Note: This report was produced with only one week of desktop research, for the purpose of identifying promising causes to evaluate at depth. We only have low confidence in our findings here, and the conclusions should generally be taken by readers as merely suggestive rather determinative.
Summary
Taking into account the expected benefits of eliminating coronary heart disease (i.e. improved health and greater economic output), as well as the tractability of policy advocacy for mandatory trans fat limits, I find that the marginal expected value of policy advocacy for such mandatory trans fat limits to eliminate coronary heart disease to be 18,503 DALYs per USD 100,000, which is around 30x as cost-effective as giving to a GiveWell top charity (CEA).
Key Points
- Importance: This is a strongly important cause, with 1.81 * 1010 DALYs at stake from now to the indefinite future. Around 94% of the burden is health related, while 6% is economic in nature.
- Neglectedness: While 35.5% of the world population is already covered by trans fat bans, a lot more needs to be done, especially since the countries not covered (i.e. low and middle income countries) are the ones where we expect the greatest future increase in disease burden, as driven by various factors – from economic growth bringing about western pattern diets and physical inactivity, to population growth and ageing.
- Tractability: A moderately tractable solution is available, in the form of policy advocacy for mandatory trans fat limits. This is highly effective if and when implemented, and encouragingly many governments are already doing this, though of course the chances of success are always uncertain.
Caveats
- This report was produced with only one week of research, and critically, only desktop research was used, without experts consulted due to the lack of time. More research – at the intermediate stage and subsequently deep stage – will be needed before we can have high confidence in these findings.
- The headline cost-effectiveness will almost certainly fall if this cause area is subjected to deeper research: (a) this is empirically the case, from past experience; and (b) theoretically, we suffer from optimizer's curse (where causes appear better than the mean partly because they are genuinely more cost-effective but also partly because of random error favouring them, and when deeper research fixes the latter, the estimated cost-effectiveness falls). As it happens, CEARCH intends to perform deeper research in this area, given that the headline cost-effectiveness meets our threshold of 10x that of a GiveWell top charity.
Further Discussion
- After recent research and consideration, CEARCH has downgraded our views on the probability of advocacy success in general, though we are still bullish on global health policy interventions overall, and are looking to do more research in this area (e.g. diabetes mellitus type 2, hypertension, coronary heart disease).
- There are two different kinds of trans fat – industrial (i.e. that which is made in factories by adding hydrogen to vegetable oils) vs ruminant (i.e. what you find in beef and butter). There is strong evidence that industrial trans fat are bad for health, but the evidence on ruminant trans fat is mixed, and it is unclear if the lack of evidence is the result of ruminant trans fat being genuinely biochemically safer or if it is because the product tends to be consumed at lower quantities (such that health effects are harder to tease out in studies).
- Theoretically, a charity working on lobbying governments to improve their public health policy towards trans fats will be able to not just lobby for trans fat bans, but also other policies that help reduce coronary heart diseases (e.g. tobacco taxes or salt taxes); hence, the estimates here may be biased downwards
- When calculating the degree to which trans fat bans reduce trans fat consumption, we look at average global consumption – which factors in advanced economies, where trans fat bans are in place and consumption levels are lower). In contrast, the typical country that will be targeted by advocacy organizations will be low and middle income countries where there are no such bans and consumption levels are higher. Therefore, the estimates may be biased downwards in this respect as well.
- The modelling of how reduced trans fat consumption impacts the prevalence of coronary heart disease is fairly basic, and expert modelling on the matter will be desirable; this is something CEARCH expects to seek in deeper research stages.
- Other positive health impacts from reduced trans fat consumption are not modelled; this is potentially a significant underestimate that will be corrected for in deeper research stages.
- Trans fat bans are unlikely to make foods less tasty, since pure oil does not taste like anything at all.
- For the same reason, while freedom of choice is not modelled here, the issue is unlikely to be material – people can still eat what dishes they please; the removal of trans fats do not make food functionally any different, whether in terms of general ingredient classes, preparation techniques or (again) taste.
