Lack of access to family planning is a widespread problem with harmful consequences for health, economic well-being, and other outcomes. Despite its importance, it is comparatively neglected by EAs. Charity Entrepreneurship (CE) proposes to tackle this problem by launching a new nonprofit that would provide postpartum family planning counseling in priority countries. Contact us at ula@charityentrepreneurship.com if you’re interested in getting involved, or apply to our 2021 Incubation Program (deadline: April 15, 2021).
1. Why family planning?
Each year, over 300,000 women die from pregnancy-related causes. Maternal mortality is particularly high in sub-Saharan Africa, with two-thirds of all maternal deaths in 2015. A higher number of births per woman is also strongly associated with higher rates of child mortality. Short-spaced pregnancies, in particular, pose a greater risk to both mother and child.
There are over 120 million unintended pregnancies each year. Data from the UN shows that 10% of all women of reproductive age worldwide have unmet needs for family planning, meaning that although they do not want to fall pregnant, nor are they using contraception. Unmet family planning needs are particularly high in sub-Saharan Africa.
Health isn’t the only casualty of inadequate family planning. Lack of access to family planning impacts a whole range of outcomes, from education and economic wellbeing to climate change. The supplementary report for our cost-effectiveness analyses discusses these in more depth and explains how we modeled them. Depending on how you consider flow-through effects, we believe that this area could be as effective or more so than direct delivery health interventions.
Due to its importance, family planning receives a good amount of attention in terms of both research and availability of (often counterfactually strong) funding. However, it remains neglected in two important ways. Despite extensive research into the barriers to family planning, little prioritization work has been done. Additionally, family planning is a less common cause area of focus among applicants to the CE Incubation Program.
To address the lack of prioritization work, Charity Entrepreneurship has conducted hundreds of hours of research to compare interventions and identify the most impactful. Progressive stages of our extensive research process whittled down to two recommended charity ideas for family planning: mass media campaigns and postpartum family planning. These top ideas are highly cost-effective, with strong evidence of impact.
Prioritization is an important first step, but to realize the change we need implementation. In 2020, Kenneth Scheffler and Anna Christina Thorsheim launched Family Empowerment Media, working on mass media campaigns. They recently launched their proof of concept campaign with two radio stations in Kano State in Nigeria, and are reaching around 2.5-3 million beneficiaries. Through Charity Entrepreneurship’s 2021 Incubation Program, we hope to launch the second of our top family planning ideas – postpartum family planning.
2. Why postpartum family planning?
2.1 The intervention
The period up to ~24 months after a woman has given birth (i.e. the postpartum) is a crucial time for family planning. A new charity would help integrate family planning counseling services into postpartum care, providing training and support to health workers.
Becoming pregnant soon after giving birth risks the health of both mother and child, yet the data show that contraceptive use among postpartum women is lower than average. Contributing factors include misconceptions around how quickly a woman returns to fertility after giving birth and stigma surrounding contraception use. Compounding the issue, family planning is frequently not offered during postpartum care. Yet many women are only in contact with the healthcare system during pregnancy and delivery, which makes this a particularly good opportunity to discuss family planning options.
We estimate that each year, 23 million postpartum women in sub-Saharan Africa are not using contraception. Surveying 22 LMIC countries, Moore et al. (2015) found that over half of pregnancies occur at too-short intervals in 9 countries.
Conversations with experts and our survey of the evidence base (detailed below) highlighted that the immediate postpartum is the optimal time for family planning counseling. As an add-on, broaching the topic during antenatal care can ensure that a woman has the time to weigh her options and discuss her decision with her partner.
This intervention would be most effective in countries where contraception is available, but misinformation prevents uptake. Based on our analysis, Senegal and Ghana look to be particularly promising countries; Benin, Sierra Leone, and Cameroon also hold promise.
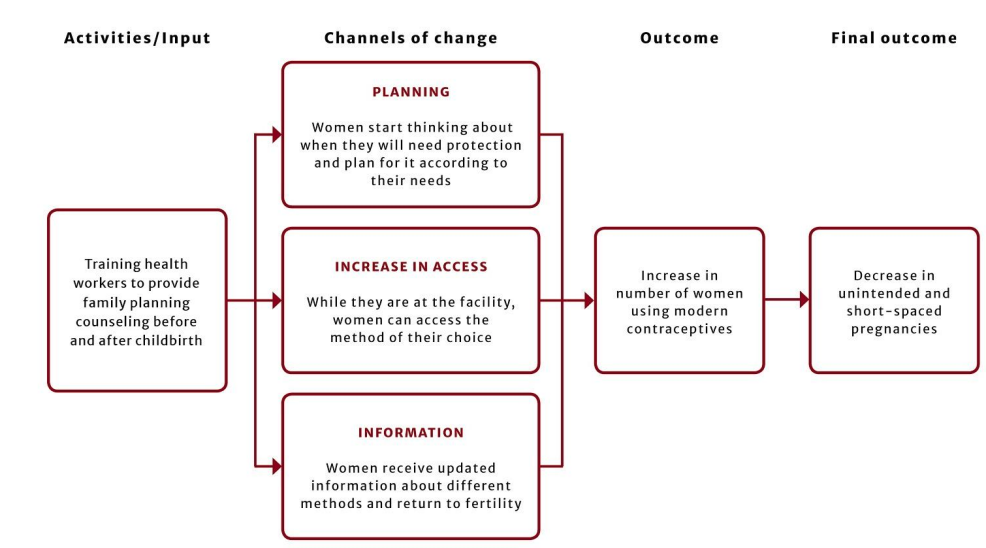
A new charity would begin by establishing relationships with local nonprofit and public actors. This would allow them to build their knowledge of the context and work on their proof of concept. Contextual knowledge is key to understanding the barriers to contraception uptake, so working with local stakeholders and being immersed in the context will be essential for a new charity. In the longer term, the charity would achieve scale by partnering with the local government.
