Just one comment: the essay asks "Why doesn’t the Gates foundation just close the funding gap of AMF and SCI?" but doesn't seem to offer an answer. The closest seems to be 3b/c which suggests it's a coordination problem or donor's dilemma: everyone is expecting everyone else to fund these organizations.
If that's the case, the relevant question would seem to be: what does the Gates foundation want? If the EA community finds something that GF wants that we can potentially offer (such as new high-risk high-return charities doing something totally innovative), then we can potentially do a moral trade with them.
Wow, great write up. Would be a good post for GWWC. I'd heard through the grapevine (I work at an organization funded by Gates) that they are having trouble giving away all of their money to good causes and are not giving it away fast enough. It seems most of the reasons given here involve resource constraints that it's not clear to me they are in practical terms.
Looks like a very in-depth analysis, congratulations. What I've read so far has effectively reassured me that room for more funding isn't ultimately a worry here and that global health is an excellent cause taking it into account. Do link to the final Giving What We Can blog version here, though I imagine most of us who are interested will spot it there and in the newsletter.
AI Use Note: Main body text entirely human written. Claude (Opus 4.8) helped develop models of animal life histories in the appendix.
Cross-posted from Good Structures.
Executive Summary
* Animal advocates sometimes make claims like “there are X of this animal...
“How long have you been v*g*n?”
This is one of the most common icebreakers at animal protection events. It’s a baseline assumption, and it mostly holds true: if you’re out advocating for animals not to be tortured or abused, realistically these days you are v**n, or close. And it makes for good conversation. It seems fairly safe to assume when you meet strangers.
But this assumption is hurting the movement in a way which we don’t always notice: someone new comes into the sp...
Summary
Back in November 2023 I posted here to launch Spiro and raise our first $198k. Two and a half years later this is an update and a fundraiser for the next step.
The short version: we've now reached over-5,900 people with TB preventive medicine, including over 3,000 children under five years old. Our early results have held up well an...
Disclaimer: This is my personal opinion and does not reflect the opinions of Giving What We Can or any particular other organisation.
Erratum: A previous version of this document falsely stated that Givewell.org based their room for more funding analysis on certain considerations. In fact, I merely speculated that big funding bodies might base their funding these considerations.
Some people might wonder why the big foundations such as the Gates Foundation, or overseas development assistance budgets of western countries could not just fund every very effective health intervention that are currently recommended in the effective altruism space.
People might also think that all effective causes might be fully funded within say 5 years (with the exception of GiveDirectly, which is very scalable).
For instance, in a debate[1] on whether a recent $400 million dollar donation to Harvard University should rather have gone to charities such as the Against Malaria Foundation and the Schistosomiasis Control Initiative, it has been argued that “there is no way[emphasis mine] that [very effective charities, such as the Against Malaria Foundation] could absorb that kind of cash when its annual operating budget hovers around $3.5 million”[2].
Another example, is someone recently stating that “The charities most supported by effective altruists target low-hanging fruit in global health. [...] When the few top-rated health charities reach funding capacity, where do we turn? Direct giving or more mediated approaches?”[3]
I think this is a misconception and it’s highly unlikely that effective global health / poverty charities will be overfunded very soon. In other words, people who think that we won't really know where we should put our money after just a few million dollars, should not be worried. If we were to move significantly more money, we would probably would find other giving opportunities.
Before we discuss why this is, we first need to answer a different question.
Why are some room for more funding estimates only in the low millions, while others are in the billions?
Some room for more funding projections, which are in the low millions, could maybe be more fittingly described as short-term room for more funding projections for a particular charity. These projections differ from long-term room for more funding projections for the overall area such as neglected tropical diseases, malaria, or micronutrient fortification, which are in the billions of dollars (see appendix). Some people may be confused when they see short-term room for more funding projections and see how they differ from long-term room for more funding projects. Concretely, the Against Malaria Foundation and the Schistosomiasis Control Initiative only have room for more funding in the tens of millions in the short-term, and would certainly have some trouble spending their resources, if they were to each receive $100 million tomorrow. However, that does not mean that they could not significantly scale-up in the next few years or that generally the funding gap for the distribution of bednets generally is only in the tens of millions. Bigger organisations such as UNICEF or the END fund could probably spent that much money on very effective interventions very quickly- I will return to that point in the conclusion.
There are some good reasons for why large donors would want to not give too much money to a charity at once:
Avoiding excessive reserves: Because of the opportunity costs (other charities could use money productively sooner), it is undesirable to have a charity having excessive reserves. Ideally, they would be promised a steady stream of funding if they meet specific targets over many years in order for them to be able to plan ahead.
Risk diversification: Funds should be distributed to several high impact organisations in order to diversify the risk of one of them not performing well.
Incentivizing others to join the cause area:
Countries: By restricting funding to a particular country, one incentivizes the country to invest in very effective health interventions themselves and use their (often very limited) domestic resources to close the funding gap between donations and the full cost of delivering effective health interventions. Poorer, low-income countries (such as Ethiopia) are less able to do this than low-to-middle income countries (such as India).
