to spillover effects from childhood experiences or childhood/adult adversity, or similarly be innate. My personal bias is that problem-focussed interventions to ‘improve self-esteem’ and the like are less helpful than general measures to allow children opportunities and environments to thrive within.
- In terms of situational/external factors, I felt many of these (natural disasters, ‘stress’) are unavoidable in normal life, and others (having children, getting married) probably shouldn’t be mandated. While it’s important to consider when people may require additional support, I think ‘wellbeing’ should be incorporated in larger discussions about disaster/future preparedness i.e. it could be considered along the matrix, but shouldn’t form part of it
- In terms of the behavioural factors, I alluded to this above in considering if these are ‘causative’ factors or not.
- The only exception is probably thinking about living standards, local environment, access to greenspace, pollution, etc which are very much not ‘people problems’ but ‘societal problems’ and likely related to SES, income, etc. It’s likely a limitation of my people-centred wellbeing matrix if this doesn’t weight appropriately in other measures (Leisure, Equality, Security i.e. adequate shelter, safe neighbourhood and ability to spend time in nature).
Overall, I felt my matrix held up reasonably well as a way of categorising existing SWB research, and my assumptions weren't too wild to be unsupported in literature.
How could my framework be helpful in practice?
To further expose my agenda: I do think mental illnesses have a huge impact on wellbeing, and historical measures of quality of life have somewhat underestimated their impact. I generally think using a wellbeing approach helps to accurately judge the impact of these conditions; while schizophrenia and bipolar affective disorder are related to significantly reduced life expectancy (not due to suicide), mental illnesses rarely cause physical impairments or direct mortality.
To take the matrix and use it in practice (0 = death, 1 = year at wellbeing baseline) for depression, based on my clinical experience:
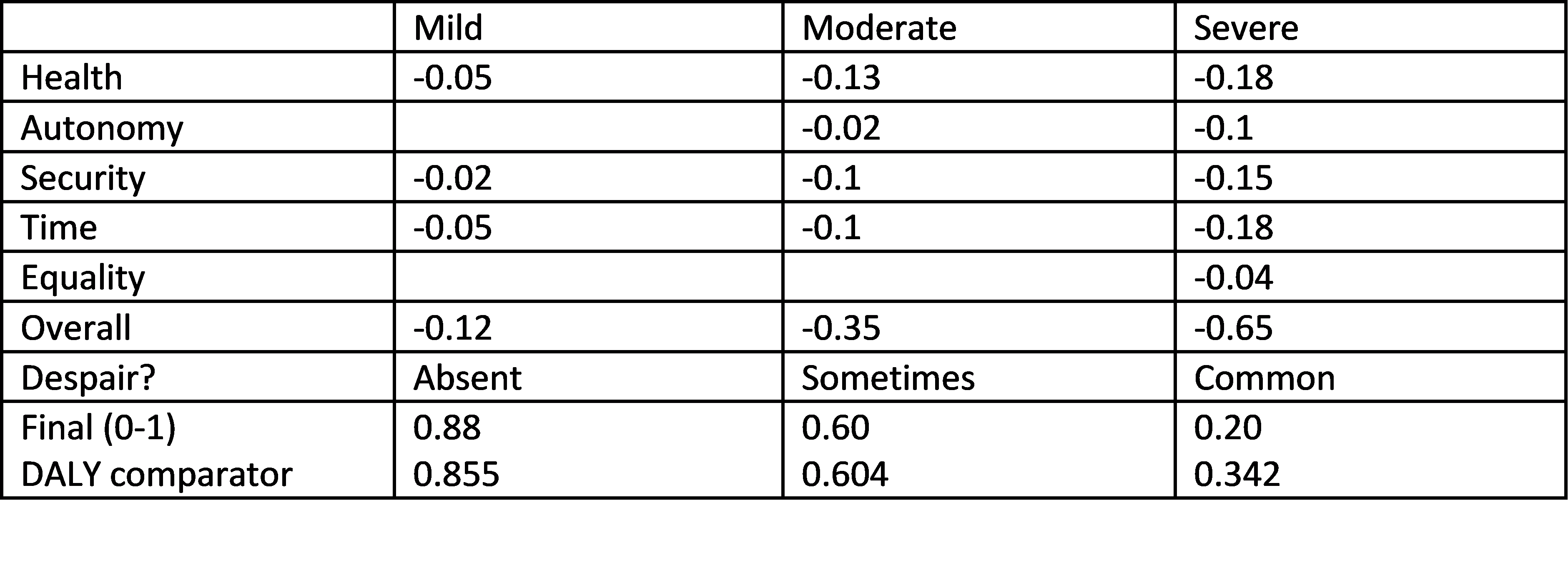
It’s slightly reassuring my ‘guesses’ weren’t too outrageous compared to the existing DALY weightings (I guess you have to trust I wasn’t cheating), but also not so similar it made all of this a completely pointless exercise.
To be brief, rather than just looking at ‘years lost’ or how unpleasant one judges an illness or impairment to be, a matrix allows an illness like depression to be considered more holistically:
- Health – Depression is an illness, and results in lots of ‘unpleasant’ symptoms – low mood, fatigue, disturbed sleep, distorted perceptions of the world, and intrusive, negative thoughts. It can also affect appetite, and seems to compound the negative effects of other illnesses (e.g. post-MI (heart attack) depression)
- Autonomy – At the more severe end, people can find it difficult to function and make choices for themselves; they can end up in hospital
- Security – Depression is a common reason for people to miss work, have difficulty getting back into work (i.e. risks financial security), and at the more severe end people can have difficulty caring for themselves (i.e. maintaining adequate food and fluid intake, accessing healthcare). It can also strain close relationships.