Expected Benefit: Improved Health from Eliminating Coronary Heart Disease
The primary expected benefit from eliminating coronary heart disease (also known as ischaemic heart disease, or coronary artery disease) is improved health, in terms of fewer deaths as well as less disability and suffering. Overall, around 1.71 * 1010 DALYs are at stake here. This benefit is modelled in the following way.
Moral Weights & Scale: The global disease burden of coronary heart disease is around 1.91 * 108 DALYs for the baseline year of 2024. This is calculated using a model that will be discussed in greater detail soon.
Persistence: The problem of coronary heart disease is likely to persist, and eliminating it will bring benefits not just for one year but across multiple years. In terms of how this multi-year benefit is calculated:
Firstly, I discount for the probability of the best solution not persisting – specifically, for the chance that a regulatory limit on trans fat is reversed (n.b. the choice of this solution will be discussed at length in the section on tractability). To calculate the rate of policy reversal on trans fat being limited by law, I take jurisdiction-years in which repeal occurred and divide by the jurisdiction-years (or at least a subset thereof that could be explicitly identified) in which the tax existed and repeal could have occurred (whether or not it did). This yields a reversal rate of around 0.4% per annum.
Secondly, I look at the proportion of the problem that will remain after counterfactual solution.
One aspect of this is factoring out the proportion of the global population already covered by trans fat bans. Currently, mandatory best-practice policies are in effect in 45 countries, covering around 2.8 billion people (35.5% of the global population), leading to a block discount of 35.5%.
The other aspect of this is modelling the proportion of the disease burden remaining after being counterfactually solved by other solutions beyond existing trans fat bans (i.e. CHD declining due to other interventions by other actors or else due to structural changes). To model such growth, I use the simple theoretical model that takes total DALYs lost to CHD to be a function of DALYs lost per capita and population size.
Note that whatever efforts that agents (i.e. governments, nonprofits and businesses) are making to solve the problem (e.g. taxing salt, increasing access to nitroglycerin at hospitals, voluntary food reformulation), and whatever impact that non-population structural trends are having (e.g. an ageing population increasing disease burden per capita given that the incidence of CHD is higher in older individuals; or economic growth involving greater access to western pattern diet foods as well as more physical inactivity; or improving education causing improved eating/exercise habits) all this will involve either increased (or decreased) prevalence rates of CHD or the disease burden per sufferer, and hence greater (or fewer) DALYs lost per capita; in short, the variable of DALYs lost per capita accounts for all these agentic and structural factors. The only exception, of course, is population size (where a larger population mechanically increases the disease burden for a given disease burden per capita), with that handled separately in this model. Note that we handle the trans fat issue separately due to the bans being fairly recent, and they may not have made much of an impact on the past disease burden with which we use to project future disease burden.
Overall, to model how the problem is expected to evolve over the years, I take the following steps. (a) Firstly, I project future DALYs lost per capita to CHD by estimating the year-on-year change via a linear regression of past DALYs lost per capita on discrete time. Projections are limited to 2100, with constancy assumed thereafter, as such projections will be unreliable in the far future. (b) Secondly, I use UN estimates of projected future population growth up to 2100 and then thereafter take that there is convergence to total fertility rate of 1.5 (given current high-income country fertility rates) and hence a -0.76% per annum decrease in population after 2100. (c) Thirdly, I multiply each future year's DALYs lost per capita and population size to obtain the expected total DALY burden for each year.
Note that the estimates here are consistent with expert modelling of future CHD prevalence rates, with Khan et al's statistical forecasting using 1990–2017 GBD data suggesting that the global ischemic heart disease prevalence rate could increase from 1,655 per 100,000 in 2020 to 1845 per 100,000 by 2030; such an increased prevalence rate (and hence an increased probability that any single individual will suffer IHD) supports the idea that DALYs lost per capita will increase in the future. Moreover, according to an earlier analysis of GBD data from 1990 to 2010, DALYs increased by 32.4% globally because of population ageing, and increased by 22.1% because of population growth - and given that population growth is expected to continue in the coming decades even as the world gets older, there is separately support for the idea that aggregate DALYs lost will increase going forward.
Finally, note that the increasingly large DALYs lost per capita, as projected up to 2100, are far from unrealistic - the 2100 figure, which is the highest, is still less than what middle income and high-middle income countries suffered on average as of 2019.