Charities: By restricting funding to charities, they’re being kept on their toes, so that they do not rely on a particular foundation or big grant giver exclusively and apply for other grants. For instance, in the past, the Gates foundation has heavily funded the Schistosomiasis Control Initiative. However, Gates later discontinued SCI’s funding not because of too little effectiveness, but because, since their effectiveness had been established, other funders would more readily fund them.
Other donors: By restricting funding to particular charities, other donors are incentivized to also invest in the effective charities. For instance, the Against Malaria foundation has a broader appeal to small private donors than more high-expected-value interventions. Thus, even though theoretically, the Gates foundation, which is the largest private foundation in the world with an endowment of US$42.9 billion[4], could buy every person in Africa a bednet every two years (population of Africa (1 Billion) * Cost of Bednet (5 Dollars) = 5 Billion dollars) that would rapidly deplete their limited resources and then they could not spend their money on other very effective causes. They might reason that (small) more risk-averse donors (who want to be certain that their money will have an impact) will close the funding gap of very effective and established interventions and that they can instead spend more money on riskier, high expected value areas.
Technological Innovation: New technological innovations—such as a very effective malaria vaccine—might be discovered, and these might be more cost-effective.
High risk, high reward project:
For these reasons, one needs to come up with short-term room for more funding estimates.
Crucially, many room-for-more-funding numbers do not include scale-up and seem to be an estimate of how much money the charities can use to fund projects in the short-term (i.e. in the next couple of years). In other words, these estimates do not take into account potential mid-term scale-up of their interventions into other countries or into more projects (see for instance[5],[6]). For instance, Givewell reports that AMF’s room for more funding in the next year is $25 Million, which translates to roughly 5 million bednets. Because AMF has reported to be constricted in terms of funding in the short-term, they had not been actively reaching out to other countries to discuss new net programs in the beginning of 2015[7]. AMF also has more leverage with regards to national malaria control programs agreeing to implement their strict and rigid monitoring and evaluation process, when they agree to give governments millions as opposed to thousands of bednets[8].
Because these room for more funding estimates do not include scale up, the Gates foundation cannot simply close the funding gap for bednets.
How much can be spent on very effective causes?
Some room for more funding estimates do not account for potential scale-ups of a charity’s operations. For instance, one might estimate that SCI's funding gap is in the low millions this year. However, SCI could intensify their efforts of existing projects, expand to other countries, and be only marginally less effective. They have in the past successfully absorbed $30 mil Gates grant[9] and if we gave them another X million dollars, they might be able to deworm another country or make their existing deworming programmes better.
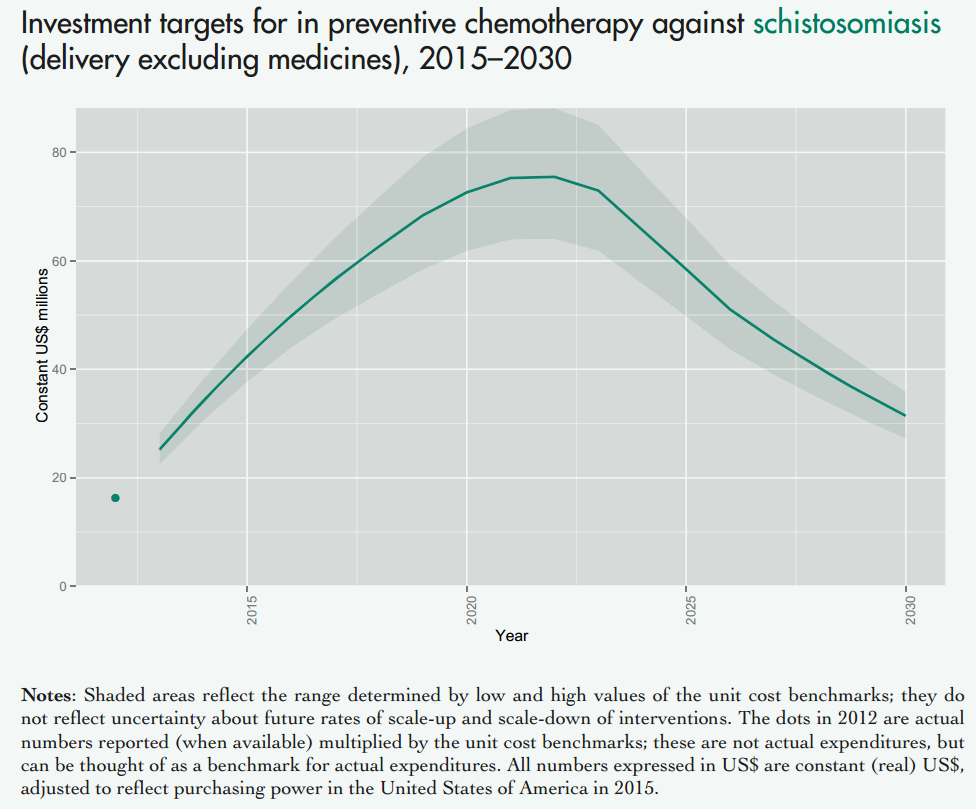
Take a look at the following graphs to get an idea of the scale for how much money could be spent on mass drug administration (preventive chemotherapy) against Schistosomiasis:
Figure showing investment targets for preventive chemotherapy against schistosomiasis (in million constant (real) 2015 US$ adjusted to reflect purchasing power in the United States). This excludes medicine prices, which are donated by the pharmaceutical companies. Figure adapted from (Fig. 2.4 Investment targets for universal coverage against Neglected Tropical Diseases (NTDs) from recent WHO report[10] on NTDs).