- Time – Depression causes fatigue and also leads to people being unable to enjoy activities they used to, it’s common to withdraw from these pursuits and also from social interaction i.e. while the amount of time they have doesn’t change, they will be unable to spend this in leisure pursuits or meaningful activity with more severe depression
- Equality – With this being relatively common and discussed, it’s unlikely milder forms of depression will result in inequality. Again, for the severe end, this could be stigmatising e.g. if people cannot maintain self-care, lose status at home/work or end up in hospital
- Despair – At the more severe end, depression can lead to suicidal thoughts and acts, so this should qualify for a catastrophic multiplier (currently arbitrary as not standardised across other conditions)
For ‘spillover’ effects, using a systems-approach: having a loved one suffering with depression is worrying, and this is more worrying the more unwell a loved one is. Similarly, the increasing loss of functioning because of more severe depression leaves others in the household taking on their responsibilities to keep the system functioning.
A system-approach allows for consideration of times where someone suffering with depression has particularly bad effects on other members of the household. If someone is the main income-provider, one could imagine the threat to financial security is particularly acute for all household members. Similarly, for anyone with caring responsibilities, struggling to function will be particularly bad for those they care for. This tends to be the reasoning behind active screening for postnatal depression as this affects the care, bonding and emotional/social development of the infant when untreated. It is then highly cost-effective to treat postnatal depression, not just for the mother’s wellbeing, but all the benefits this has for the infant. Outside of this specific example, parental mental health clearly has an impact on children (poverty of close relationship, threats to security) and it’s therefore particularly important to address mental health needs of parents with young children for their wellbeing throughout life.
Measuring interventions
It follows that effectively treating depression improves the wellbeing of the person suffering from depression and, to some degree, their household. If you then wanted to roll out a scheme e.g. a local programme for people to access free cognitive-behavioural therapy (CBT) for depression, and wanted to judge how cost-effective this would be for wellbeing, I guess it would be along these lines:
- Firstly, you would need to know the cost of this scheme i.e. setting up the scheme, training people to deliver CBT, spaces/technology for people to have CBT. You then need to predict how many people could be seen in one year
- Then you would need to know the prevalence of depression in the community (roughly) i.e. how many people this could potentially benefit in the longer-term, as well as the ‘average severity’ of depression in sufferers. For spillover effects, it might be helpful to know the prevalence in working-age adults, parents, etc.
- With that information you know how many people could get the free CBT in a year, and multiply this by the ‘wellbeing impact effect’ of the average severity of depression e.g. the service can see 1000 people in a year, the average severity is ‘moderate’ (0.6 wellbeing-adjusted impact years), so therefore there are potentially 400 WAIYs you could get out of this intervention
- Let’s say 50% of people do recover completely with CBT (guess stolen from here) – that gives you 200 WAIYs
- Of the remaining 500 people, another 160 show a reliable improvement (i.e. they are still depressed but they are now mildly depressed vs severely). 160 people being mildly depressed (0.88) vs moderately depressed (0.6) gives you an additional 44.8 WAIYs – a total benefit for the intervention of 244.8 WAIYS per year for the cost of providing CBT.
- You can similarly model spillover effects to work out the likely benefits to wider household members/community e.g. in reducing unemployment.
Obviously, it’s based on a lot of guesswork, so you’d want to collect more detailed information to understand the service when it’s up and running i.e. then you could see how many people are accessing the service with different severities of depression, their recovery/improvement rates and then judge the true impact on WAIYs vs the estimate.
You could then assign a cash value for what one WAIY is worth to see if this is greater than the costs, or have a minimum cost-per-WAIY hurdle that interventions have to meet in order to be considered ‘worthy’ of public funding. You could compare this to other treatments for depression to see if this is the best use of money.
One quick diversion to release the bee in my bonnet - I would discourage the assumption that psychotherapy does not result in harm and so there is no need to consider this in CEAs. Firstly, we do know that a fraction of people deteriorate during treatment (whether or not this is due to the therapy itself). It also seems like a logical fallacy to assume harm cannot occur – if talking to someone can improve one’s mental health, it makes sense that talking to someone can worsen one’s mental health. Again there are clear examples of this – it used to be commonplace to offer debriefing sessions following a traumatic event; it has since been demonstrated this is, at best, unhelpful, and at worst increases the risk of PTSD. It is clinically accepted that therapy can ‘destabilise’ people i.e. talking about painful memories can make people feel worse before they feel better, and so if people are in crisis, therapy is contraindicated without a robust safety net (which may not be available in resource-poor settings). Similarly, assuming it is universally helpful is an error – some people do not want therapy, some will not be able to reliably attend due to work/family commitments, and the rates of non-improvement, deterioration and drop-out before the minimum number of 'effective' sessions needs to be included.
Usually there are guardrails around therapy’s harms, because if therapy is having a non- or adverse effect, people will drop out. However, this makes evaluating risks difficult because those who drop out of therapy do not complete outcome measures. This is also the risk of using the wrong form (or modality) of therapy, especially if providing this as the only treatment option in resource-poor settings e.g. if you provide a therapy only suited for mild depression, you can imagine that people actually suffering more from another illness, or more severe depression, will get worse or not improve while still trying to engage as there's nothing else.
If adopting a task-shifted approach (i.e. you ask non-clinicians to deliver therapy), you have to factor in adequate support for the person expected to take on these therapeutic relationships, and in some populations you can imagine they will encounter a much higher burden of patients who have had traumatic experiences than what is captured in RCTs in other settings – it may directly harm those delivering the therapy to put them in that position, and similarly a lack of support/supervision can lead to even trained therapists straying into counter-therapeutic territory to harm those accessing it. If a therapy group collapses because it can’t be managed safely by a non-clinician, this will likely make everyone in the group worse. And then what?