The projected growth of DALYS lost due to coronary heart disease up to 2100, after taking into account counterfactual solution (but absent trans fat bans), is shown in Diagram 1.
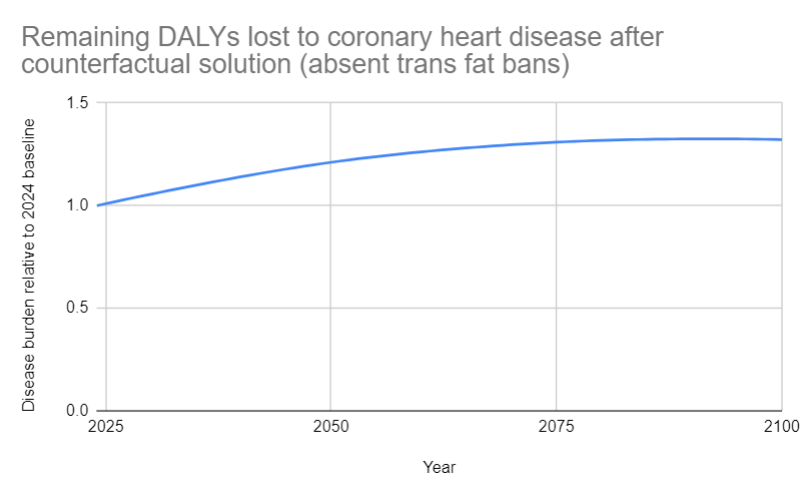
Diagram 1: Remaining DALYs lost to coronary heart disease after counterfactual solution (absent trans fat bans)
Thirdly, I discount for the probability of the world being destroyed anyway (i.e. general existential risk discount), which is around 0.07%. This takes into account the probability of extinction, since the benefits of saving people from coronary heart disease in one year is nullified if they would die in an extinction event anyway. For how this risk is calculated, refer to CEARCH's shallow research on nuclear war.
Fourthly, I apply a broad uncertainty discount of 0.1% per annum to take into account the fact that there is a non-zero chance that in the future, the benefits or costs do not persist for factors we do not and cannot identify in the present (e.g. actors directing resources to solve the problem when none are currently doing so).
Then, by taking the remaining DALYs lost to coronary heart disease after counterfactual solution (absent trans fat bans) and discounting each year's DALY burden using the other per annum discounts (i.e. solution reversal discount, existential risk discount, uncertainty discount), we can find the amount of DALYs relative to the baseline year available for policy advocacy for mandatory trans fat limits to counterfactually avert in each year (factoring out already existing trans fat bans).
Finally, by (a) summing the discounted per annum relative values for 2024-2100, and then (b) using a perpetual value formula for 2101 to infinity (assuming post-2100 population decline due to a long-term total fertility rate of 1.5), all the while (c) factoring out the impact of existing trans fat bans via a block discount, we see that the benefit of improved health from eliminating coronary heart disease (via trans fat bans) will last for the equivalent of 89 baseline years.
Value of Outcome: Overall, the raw value of improved health from eliminating coronary heart disease is 1.71 * 1010 DALYs.
Probability of Occurrence: There is no uncertainty here that coronary heart disease is an actual problem that harms people. As the Sanchar-Gomar et al 2016 review notes, although the trend has tended to reach a plateau since 1990, the overall mortality rates for CVD and CHD have fallen in most developed countries (by 24–50%) since 1975, with this (according to US data) being driven by improvements in therapy (50%), as well as changes in risk factors, including reductions in total cholesterol (24%), systolic blood pressure (20%), smoking (12%), and physical inactivity (5%). In contrast, in developing countries (e.g. China, India, sub-Saharan Africa, Latin America, and the Middle East), mortality from CHD was expected to increase from an estimated 9 million in 1990 to a projected 19 million by 2020. The upshot of this is that in both developed and developing countries, CHD as a problem has hardly been eliminated (despite some encouraging trends in rich countries), nor will it be by the baseline year of 2024 – hence, the probability that CHD is a problem can be assigned ~1.
Expected Value: Hence, the expected value of improved health from eliminating coronary heart disease is 1.71 * 1010 DALYs.