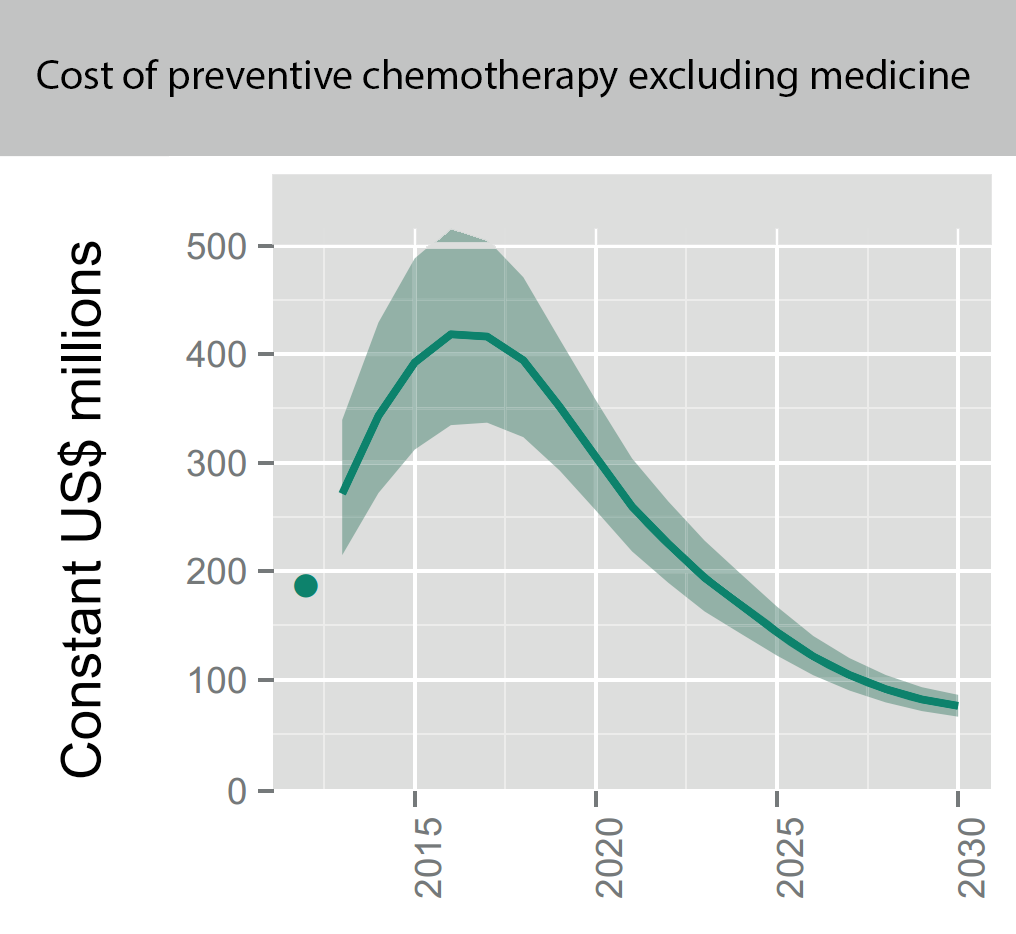
As you can see this is in the tens of millions every year (for comparison, Givewell moves around 6 million a year to SCI). But this is just schistosomiasis. The cost for all mass drug administration against all NTDs (such as Soil transmitted Helminths) cost even more:
Figure showing the overall projected costs (in million constant (real) 2015 US$ adjusted to reflect purchasing power in the United States) of all preventive chemotherapy (i.e. mass drug administration against NTDs including schistosomiasis and soil transmitted helminths, but not malaria) for the coming years. This excludes medicine prices, which are donated by the pharmaceutical companies. Figure adapted from (Fig. 2.4 Investment targets for universal coverage against NTDs from recent WHO report[11] on NTDs).