But, back on topic, for a fairer CEA, you would need to factor in the service being underfilled (e.g. if the country was completely opposed to CBT on principle, or your scheme was completely impractical in its implementation). You would also need to collect data on how many people dropped out (assuming no effect in the remaining people otherwise unaccounted for) and who got worse.
- Again, stealing data from the above paper, 6% of people got worse; let’s say they become severely depressed (0.2) vs moderate (0.6). -24 WAIYs, for a net total of 220.8 WAIYs
- To be fair, you should also compare this against the alternative i.e. what is the likely outcome of these 1000 people not having free CBT in terms of rates of spontaneous recovery (adjusted for time spent sick vs time to recovery/improvement with CBT) and deterioration which might produce an even stronger argument for the CEA of the intervention if you show, without the service, we expect X number of people to get worse.
However, this essentially works best when I can gauge the acceptability, uptake and benefit of my intervention with reasonable reliability. If I was thinking about providing CBT to an LMIC setting, I would have to proceed with more caution given the issues I raised with RCTs in judging whether CBT is similarly helpful as an intervention in an LMIC and my lack of lived experience within an LMIC.
The greater issue, though, is me stating that for this amount of money, this intervention for depression is the best way to improve your (population of LMIC’s) wellbeing. It's based on my assumptions about wellbeing from my perspective, and in the name of subjectivity, I could be completely wrong. I could try and support locally run research to collect more data to be sure of my assumptions, or impose an external RCT and accept it could be misleading. However, this doesn’t really address the fact that I’ve decided treating depression is the best use of funding in the first place, which means I’ve not only made assumptions about depression’s effect on wellbeing, but also every other problem that community might be facing i.e. I’ve done a comparison WAIYs estimate for different issues, compounding my assumptions. I’ve already admitted that the existing research into wellbeing is in its early days and heavily weighted by wealthy countries with different cultures and so it might not be that helpful in considering something like CBT in an LMIC.
Unless I decide wellbeing isn’t that important to consider and it’s worth waiting (likely) decades for this research to come to fruition, it is always going to involve a certain amount of guesswork. However, it also seems to me that the focus on ‘subjective’ wellbeing can allow for more direct measures via trade-offs. I could, as an example, go to a community I think might benefit from my free-CBT scheme, screen people for depression and find some eligible participants. I could explain CBT and all of its benefits, and that I think they are depressed and this could help them (50% chance of recovery! 66% chance of improvement!). I could then offer the CBT, or the equivalent cash-value sum of providing the therapy – if no one chooses the CBT, it suggests it’s not worth the money to the people I’m trying to help. I could even return in a couple of months, find these people, screen them again and offer the money vs money plus CBT if I want an even better idea of how to judge my intervention’s ‘subjective’ benefits.
This is at least an up-front approach which avoids coercing people into CBT, and provides quite an honest CEA i.e. am I better off just taking the money I would have spent on therapy and giving it directly to this community if I want to do what they would find most helpful? Or should I be considering a way of providing access to those that want CBT but factoring the costs for people to attend if I want to make this work? E.g. if they can’t spare the time away from work/family commitments without financial compensation, but would benefit from CBT, should I be offering compensation/childcare.
Either way, there has to be some way of involving local communities and allowing them to provide feedback if there is going to be any argument for CEAs in directly improving ‘subjective’ wellbeing.
What would I be suggesting as research areas for maximal gains in wellbeing from my biased perspective?
I thought from my biased/blinkered UK psychiatry perspective on what I would be thinking were potential areas for funding which would have the greatest impact on wellbeing from my assumptions. While my framework has been informed by subjective wellbeing approaches, the overall matrix is an ‘objective’ overview of ‘subjective’ wellbeing. These are things I think generally would have great effects, potentially globally, with the caveat that I wouldn’t suggest these are priorities in LMICs specifically – this must involve local involvement and a great deal more research. [Generally addressing the global mental health gap is unlikely to be low-impact (provided it’s done thoughtfully with involvement of the communities affected).]
If I had to pick my top three:
Psychosis/Schizophrenia research
While there are arguments for mental illnesses having a strong societal context, schizophrenia is relatively consistently prevalent around the globe (1%). This is a very disabling illness, particularly for people who have ‘negative symptoms’ which is common in chronic forms of schizophrenia, and acute episodes (psychotic episodes) are highly distressing for people to experience. The current treatments are various shades of problematic (either due to Parkinson’s-type side effects, or due to metabolic side effects e.g. resulting in obesity, diabetes, heart disease). It tends to first present when people are young (i.e. late teens/early twenties) and therefore can affect people in work or higher education, or those with dependent children (thinking of spillover and autonomy).
It has a variable life course – some have one episode of psychosis and get better, some have a relapsing/remitting illness, and others have a progressively disabling course. Some people will have treatment-resistant schizophrenia i.e. it does not respond to multiple trials of antipsychotics, and therefore are eligible for clozapine (another antipsychotic which works better than others, but has a risk of serious complications and so requires intensive monitoring of blood tests and heart health). A good proportion (60%) respond, but others do not. Schizophrenia remains highly stigmatised as an illness, reduces life expectancy, and can lead to protracted hospital admissions.
Generally, it feels we are barely scratching the surface of understanding this illness properly and are sorely in need for better treatments. Regardless, it’s important to ensure timely treatment if someone does become unwell (as the duration of untreated psychosis is a significant factor for how well and how quickly someone recovers) and to support them in returning to their usual activities. There’s ongoing research about earlier use of clozapine for this reason (i.e. not waiting for two treatments to fail), or genetic testing for antipsychotic response, and other ways to make antipsychotic/clozapine treatment less invasive e.g. finger-prick blood monitoring. CBT for psychosis is relatively new and has some very good wellbeing-oriented results, as does family-based therapy.