Expected Benefit: Increased Economic Output
Beyond the health benefits, there are also economic benefits to eliminating coronary heart disease. Around 9.95 * 108 DALYs are at stake here, as calculated in the following manner.
Moral Weights: I take the value of doubling consumption for one person for one year to be 0.21 DALYs. This is calculated as a function of (a) the value of consumption relative to life from GiveWell's IDinsight survey of the community perspective, as adjusted for social desirability bias, and (b) CEARCH's estimate of the value of a full, healthy life in DALY terms. For more details, refer to CEARCH's evaluative framework.
Scale: I start by calculating the economic burden of coronary heart disease relative to annual income per CHD sufferer, using three separate estimates to do so.
The first estimate is the American Heart Association's. I take the AHA's estimate of the total economic burden of cardiovascular disease in America in 2017 – factoring in both direct treatment costs (i.e. hospital inpatient stays, hospital ED visits, hospital outpatient or office-based provider visits, home health care, and prescribed medicines) as well as indirect productivity costs – and multiply this by the proportion of the total cardiovascular disease burden in the US that is specifically related to coronary heart disease. This is then divided by the number of CHD sufferers in America in 2017, to get the economic burden of CHD per sufferer. Dividing through by US GDP per capita in 2017 then gets the economic burden of coronary heart disease relative to annual income per CHD sufferer.
The second estimate is Leal et al's. I take the authors' estimate of the total economic burden of coronary heart disease in the EU in 2003 in euros – factoring in both the direct treatment costs (i.e. healthcare costs and informal care costs) as well as the indirect productivity costs – and translate it to USD. This is then divided by the number of CHD sufferers in the EU in 2003, to get the economic burden of CHD per sufferer. Dividing through by EU GDP per capita in 2003 then gets the economic burden of coronary heart disease relative to annual income per CHD sufferer.
The third estimate is Li et al's. I take the authors' estimate of the total economic burden of cardiovascular disease in China in 2003 – factoring in direct treatment costs (i.e. direct medical cost and direct nonmedical cost) but not indirect productivity costs – and multiply by the proportion of the total cardiovascular disease burden in China that is specifically related to coronary heart disease. This is then divided by the number of CHD sufferers in China in 2003 to yield the economic burden of CHD per sufferer. Dividing through by Chinese GDP per capita in 2003 then gets the economic burden of coronary heart disease relative to annual income per CHD sufferer.
I create a weighted average of these three estimates – penalizing Li et al's estimate due to it not taking into account indirect productivity costs – which yields an estimate of 25% of the economic burden of coronary heart disease relative to annual income per CHD sufferer. This is correspondingly also the degree of consumption doubling per coronary heart disease sufferer if their CHD is eliminated
At the same time, the total number of coronary heart disease sufferers in the baseline year of 2024 is around 217 million, as calculated using 2024 prevalence rate (predicted using the 2019 GBD baseline and projecting forward based on past growth trends) and 2024 population (drawing from UNPD projections).
Multiplying the degree of consumption doubling per coronary heart disease sufferer if their CHD is eliminated multiplied, by the total number of coronary heart disease sufferers as of 2024, yields an estimate of around 53.2 million consumption doublings achievable by eliminating coronary heart disease in the baseline year of 2024.
Persistence: The same per annum discounts, block discounts and projections of the disease burden (and hence economic burden) over time, as discussed in the previous section, are used here as well, such the benefit of increased economic output will similarly last for the equivalent of 89 baseline years.
Value of Outcome: Overall, the raw value of increased economic output is 9.95 * 108 DALYs.
Probability of Occurrence: Same probability as before is applied.
Expected Value: All in all, the expected value of increased economic output is 9.95 * 108 DALYs.
Tractability
To summarize our tractability findings: we can solve 0.0003 of the problem with a USD 28.1 million investment into policy advocacy for mandatory trans fat limits (factoring in the subsequent governmental costs of enforcement and private sector costs of supply chain restructuring), which means the proportion of the problem solved per additional USD 100,000 spent is around 0.000001.