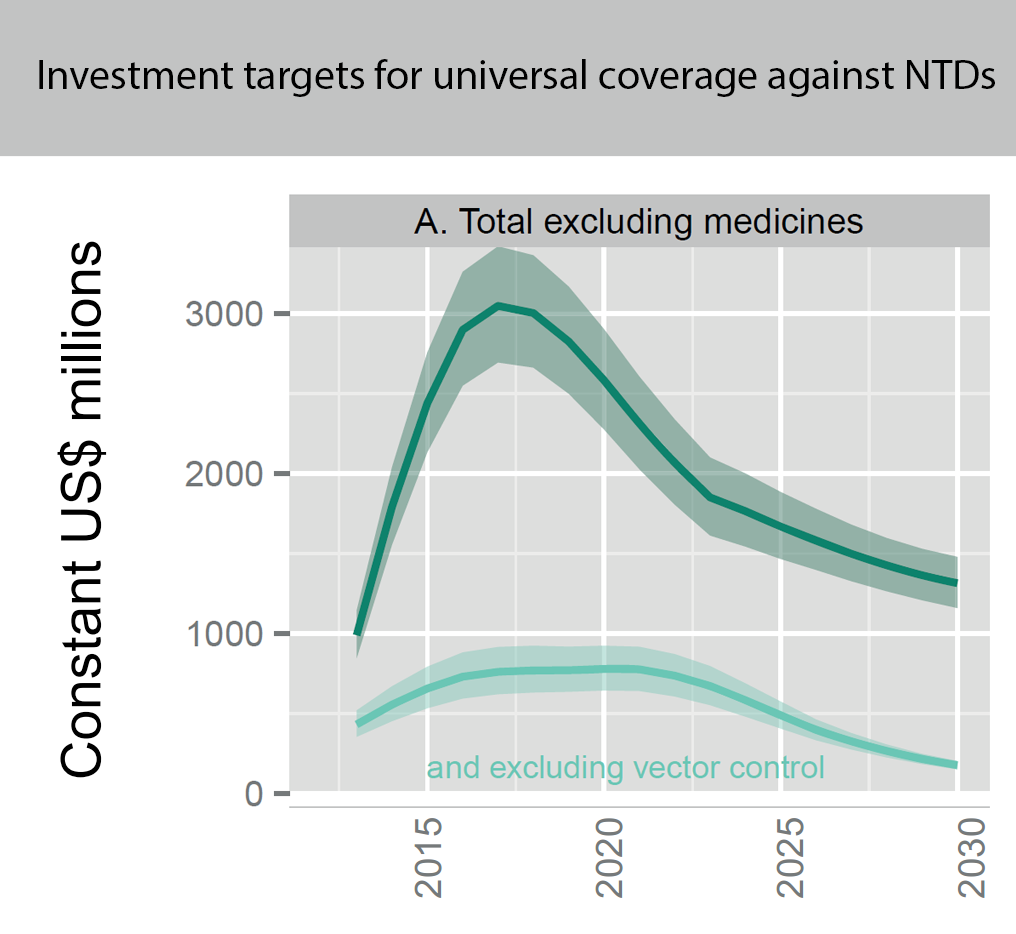
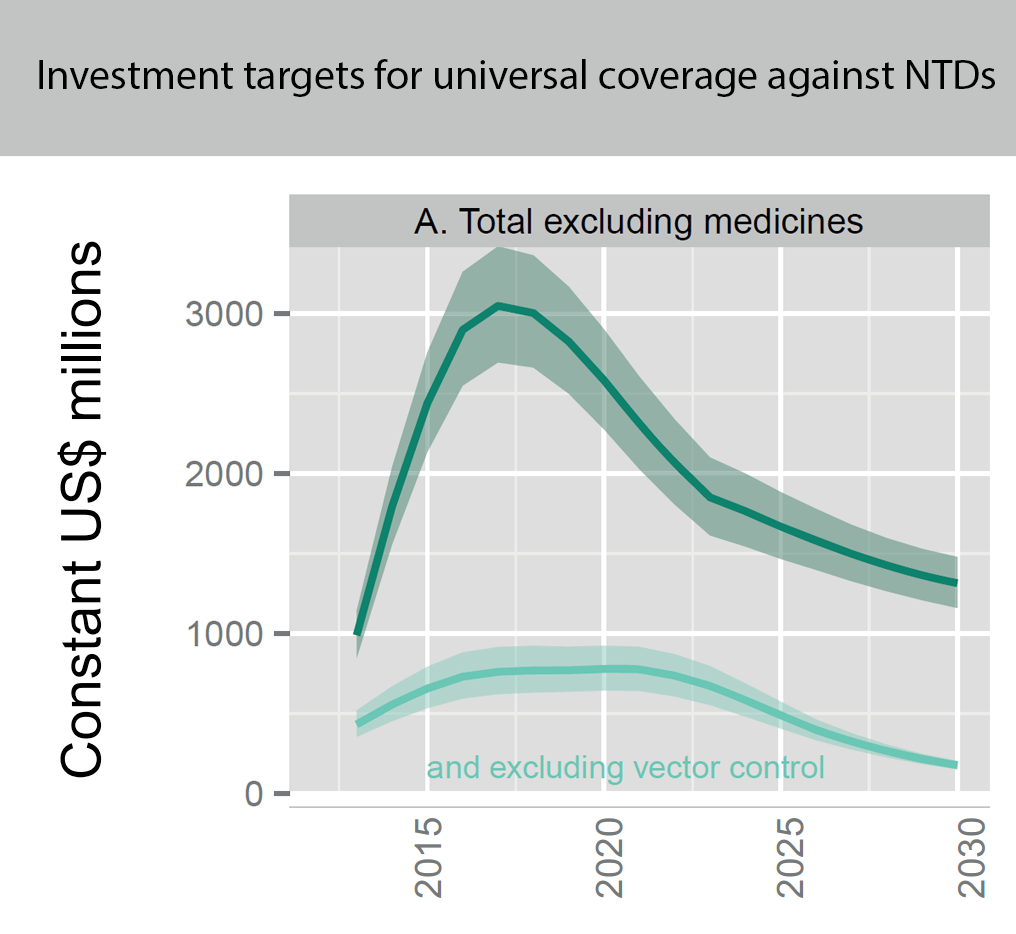
And providing universal coverage for all neglected tropical diseases will cost hundreds of millions (or even billions if you include vector control) every year:
Figure showing the overall projected costs (in million constant (real) 2015 US$ adjusted to reflect purchasing power in the United States) of all preventive chemotherapy for universal coverage against NTDs (such as schistosomiasis and soil transmitted helminths, but not malaria) for the coming years. This excludes medicine prices, which are donated by the pharmaceutical companies. Figure adapted from (Fig. 2.4 Investment targets for universal coverage against NTDs from recent WHO report[12] on NTDs).