This is a high-impact area where research and advances in treatment could be high-yield.
Interventions aimed at women of childbearing age to empower control over pregnancy, and generally any intervention to benefit young children
I don’t want to risk over-simplifying a very fraught topic, but this UK-based charity has a lot of information to help understand the issues women face in trying to ‘break the cycle’ if they have children removed from their care (often due to being in a violent relationship, or mental health/substance misuse problems). I would endorse any supportive measures for safely escaping domestic violence, etc; or proactively engaging vulnerable women or those at risk of exploitation in discussions about long-acting reversible contraception if desired. While children’s mental health services are important, I personally find it hard to reconcile children who are born into very difficult situations receiving support for their mental health (which is not really addressing the reasons they may be suffering) or interventions from social care, but this drops away after they turn 18 and they go on to have children themselves. I feel this leads to an odd disconnect between support for children in ‘bad homes’ but seeming indifference or derision towards parents/mothers who are unable to provide a supportive environment.
Based on what I’ve said about spillover effects, it seems these problems should be addressed in tandem – women should have a supportive environment where they are more able to exercise control over pregnancy and choice of partner, and difficulties the parents face need to garner the same amount of support (regardless of the effects on the child) to ensure children are in an environment to promote their wellbeing in the long-term.
Psychedelics in palliative care
Alright, I don’t really see this as a key priority, but it’s something I surprised myself with. To keep it short, I’ve been highly sceptical about psychedelic-assisted psychotherapy – I am keeping an open mind, but so far the research I’ve come across has been unconvincing (you can’t ‘blind’ any trials, recruitment is often targeted to people curious/believing in psychedelics), and I still remember the hype about ‘micro-dosing’ which has since been debunked. For what it’s worth, I’m pro-legalisation for the sake of these drugs not being as harmful as alcohol, I just dislike the ‘medicalisation’ route. It ends up leading to a politicisation of medicine (e.g. medical cannabis being recommended for a range of problems with absolutely no basis in evidence) which completely taints any discussion about harms/benefits.
I also generally think the impact of psychedelic-psychotherapy is fairly minor and likely costly, the proposed application of psychedelics requires controlled administration (i.e. in a clinical environment) alongside relatively intensive psychotherapy which makes it likely to favour relatively wealthy people, not in crisis, with jobs which will allow them to work around these sessions. Obviously in certain groups/situations it could be very useful (i.e. survivor’s guilt in PTSD), but the research isn’t quite there yet, in my entirely personal opinion.
However, in my trawl through all the wellbeing research and evaluating my framework, I did come across a couple of tangentially-related studies about the effects of psychedelics in promoting positive attitudes to death and reducing existential fear (i.e. despair). With even a one-off dose of LSD having relatively enduring effects. It makes sense to me to consider the use of psychedelics for people with life-limiting illnesses (e.g. in palliative care), or perhaps in the elderly more conservatively. Palliative care is set-up to be more holistic and spiritual, and opening conversations about death is very much their strength (I’d argue much more appropriately than thinking of this in psychotherapy).
Reducing fears, anxieties and existential dread could have significant gains in palliative care, and may reduce the use of opiates and other drugs which negatively affect wellbeing outside of limiting pain i.e. they are sedating, cause constipation, and interfere with enjoyment of life. Pain is highly related to anxiety (one of the first surgical ‘anaesthetics’ used was Valium), and it’s not uncommon for people to feel physical pain as a result of psychological distress (tension headache is the classic example), so it wouldn’t seem too far-fetched to imagine psychedelics could have a hugely beneficial effect on wellbeing in this context.
Final thoughts
Thank you to anyone who has spent time reading my earnest, but likely misinformed, approach to wellbeing as it relates to mental health. I’d be interested to know how far I’ve strayed off track, or if there is any weight to my general argument: having an evaluative framework based on subjective concepts of wellbeing (allowing synthesis of existing research and providing the skeleton for these cross-comparisons) is useful. I think the end result – producing something which could be considered a ‘tweak’ of the DALY to better reflect subjective concepts of wellbeing is a little easier to adopt and understand than creating something completely new.
[References linked in-line as this is long enough! Sorry my Word tables have formatted quite badly.]


Hello LondonGal (sorry, I don't know your real name). I'm glad that, after your recent scepticism, you looked further into subjective wellbeing data and think it can be useful. You've written a lot and I won't respond to it in detail.
I think the most important points to make are (1) there is a lot more research that you suggest and (2) it didn't just start around COVID.
You are right that, if you search for "subjective wellbeing", not much comes up (I get 706 results on PubMed). However, that's because the trend among researchers to refer to "subjective wellbeing" rather than "subjective well-being", ie with a hyphen, is very recent (as, AFAIK, is unrelated to COVID). Searching for "subjective well-being" yields, by comparison, 4,806 results.
If I expand the search to other keywords, namely "happiness" OR "life satisfaction" OR "subjective wellbeing" OR "subjective well-being", I get over 150,000 results on PubMed. This is displayed below. Note the results go back to 1838, but the research only really kicks off after 1980.
I'm not an expert in academic databases, so I don't know how comprehensive PubMed is of all research, but I'm guessing it's a subset. FWIW, Ed Diener et al. in a 2018 article on subjective wellbeing states that there were "170,000 articles and books published on the topic in the past 15 years" although I haven't looked into his numbers.