Below is a theory of change for this new nonprofit:
2.2 Evidence & cost-effectiveness
This spreadsheet summarizes the nineteen studies on postpartum family planning, including eight RCTs and two systematic reviews. Find more discussion of the evidence of effectiveness for this intervention in section 5.3 of our report.
Based on the evidence, we estimate a 4.7 percentage point increase in uptake of contraceptives. This spreadsheet contains our cost-effectiveness analysis. The main impact we sought to capture was the cost per unintended birth averted: we found that postpartum family planning would cost as little as $67. We discuss why we chose to measure cost-effectiveness in unintended births in our supplementary report.
In addition to unintended births averted, we quantified cost-effectiveness in terms of DALYs, income effects, contraceptive uptake, CO2 emissions, and welfare points. We also calculated cost-effectiveness when including counterfactual considerations for donor funding, government resources, and the nonprofit’s co-founders. Based on our analysis, this intervention is cost-effective from multiple perspectives.
This overview table displays our cost-effectiveness estimates for the various factors we considered:
| Unit | $ cost per unit |
| Additional user of contraception | 39 |
| DALY averted | 984 |
| Unintended birth prevented | 67, or 144 if counterfactuals included |
| Tonnes of CO2 averted | 0.33 (3 tonnes per $ spent) |
| Welfare points | <0.003 (377 WP per $ spent) |
| Dollar generated in income benefits | <0.01 ($105 per $ spent) |
3. How you can help
We’re keen to connect with aspiring entrepreneurs, so if you know anyone who might be interested, please share this post. Further details about the Incubation Program can be found on our website (apply by April 15). Feel free to contact us for more information at ula@charityentrepreneurship.com.
Larks, as much as you consider the provided cost-benefit analysis to be "naive", I am afraid the same applies to several of the counter-points you mentioned. Could you please give some sources that support (a) your claims and (b) are broadly generalizable or generalizable to a degree they should support policy? Specifically, I think some of your assumptions you just take as given even though there is a lot of high-quality evidence to the contrary. I was also a bit disappointed that you did not want to answer on the below issues when you made that identical post the first time around. It seems to me like it is informed by an inherent pro-natalist view without the proper analysis of underlying issues and well-established complexities to the contrary. For the four bullet points in your post, I would like to provide counter-arguments (which I would be happy to discuss if you're interested) why they might not be correct and would greatly appreciate if you could provide generalizable evidence supporting your bullet points:
What is the EV here? Does this scale linearly with the amount of people that come into existence? Do you have any sources for the amount of "additional happiness" vs "additional suffering" caused by these humans to other life-forms (cf. average global meat and fish consumption)? There are various studies that basically say that the relation between "children" and "happiness" is complicated at the very least, for example seen in the following articles. All in all, happiness for parents mostly decreases while they actively rear children, for example:
This depends on the kind of growth and whether the government and economy of a country with a growing population can adequately supply all these points you mentioned. Many countries only experience a real bump in development due to the Demographic Dividend, i.e. when birth rates fall (s. for example Johns Hopkins University and Wikipedia). In many countries, unsustainable population growth depletes financial resources of governments and prevents long-term strategic investments by tying budgets to short-term social support. The same applies to families: Family income only increases with more family members once these new family members reach working age. Before that, they do not have more, but less money to spend on the individual, including education and training. In other words: Growth in population is not good for a country per se. It needs to be sustainable and supportable (by government and family budgets) for a country and its population to profit. Many countries such as Rwanda only really developed once they managed to profit from the Demographic Dividend, as established in countless peer-reviewed articles.
This only holds true if the society that grows can provide adequate education opportunities to support the specialization you mentioned. Good counter-examples to your argument are, in fact, the fastest-growing populations we know: Sub-Saharan countries. If your argument was generally true, countries such as South Sudan, Angola, Malawi, Burundi, Uganda, Niger, Burkina Faso and Mali should experience greater degrees of professional specialization. Do you have any evidence to support this? I would be very happy to see it!
Do you have any studies here that show the likelihood of people in the fastest-growing societies by birth numbers becoming inventors or scientists?
The scientific publication that has received the most supportive signatures from scientists ever, the World Scientists' Warning To Humanity, specifically urges world leaders to reduce human population growth. Quoting from Wikipedia which provides the primary source:
The Second Notice specifically states:
Do you think that this notice is generally biased or naive?