I’m listing costs for some other diseases in an appendix below.
Where should effective altruists spend their money?
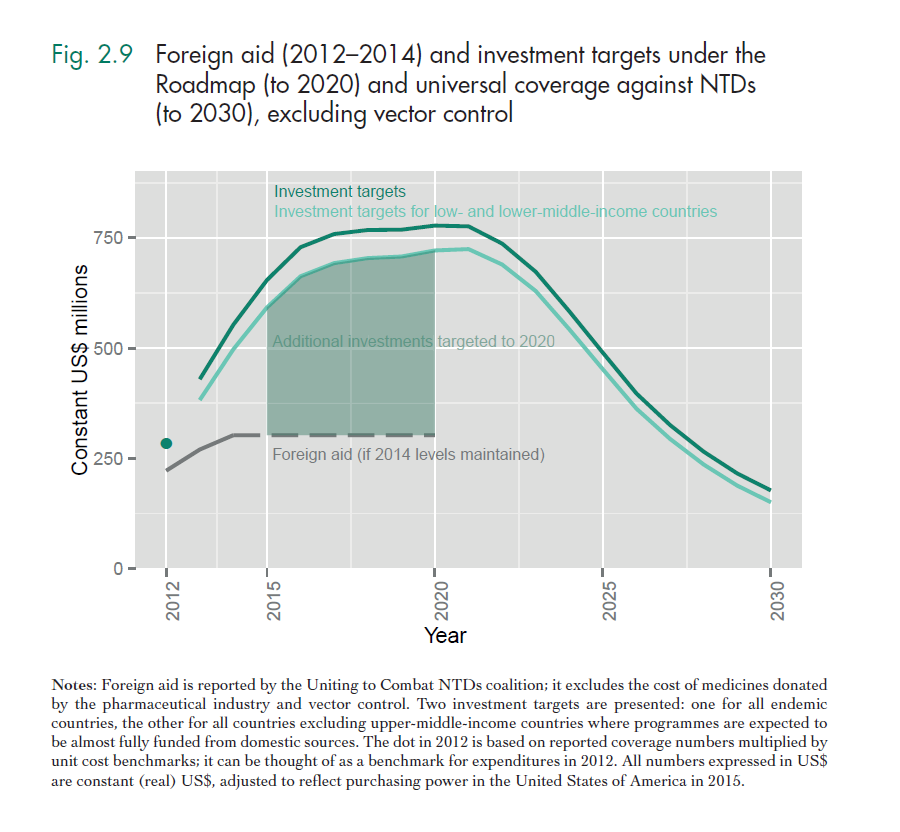
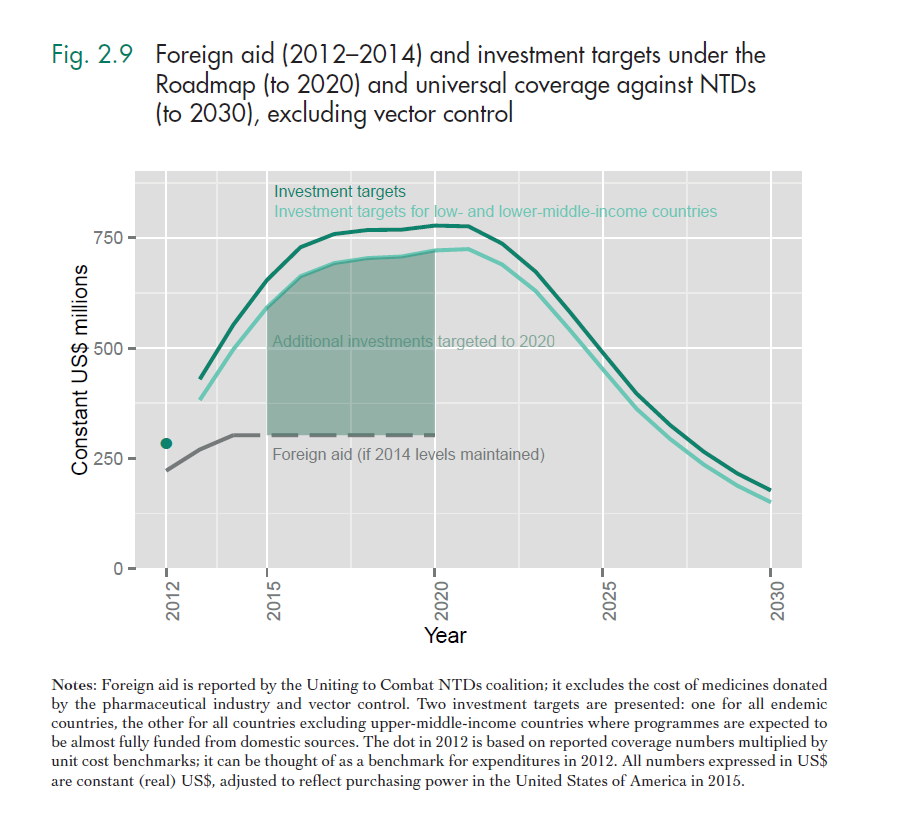
If we were to spend all the money we need to for universal coverage against certain NTDs we’d discourage others from funding NTDs (both domestic and western donors). A recent WHO report[13],[14], has a better estimate of the true funding gap for neglected tropical diseases, which I define as what would not be funded if we don’t fund it. This takes into account that the high costs for universal coverage against NTDs as shown above will be covered to a large extent by domestic funds from lower-middle income countries. Lower-middle income countries such as India often just need technical assistance. In contrast, lower income countries cannot fund mass drug administrations, bednet distributions etc. themselves at all, because they're too poor and it is politically not feasible to spend massively on poor rural populations. Even taking this and increasing western aid budgets into account there's a big funding gap. Nobody knows where the money needed to achieve somewhat universal coverage from NTDs is supposed to come from.
The WHO writes:
“The commitment of foreign donors and community volunteers to NTD control will continue to be important in scaling up access to those products that are available. However, it is unlikely that they can mobilize resources at the scale implied by universal coverage against NTDs. Universal coverage against NTDs will fail if it fails to mobilize domestic investment.” It is unclear whether poorer countries will be able or whether it will be politically feasible to mobilize sufficient domestic investment to close the funding gap.