You might be interested in this article in the recent World Happiness Report which looks at various trends related to happiness, including academic interest, and find the fraction of articles on the topic has been trending up since the 80s: note the steady linear increase on the logarithmic y-axis.
Hence, as you suspected, many of the topics you raise here are reasonably quite well-trodden in the literature.
If you're interested in looking further at the pros and cons of the WELLBY, the easiest thing for me to point you to is HLI's To WELLBY Or Not To WELLBY report and references therein. You may also find this reading list useful.
In terms of the state of the literature, if you'll forgive further laziness and self-promotion, I'd suggest my EAG London talk. The short answer is that 'we' (ie happiness researchers) know quite a bit about the nature and measurement of wellbeing and its causes and correlates, but relatively little about what the best ways are to increase it; work on WELLBY cost-effectiveness is barely older than COVID.
Hi MichaelPlant, [Edit: Jk - I don't get the comment about my username/real name, I saw a mix being used on the forum, but I might have missed some etiquette - would you like my real name? Just 'hello' is fine if you'd prefer - no offence taken.]
Thanks so much for taking the time to read and respond! I was hoping to get more insight from people within EA who might be able to fill me in on some of the more philosophical/economic aspects as I'm aware these aren't my areas of expertise (it was very much a 'paper' EA-hat I was trying on!) - I felt furthering my online searches wasn't as helpful as getting more insight into the underlying concepts from experts and hoped my post would at least show I was interested in hearing more. Thanks for the links as well - I did come across a few of them in my approach to this work, but will take your advice these are worth looking at again if you think I've not appraised them properly - you definitely know best in this regard!
Also, apologies - you might be right in saying I didn't structure a paragraph very well if it has left anyone with the impression I was suggesting subjective wellbeing research has only been in existance since COVID. My own graph disproves this, for starters! I think it's this paragraph from the first section I've not phrased well (italics added).
I was trying to emphasise the relatively steep growth in interest over the last few years due to questions about cost-effectiveness (e.g. WELLBY), which as you mention is 'barely older than COVID'. I don't actually think we disagree here so I'll need to think how to rephrase it to avoid conflating this with SWB research as a whole - to be clear, I don't think your reading of this was unfair and I can phrase it better.
I'm not too sure I was ever arguing I was doing an exhaustive literature review (?) - I felt I stated a few times this was non-scientific, should have no weight, etc. My goal was just trying to get a quick overview as more of a sense-check, but didn't want to limit my reading to the first x number of pages in case that was biased - I chose very limited terms and stated them so it would be clear how I did the search, which allowed you to double-check I wasn't pulling anything dishonest (impressive that 7 papers have been added since I did the search last week - clearly there is a lot of interest!). If I set out to do a completely exhaustive review, you're right to suggest the terms you did (I would add "SWB" as well), but I'm not sure that would be a reasonable expectation of something like an "abstract-only" non-academic review from a visitor with a full-time job when that returns thousands of results...
I'm sorry if it appeared that selecting limited search terms was an attempt to 'downplay' SWB research as a field - I mentioned it was my time constraints that were the problem but it's easy to miss in a long post. I felt I was trying to explain throughout how interesting/useful I found this piece of work, spoke about how it changed my mind in the later sections and identified blind-spots I wasn't aware I had. I don't think I was critical of 'subjective wellbeing' research as whole - I tried to lay out my very specific concerns very clearly (e.g. in "life satisfaction" being used as an isolated measure for subjective wellbeing) but my overall conclusion was in support of finding a way to incorporate more of the diverse value these researchers were adding to the understanding of how we think about wellbeing estimates e.g. other measures, combining measures, qualitiative research, etc. I was approaching the problem with an open mind and left the exercise positively so I'm sorry to see it might have appeared mal-intentioned.
I hope this doesn't seem like nit-picking, and it's not intended as criticism of you personally as you similarly were upfront about not being familiar with PubMed; it can be tricky to get to grips with, but it might be helpful to share a quick point.
For the search that you linked that returned 150k results - if you go to "Advanced" under the search bar and click through you can see this searched "All Fields" and expanded the terms you used as they weren't in quotation marks (it's a quirk of the database that perhaps isn't true for others!). This was the actual search run from your link - for all I know this was your intent, but in case it wasn't (just judging this as a possibility based on the hyperlink):
With quotations to limit results to those specific terms (I'm not sure if that was your intent) and using Title/Abstract (PubMed also doesn't really like hyphens as you see above but I used "subjective well" to try and work around this) you get more like 20-30k results. You can use MeSH terms (key words instead), other variations, etc to push it up or down (I tried a few variations to work with 'well-being' hence this being #8). And as you rightly say, you can always add more terms to include more papers.
Again, my aim isn't to down-play SWB research at all with this point (I like the field!), it's just in case it's helpful as I use PubMed all the time and it's one of many databases which contains mental health literature. Whether 2k or 150k+ results (even a few well-written papers wouldn't necessarily be an argument against the field - it just suggests to me it's new), I still stand by my OP in being broadly positive about the area as a whole, hence coming up with a framework of my own in inspiration, I just haven't shifted much in my specific critiques of certain applications of specific aspects of SWB but I'll have a read of your links and see if it changes my mind! Similarly, if you had any further thoughts, I'd appreciate hearing them for your feedback.
Hello,
I just wanted to follow-up, as I’ve read your links as promised. I share a genetic trait of speed-reading, so this wasn’t too onerous – please forgive me for not watching a video of your EAG talk (this is inefficient for how I work) but you linked your write-up on the forum which I read instead.