In terms of eliminating the disease burden of CHD, we have the options of prevention vs treatment – preventing the disease from occuring at all, on the one hand, and treating it such that the disease does not burden its sufferers, on the other. There are strong theoretical reasons to favour treatment: the health burden (and hence economic burden it causes) will be higher under treatment vs prevention, given that treatment may not start simultaneously with the onset of the disease and given that treatment may not fully eliminate the disease burden. Moreover, based on expert interviews on the topic of NCDs (e.g. hypertension and diabetes), it does seem that experts do recommend prevention over treatment.
The challenge, then, is identifying which risk factor it would be best to target to reduce the disease burden of CHD. To do this, I use the GBD to identify the biggest risk factors in terms of DALYs lost to CHD per capita. The top three risks are, in descending order, high blood pressure (1285 DALYs lost per 100000 people), high LDL cholesterol (1097 DALYs lost per 100,000 people) and smoking (562 DALYs lost per 100,000 people). At the same time, I look at the chances of success in making headway eliminating these risks. Policy advocacy for sodium taxation to reduce high blood pressure has perhaps a 13% chance of success, according to previous analysis by CEARCH. Meanwhile, policy advocacy for mandatory trans fat limits (which raises LDL levels even while lowering HDL levels) has maybe a 38% chance of success. As of 2022, 45 countries have seen implemented mandatory best-practice policies on trans fat, and so, logically, they would have experienced at least an internal advocacy campaign to ban trans fat (i.e. someone advocating from within government to alter the status quo); this provides the minimum potential number of countries that have experienced lobbying to impose mandatory limits on trans fat. Meanwhile, there are 193 countries; and that provides the theoretical maximum number of countries that have experienced lobbying on the imposition of mandatory trans fat limits. Hence, in terms of the potential number of lobbying attempts we have min = 45/193 and max 193/193. Assuming that each number of lobbying attempts has equal probability of being the true number (i.e. the PDF is flat), this translates to 119 lobbying attempts, and hence a success rate of 45/119 or around 38%. And finally, tobacco taxation has perhaps a 27% chance of success, according to previous case study analysis by Charity Entrepreneurship. Multiplying impact (if the risk factor is eliminated), with the probability of success, this yields roughly 167 DALYs for sodium taxation advocacy, 417 DALYs for mandatory trans fat limits advocacy, and 152 DALYs for tobacco taxation advocacy. This analysis is very rough, but I use this to prioritize and identify a potentially best solution – which turns out to be policy advocacy for mandatory trans fat limits.
In terms of our theory of change:
- Step 1: Lobby a government a government to impose mandatory trans fat limits;
- Step 2: Mandatory trans fat limits reduce trans fat consumption
- Step 3: Reduced trans fat consumption reduces the remaining global burden of coronary heart disease
Step 1: To estimate the probability of successfully lobbying a government to impose mandatory trans fat limits, I take both an outside and inside view.
For the outside view, I consult three reference classes.
The first reference class is simply the success rate of previous attempts to impose mandatory trans fat limits – as calculated by the previous analysis used to do our initial prioritization.
The second reference class is the success rate of previous attempts to raise taxes on sugar-sweetened beverages – which is relevant to the extent that this is another health policy intervention that involves lobbying governments to regulate food.
The third reference class is the success rate of general lobbying attempts in the US/EU/China – after all, the base rate of success in lobbying should inform our estimate of the rate in specific cases.
Aggregating these three reference classes, I use the following weighting scheme. The three reference classes – (a) mandatory trans fat limit advocacy, (b) SSB taxation advocacy, and (c) general lobbying – have decreasing relevance, and I penalize them accordingly. However, the trans fat ban reference class is highly unreliable, based as it is on a fairly theoretical extrapolation of the number of lobbying attempts. Meanwhile, the SSB taxation reference class faces serious worries about selection bias – the jurisdictions that even see attempts to implement such taxes will doubtlessly have a higher baseline level of support for such taxes (such that health advocates see that they have a reasonable chance of success and will even make the attempt in the first place. Taking both relevance as well quality issues into consideration, I ultimately decide in favour of equal weights, yielding an outside view estimate of 53% probability of lobbying success.