The funding gap that you see in green above is thea better approximation of the real funding gap that could be closed by effective altruists, which is in the hundreds of millions. The counterfactual here would be that this funding gap would not be closed even if foreign aid increases above 2014 levels. Narrowing in on this target will obviously lead to decreased effectiveness (for instance, a key driver of cost-effectiveness of bednet distributions and mass deworming is disease prevalence). It is difficult to estimate when an intervention becomes much less cost-effective. However, it seems as if there is ample room for more funding before we hit those diminishing marginal returns on investment.
Of course, the Schistosomiasis Control Initiative might be overwhelmed by spending so much more money and we would probably have to find bigger organisations in the schistosomiasis space, such as the END fund, UNICEF, who could absorb more money for effective NTD interventions (I return to this point in the conclusion).
What happens after universal coverage against neglected tropical diseases and Malaria?
After moving many more millions to Malaria and Deworming charities, and establishing universal coverage against Malaria and NTDs (some of which are probably not much more ineffective to treat than schistosomiasis), there are many more very effective health interventions that one could fund.
Here are just some random examples of health interventions whose cost-effectiveness estimations might be somewhat off and potentially worse, but that are probably still very effective:
Antenatal syphilis screening: $50 per DALY averted[15]
Introduction of auto-disable syringe that cannot be reused and reduces needle sharing: $46-48 per disability adjusted life year (DALY) averted[16]
Female condom distribution programmes in Zimbabwe: US$146 per DALY averted[17]
There are many more examples such as these and it will take quite a long time to fund them.