I feel you may be approaching this assuming I’m a bad actor, and I’m going to further endeavour to demonstrate this isn’t the case (I thought offering my meta-analysis skills for free, my arguments above about not over-interpreting an RCT, and this post in general would demonstrate that I’m approaching this in good faith). I care about this topic and I want EA to continue having interest in mental health/wellbeing – I think this could do a lot of good. I’m not sure why being non-EA would suggest I disagree with effective ways of doing altruistic work, or that I’m incapable of contributing anything to a discussion of mental health and wellbeing given this is literally my job, and so shouldn’t offer my perspective on a public-facing forum. I want to understand more about EA approaches to my field but I’m not so selfish to ask someone to do all the work for me (a stranger), hence putting a lot of effort into my post to show I am genuinely interested in trying to understand (side note: thanks again to people who have offered to chat off-forum - it’s really appreciated, and I’m sure my opinions will change in the coming weeks with your help).
I’m wondering if this is coming across instead that I care about making another anti-HLI post – I don't. I tried approaching this problem (how does mental illness relate to wellbeing) from first principles to see what happened; I thought this was a sort of EA-oriented approach. I vaguely referenced the HLI post I commented on in my introductory comments to explain how this work came to be and interrogate my motivations (allowing others to do the same) - not linking the post/naming HLI, calling my contribution an 'overly technical diatribe' and not mentioning HLI at all was meant to dissaude from the idea my involvement in that thread should be considered on it's merits. It was a reflection of my internal responses which I thought was important to interrogate in trying to adopt a less biased approach in my work (appraisal of SWB as a whole). We reflect all the time on unconscious vs conscious in psychiatry (blame Jung) but maybe this was weird to mention. Either way, It’s not like I’m competing for any EA space/funding which would make this something sinister or detract from HLI, and I’m not a big deal at all to think I could do this even if I wanted to.
Anyway, I’m confused why you’ve said “’we’ (i.e. happiness researchers) know quite a bit about the nature and measurement of wellbeing and it’s causes and correlates, but relatively little about the ways to increase it…” when you’ve linked several resources that suggest my heuristic approach isn’t too bad and my main question was about putting this in practice. I’m not too sure I understand how your comment seems to contrast the idea of my overly/”deliberately” shallow non-academic review with several sources supporting my approach. Isn’t that a good argument for interdisciplinary work? I’m not really understanding the tone of your comment when my post wasn’t ‘here’s my systematic review of wellbeing, it’s a new field with nothing useful to say’ but rather, ‘this is what makes sense to me, this doesn’t seem too out-there?, could this be used helpfully?’
In terms of the Diener, et al. paper– I had come across this author before in my work for this post (but not this specific paper). They use the comment about 170,000 articles (paper was accepted in 2017) in their introductory paragraph as a set-up for their narrative review of the literature – so I don’t need to talk about Google Scholar or try and ‘verify’ the numbers. They only mention it to talk about the growth of interest in SWB, which we all agree with.
This was a lovely piece to read, and I’m glad you directed me to it. It’s an extremely thorough review of wellbeing literature (32 pages excluding refs in PDF form, 439 different references). I’m not too sure why you’ve linked it, as it seems to be really in support of a lot of my work? Perhaps this was your intent as you don’t comment on my more specific criticisms, or my overall framework or findings. It's not clear in how you framed it, which seemed to be as a counterpoint to me post, but maybe it was an agreement with the broader points you didn't want to address in detail.
While I’m sure you’ve read this paper as you referenced it, for anyone else following – I can summarise the areas where this review supports my own:
It discusses concerns with single-measure SWB that I identified e.g. issues of subjectivity as a whole, reluctance providing honest answers to researchers, differences of meaning in various contexts, how people retrieve the relevant information to respond (likely too quickly to provide an evaluative judgement) and influenced by current mood/prior discussion (my joke about coffee). They point out that studies ‘on their own, provide little evidence regarding the validity of the measures themselves’, and conclude that, “although different camps have emerged that advocate for one set of measures over others, we believe that such advocacy is premature… we recommend that, when possible, researchers should include a broad array of measures….”
It lists several predictors, correlates and causes of SWB: social relationships/social capital; income and wealth; religiosity; demographic factors (e.g. age); health; genetic and personality factors; internal factors (e.g. self-esteem); basic needs (e.g. food, shelter) and safety; autonomy; ‘freedom’; ‘balanced life’; ‘adaptation’ to life events such as disability; cognitive processes; ‘fair and efficient’ law/government… These were all factors I either included in my framework or identified in review and explained my reasons for excluding.
The paper was arguably even more in favour of cultural contextualisation than I was e.g. “Even when a relevant term such as happiness is clearly defined, it is worth exploring whether the term [is] used in similar ways across cultures and time. Most philosophers and historians agree that the concept of happiness has changed over the years. In antiquity [the authors reference ancient Greece], this concept centred around good luck and fortune, whereas contemporary Americans view happiness as a pleasant experience over which they have control and something that they can actively pursue.” The authors go on to mention the differences of contemporary understandings of happiness between American (personal achievement and intense positive emotion) and Chinese people (spiritual enrichment, harmony and dialectic relation between happiness and unhappiness).
It spends a long time talking about the difficulties of interpreting causal vs correlative relationships, or third-variables, in describing how these factors relate to SWB.
They are consistent in pointing out all the ‘open questions’ that still need to be answered in understanding and measuring SWB, and how to apply this to policy decision-making. They also suggest research into other methodologies to answer questions about predictors and outcomes of wellbeing to define these relationships better, and describe a variety of ways SWB can be measured (outside of various self-report tools).
The conclusion of this paper:
It seems they think there is a place for me within wellbeing research and I’d discourage anyone adopting the idea that only evaluating a problem from one perspective strengthens your understanding – it’s much more likely the ‘most right’ answer lies in-between various disciplines to maximise experience and expertise.