For the inside view, I reason as follows. Policy advocacy is fundamentally difficult, so a reasonable starting point would be to assign a <=10% chance of success. That said, many countries already do impose bans on trans fats, which suggests that such bans are politically feasible and that successful advocacy is not extremely improbable (i.e. <=1%) – perhaps further calibrating to 10% seems reasonable. However, enforcement seems to be a challenge, at least in LMICs (n.b. the main challenge of enforcing trans fat regulation is laboratory capacity to allow the testing of goods for trans fat and hence the subsequent use of penalties/sanctions/administrative measures against errant manufacturers or importers) - hence, I adjust the probability downwards, to perhaps a 9% chance that advocacy efforts are successful.
When aggregating the outside and inside views, we have to note that while the inside view is subject to the usual worries about inferential uncertainties, the outside view is also considerably flawed in this case (i.e. the trans fat ban reference class relying on theoretical extrapolations; the SSB taxation being both somewhat less relevant as well as subject to selection bias concerns; and the general lobbying reference class being much less relevant). Hence, equal weightage is used, yielding an aggregate estimate of 31% probability of lobbying success.
Step 2: To estimate the degree to which mandatory trans fat limits reduce trans fat consumption, I use an empirical estimate. Given mean global intake of trans fat at 1.4% of total energy intake, and given that the Danish ban decreased trans fat consumption from 1.5g per day to virtually nothing (i.e. 100% reduction), I take that the typical ban will reduce trans fat consumption by 1.4% of total energy intake.
Step 3: To estimate the degree to which reduced trans fat consumption of 1% reduces the remaining global burden of coronary heart disease, I again look for an empirical estimate. De Souza et al's systematic review and meta-analysis of observational studies finds that highest vs lowest levels of intake of trans fat is associated with increased CHD at a relative risk ratio of 1.21 (p <0.001) – which translates to a 2% increase in energy from trans fat being associated with a 25% increased risk of CHD, a finding consistent with conclusions from two previous meta-analysis. This increased relative risk of CHD caused by trans fat consumption can – in conjunction with data on current prevalence, incidence and average duration of CHD – be used to calculate the degree to which prevalence of CHD will fall for a given decrease in trans fat consumption. For more details, refer to Annex C in the cost-effectiveness analysis. Per these calculations, the relative reduction in prevalence of coronary heart disease given reduction in trans fat consumption (by 1% of total energy intake) is around 9.8%. Given 148 countries still being uncovered by mandatory trans fat bans, a 1% reduction in trans fat consumption relative to total energy intake in an average remaining country will reduce the remaining absolute global prevalence of coronary heart disease and hence the concomitant remaining disease burden by 0.07%
Overall, the proportion of disease reduction from policy advocacy for mandatory trans fat limits to eliminate coronary heart disease – as a function of (a) the probability of successfully lobbying a government to impose mandatory trans fat limits; (b) the degree to which mandatory trans fat limits reduce trans fat consumption; and (c) the degree to which reduced trans fat consumption of 1% reduces the remaining global burden of coronary heart disease – is ultimately 0.0003.
Meanwhile, on the costing side, we have to be concerned with three things: (i) the cost of advocacy (for a nonprofit working on the matter); (ii) the cost of enforcement (for the government); and also (iii) the cost to the private sector in terms of supply chain reformulation (i.e. food reformulation etc).
To estimate the cost of advocacy, I consider two reference classes – an existing charity and a hypothetical Charity Entrepreneurship incubated charity. For the former, I look at Resolve to Save Lives, which seems the premier organization working in this area; they are partnering directly with the WHO to develop and launch REPLACE, an initiative to eliminate artificial trans fat from the global food supply. I assess that around 1 year of operations is a reasonable timeframe for the charity to do geographic selection, subsequent in-country preparatory activities (e.g. prepare supporting research reports on the economic and health benefits of the policy, conducting public polling to show public support, construct a coalition of NGOs and advocates, convince past and present politicians to be legislative champions) and to actually lobby the sitting government - and hence succeed (in which case it can pivot to a different country) or judge that policymakers are just not receptive and that its efforts have failed (in which case it can pivot or else shutdown). For the hypothetical CE incubatee, the typical structure is that of 2 co-founders, with funding of around USD 50,000 per person per annum. As before, I take a year to be a reasonable timeframe for either identifiable success or failure. In aggregating the two estimates to come up with a weighted average, I take into account the following considerations. On the one hand, (a) the existing organization's financial track record generally gives a much better indication of baseline expenditure requirements in the cause area, and (b) ensuring that countries have the laboratory capacity to enforce bans seems key, and that in turn may require the charity to fund testing if poorer governments lack the capacity, making a larger budget pro tanto more necessary. On the other hand, (c) Resolve to Save Lives's work (and hence budget) covers other areas aside from trans fat, and in any case, (d) the explicitly EA-aligned CE-incubatee will almost certainly be more cost-effective. Hence, I ultimately use equal weightage, which yields a cost of advocacy per annum of around USD 357,000.