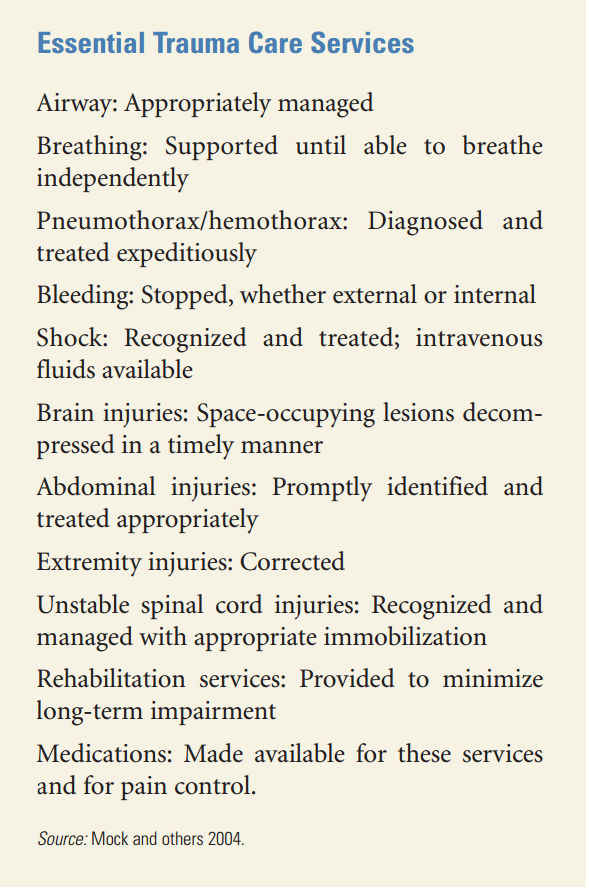
But even after such ‘distribution of stuff’ health interventions are funded there are some incredibly effective health interventions to fund. For example, take a look at the recent DCP report on ‘trauma care hospitals[18], which provide very basic treatment:
Medecins Sans Frontieres could help with setting up such hospitals in developing countries. And such hospitals are very effective:
"A subsequent study in a pure trauma first-level hospital in Cambodia found a cost-effectiveness of US$78 per DALY averted (Gosselin and Heitto 2008). Another study comparing two Médecins Sans Frontières trauma hospitals in Haiti and Nigeria found a cost-effectiveness ratio of US$223 and US$172 per DALY averted, respectively,"[20],[21]
Another study suggests that providing essential surgeries can cost as little as $33 per surgical DALY averted in sub-Saharan Africa[22].
This might be an underestimate, but it is very likely that it is not very far off: hospitals are pretty good at estimating DALYs averted, because a patient comes in with a medical problem, say appendicitis, if it’s diagnosed, you know the associated burden, you treat the patient, and you know how much it costs. In