Your next link – the World Happiness Report, seems to just be cited here to further illustrate growing interest in SWB (which I haven’t disputed). It does highlight as a pull-quote on the first page: “The recent pandemic has likely had a strong impact on popular conceptions of what is most important for a good life, and indeed on how society can foster collective improvements in well-being”
…Again, I’m not sure how this discounts my (poorly-worded) comments about the effect of COVID on the field. It might be to suggest it was an oversight to omit ‘happiness’ from my search which would produce a different graph than the one I used, but I’m struggling to see the relevance of this above what I’ve already addressed (i.e. your graph includes any paper mentioning 'health' or a number of other vague terms due to the search) – it seems we all agree there is growing interest in SWB, and there is an increasing interest over the last few years, for one reason or another.
The report goes on to mention the same issue I did in that there are a few early-adopter countries in the field of wellbeing research, but this is becoming more global over time from the ‘earliest mentions’ in the economics literature from the 1970s (they made this comment, not me, hence their graphs starting in 1970):
This was what I was representing in my pie chart (I'll admit this is slightly prettier) to talk about interpreting the existing research (i.e. the issues the Diener paper raised about cultural understandings of wellbeing/'happiness'). The report also mentions the diverse number of measures being used for SWB (10 domains and 38 individual measures) to discuss how best to measure world happiness. These are elaborated upon further in the Appendix to the chapter you linked, along with other graphs representing country-based origins of SWB.
In the ‘challenges’ section, it explicitly talks about the difficulties in composing ‘any new indicator framework aimed at capturing a meaningful concept such as well-being or progress’ and how that can combine different measures, or aggregate individual experience into summary numbers for groups or populations, to ‘express values through numerical weights’ – this is exactly what I had a go at doing with my framework/matrix. Interestingly, it also encourages not focusing on over-analytical approaches to “unanswerable questions” (they talk about climate change as an example) and delaying actions which provide benefit for the sake of attempting ‘futile’ over-analytic approaches of far-future impact calculations. This seems to be similar to my conclusion.
The ”To WELLBY or not to WELLBY” I read prior to this work and I’m afraid I still disagree on re-read for the same points I made in my original post (single-measures in isolation, life satisfaction, conversion to different settings). I’ve highlighted that this isn’t a ‘fringe’ opinion derived from my ignorance when looking at the other materials you linked. I also clearly will not agree with ‘Affective mental health, usually measured with depression scales, involves questions about how people feel, which will directly relate to SWB’ (an unreferenced footnote) – I feel I have explained this point very clearly in my post and cannot take HLI’s report as ‘stronger’ evidence that would lead me to reconsider; I have addressed this from my relevant expertise and from listing the PHQ-9 in a previous comment.
Also, I’m really sorry, but that article mentions repeatedly HLI’s psychotherapy meta-analysis I’ve already talked about on this forum (as have others) in terms like “(3) Using SWB will reveal previously under-captured benefits, such as it has already done for psychotherapy,” and alludes to future plans to publish research on issues such as the ‘neutral point’ on SWB scales, and agrees comparing SWB scales isn’t supported in literature (i.e. to convert to the LS evaluation used to support the utility of the WELLBY) but suggests things that ‘could’ be done to manage this. It’s putting me in a difficult position to discuss this link when I’ve explicitly stated I don’t want to reopen old arguments and I feel any further critique of HLI isn’t appropriate at present on this forum. I feel statements like those in the article are otherwise inciting me to dig around HLI’s website to see what was built off these prospective ideas, and it’s just going to devolve from there. Perhaps you could highlight the parts that disagree with my original post in terms of your opinion vs that of HLI if you really think this offers strong counterpoints?
In terms of your linked EAG debate, I’m running into similar problems. I didn’t see much disagreement in the early parts discussing the importance of SWB and ways of measuring it, but otherwise it focusses on HLI’s work and references the meta-analysis, framing it as: “We looked at cash transfers and group therapy for depression. We did a meta-analysis of each. We looked at the available studies. We had about 140,000 people total across both. So we really tried to look at all the available evidence that was there. We did some kind of technical jiggery-pokery to convert it into wellbeing scores. And what we found was that the $1000 cash transfer has about the same per-treatment effect as group therapy for well-being. You can see that the cash transfer does have an effect, has a much longer lasting effect. But the effect of treating depression is larger, but fades sooner.”
From my previous comment on the HLI post on this forum, you must see how this is problematic to link here. It’s not arguing against anything I’ve said in my post, and I can’t go into the reasons why I disagree with later points without restarting settled arguments. I’m assuming you didn’t reply to my comment on your post about HLI as you didn’t want to engage with me about my issues with the meta-analysis etc, and I think it would be implicitly crossing a boundary for me to reproduce those arguments here. I think you are and were completely within your rights to disengage with that discussion and I respect that choice - I don't want to put you in a position where you feel you have to engage again in something you found negative to avoid appearing to 'concede' any points about HLI and so I cannot comment on HLI-related links.
I'm not really 'online' very much and it was part of my reflection about my comment on the HLI post - I felt it was only fair to similarly 'put myself out there' and invite criticism of my work given how I imagined you and the HLI team might have felt in that thread. I tend to post random artwork etc online - it would feel really harsh if in the middle of some drama, a critic's sister happened to be an art professor and came in to critique my art. I thought it was only fair to allow the same to happen to me.