As for the cost of enforcement – this is about USD 19.8 million, as calculated through the following process:
As for the cost of supply chain restructuring – this is about USD 7.92 million, as calculated through the following process:
- Look at estimates of the aggregate cost of complying with a trans fat ban in the US, with this taking into consideration manufacturer reformulation (3 billion, one-time), relabelling (37 million, one-time), substitute ingredients (250 million per annum) and restaurant reformulation (570 million, one time), and divide through with US population in 2015 to get the relevant per capita costs.
- Apply the same steps as described in estimating the cost of enforcement (i.e. factoring in intervention country's population size, equivalent baseline years in which supply chain restructuring occurs, probability of advocacy success, and lower counterfactual value of non-EA financing) to both the one-time and ongoing costs here.
The total cost of intervention comes up to about USD 28.1 million.
Consequently, the proportion of the problem solved per additional USD 100,000 spent is around 0.000001.
Marginal Expected Value of Policy Advocacy for Mandatory Trans Fat Limits to Eliminate Coronary Heart Disease
All in all, the marginal expected value of policy advocacy for mandatory trans fat limits to eliminate coronary heart disease is 18,503 DALYs per USD 100,000 spent, making this around 30x as cost-effective as a GiveWell top charity.


Hi Joel,
I would be curious to know CEARCH's take on the meat-eater problem. For the 35.07 G poultry birds and 7.84 G humans in 2020, and Rethink Priorities' median moral weight of 0.332 chickens, one can conclude the total moral weight of chickens is 1.49 (= 35.07*0.332/7.84) times that of humans. So extending the life of humans may be net negative in the nearterm.
In any case, considering the impact on wild arthropods is pretty uncertain (quick illustration here), and may well be more important than the impact on chickens (see here), I would say the impact of life extension in the nearterm is pretty uncertain too.
Personally, I would like to see analyses looking into the longterm effects of life extension, along these lines.
Hi Vasco - this is something I've thought a lot about! My rough answer is that, having done some BOTECs myself, I do think that saving lives is net positive. Note that you can't just take the RP figures and use them like this (i.e. comparing moral weight of humans x no. of humans, vs moral weight of chickens vs no. of chickens), since the RP weights only look at peak intensity, and doesn't factor in the degree to which that peak is reached, or for how long - nor does it take into account non-experiential goods (e.g. life per se, or liberty, or achievement, or love etc). If you factor all this in, (probably) saving lives isn't net negative - but it's very subjective, since obviously we can't really measure the qualitative experience of animals and have to extrapolate/guess.
Thanks for the reply!
Nice, I think it would maybe be worth including in the post something about that, as it could change the results significantly.
Thanks for clarifying. Intuitively, factory-farmed animals have more intense experiences (relative to their moral weight / peak welfare capacity), so I think accounting for intensity would make saving lives even more negative than my BOTEC suggested. Moreover, in general, I would claim non-experiential goods tend to be correlated with experiential ones, so I do not think accounting for them would favour saving human lives (also, factory-farmed animals have little liberty and achievement, and die more often). In any case, all goods are experiential in the sense words like "life per se, or liberty, or achievement, or love etc" refer to subsets of experiences.
Have you considered the effects on wild (terresthrial and marine) arthropods and nematodes (due to deforestation, fishing, and global warming)? Accounting for these, I think the sign of the expected value will be quite uncertain... We may conclude that our best guess for it is negative/positive, but that would not offer a strong basis for action. If there is lots of uncertainty, I think it makes more sense to say that we do not know, and carry out more research to increase the resilience of our estimates.