Awkwardly, your opponent in this debate seems to support my approach in this post on several fronts. Their conclusion:
I felt I was doing that but trying to put it in EA terms for CEA-purposes, and it’s not clear to me why this rebuttal was considered ‘wrong’ (?). FWIW, I have also come across the @ryancbriggs post on the capability approach (which is something referenced in the counter-argument) and I felt much more closely aligned with these ideas than HLI’s. [I'm sorry, I don't know the etiquette on 'tagging' here - please ignore me if this isn't expected when linking to someone's work].
I’m not going to go through each of the items on the HLI reading list you also suggested (as it’ll be too long), but similarly it wasn’t presented in reference to anything specific, and I’m not sure if it’s just to demonstrate the idea I might benefit from more reading into SWB. I’m struggling to agree that I’m vastly under-competency from the resources you did link to understand how these would be revolutionary to my understanding.
Honestly, I’m pretty confused, perhaps I’m not reading the tone of your post correctly - very possible. I do appreciate you linking these papers/reports but I’m struggling to understand your overall point (my interpretation was you didn’t think I knew enough for my post to be very valuable, especially on the basis of a search you felt I had conducted poorly/with an aim in mind to downplay SWB - FWIW I didn't think 699 papers was weirdly small to anticipate this being the perception). From the HLI-related links you’ve chosen, perhaps we just disagree on certain things, which is fine, but your comment also didn’t highlight all the ways my approach fit in with other work in this area, and in complete reading of those papers. I think that omission from someone considered well-known in this area in EA does invite negative conclusions of the post as a whole and suggests those sources devalue my work much more broadly.
I’ve been clear I’m not approaching this with any expertise out of my field (mental health), and I have a lot to learn - I'm open to the idea further discussion will lead me to change my mind [I don't necessarily expect Michael to respond, he certainly shouldn't feel any obligation, I'm referencing other people kindly offering their time!]. But common ground is helpful as it suggests interdisciplinary work (similar to what went into the DALY, etc) is possible for wellbeing measures too. I’m not sure if taking a stance like “happiness researchers” just know more/everything about wellbeing/SWB is anything more than severely limiting – if so, I suppose I could be saying no philosopher has any right to comment on mental health as “we” (psychologists/psychiatrists) have got it, so shh.
I disagree with this - not only is this a wild take in psychiatry of all disciplines, but experience has taught me multidisciplinary work is key in providing the best care for patients and solve problems much more effectively. It prevents people working in silos and wasting time. Is it really the case in EA that any particular speciality field (or EA as a whole) ‘stakes claim’ on something like wellbeing which is inherently cross-discipline, to say there’s no benefit from other ideas? I think there's benefit in keeping concepts accessible vs telling people they won't understand and should consider a 'reading list' to contribute - the point of interdisciplinary working is to avoid the need for everyone to be competent in philosophy, economics, psychiatry, psychology and social science etc to have an opinion - you invite people with detailed understanding of their specific area to discuss and find solutions. I'm not suggesting EA people need to do medicine/psychiatry, read textbooks and papers to understand mental health, just maybe there is value outside of the 'bubble' of "happiness researchers".
It 100% may just be a communication thing, but this was more of an olive branch than perhaps it appeared. I think perhaps it is too late for me to strike this tone with HLI and its members (again, this is fine, it doesn't offend me - it's completely fair as a take) but felt it was worth responding anyway in case others might have felt I've been mean-spirited. Just culturally, this is a small forum with a lot of power, and it's difficult to understand as an outsider. I was surprised to learn a lot of these linked resources seemed to suggest a closer alignment than I assumed and perhaps there is a role for non-adversarial non-EAs approaching some otherwise intimidating concepts in good faith for good outcomes.
Hey LondonGal, thank you for following up on this. I appreciate you clarifying your intentions about your post. Our team has read your comments and will take your feedback into consideration in our future work. I’ll hope you’ll forgive us for not responding in detail at this time. We are currently trying to focus on our current projects (and to avoid spending too much time on the EA forum, which we've done a lot of, particularly recently!). I expect that some (but probably not all) of the points you’ve raised in your original post will be addressed in some of our upcoming research. Thanks again for engaging with our work, and for sending the olive branch. It’s been received and we’ll look forward to future constructive interactions
I can't see anything in Michael's comment about you being non-EA, have there been edits on the comment?
I don't think there have been any edits, and I'm sure Michael would identify them if he made any. I was trying to make my comment less personally-directed by broadening the scope (i.e not just talking about HLI and turning to a more general sentiment about input from 'anonymous' outsiders on this forum and how they might be perceived - I remain a bit confused about the 'real name' comment).
FWIW, I've had lots of positive interactions with EA members on this forum (in public and in private), even from such short-lived involvement, so it wasn't a chip-on-the-shoulder type statement. I mean no smear against EA as a whole. Thanks for prompting me to clarify.
Ah ok makes sense. I had read your comment as saying that Michael suggested you weren’t EA enough.
Oh gosh! Not at all, thanks so much for letting me know in that case - I'm sure others are reading it the same way if that was your interpretation.
I'm just being quite cautious in trying to not come across as some strangely specific and verbose troll with an HLI problem. My post wasn't about HLI and I found it difficult striking a balance to respond to that comment without seeming to make it about HLI i.e. perhaps there could be an interpretation I'm acting in bad faith (should that interpretation exist at all) not due to previous critique of HLI but my short history on this forum. I personally think that is a fair thing to find suspicious (!) and it's a reason I've felt there has been a higher burden on me vs established members in demonstrating I'm trying very hard to understand EA's philosophy and methods to allow a good faith interpretation vs providing lazy, half-baked criticism - I was trying to allude to this in the end of that comment and in my response to Ray below.
The culture is clearly a bit more challenging for me, and I'm often doing a few things at once when I'm online, so please continue to call me out if I risk being misunderstood.