comparison, Givewell estimates that combination deworming is $72 per DALY (disability- adjusted life year) averted (note that Givewell’s estimates typically have a lot more conservatism applied).
In sum, one may guesstimate that the room for funding for very effective health interventions (<$1000 per DALY averted) is at least in the hundreds of billions per year (for sub-Saharan Africa, spending only $86 per capita already comes to about $80 billion USD).
Who else could close the funding gap?
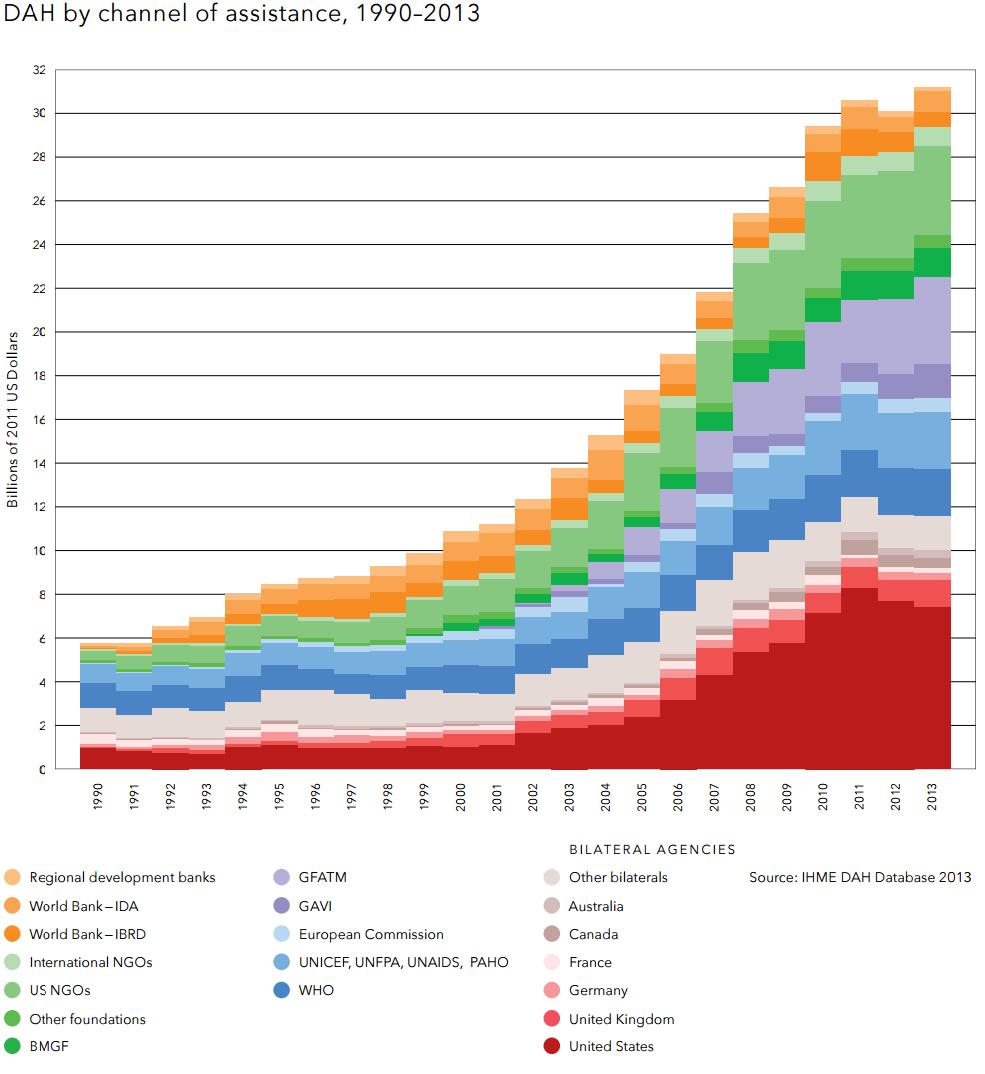
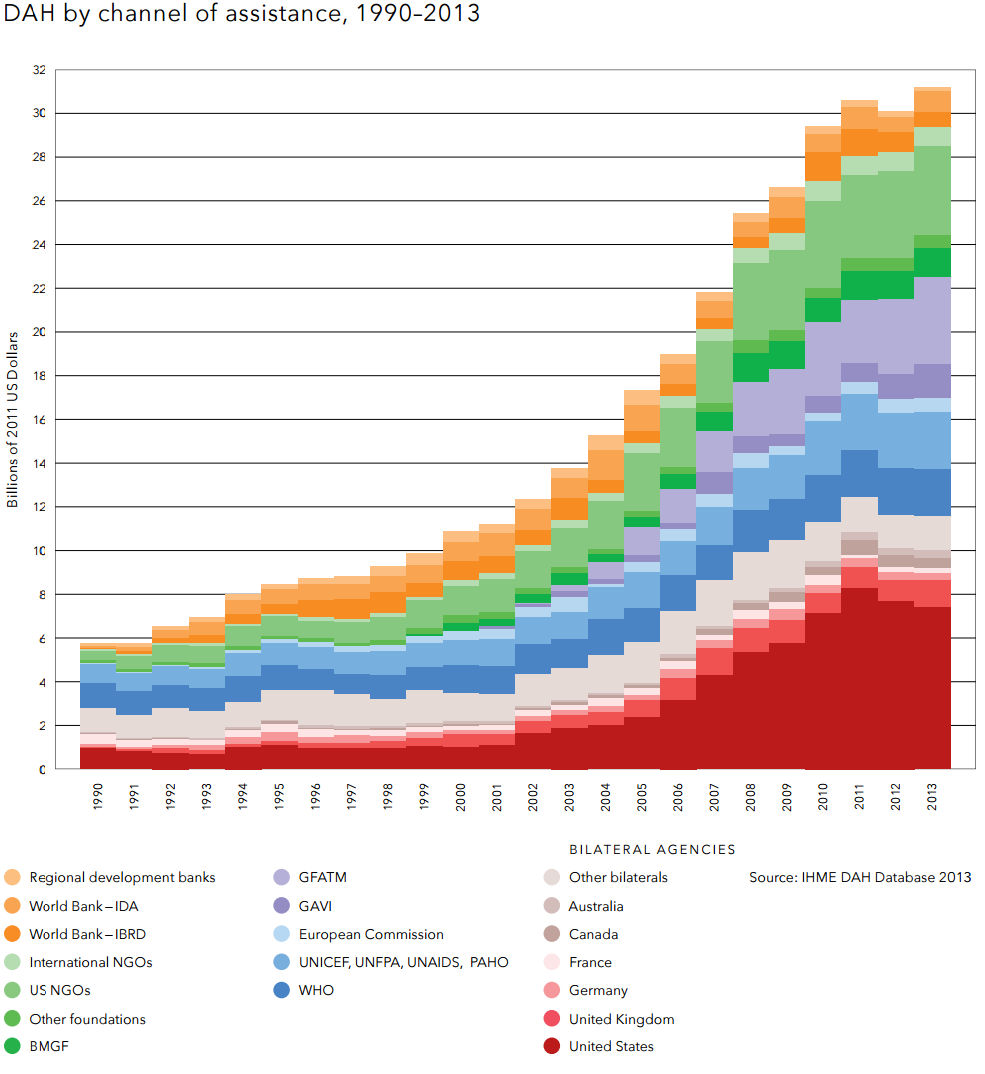
The Gates foundation spends about US$1 billion a year on global health interventions[23]. Countries spend only a part of their Overseas development aid on global health. Development Assistance for Health is only $31.3 billion a year (see figure below[24]).
Conclusion
In sum, there are likely going to be many, very cost-effective global health interventions (<$1000 per DALY averted) that have a lot of room for more funding (Billions of dollars per year) in the next 15 years. As the number of people who want to give effectively increases steadily, we will be able to conduct more research into finding out which cost-effective charities in the global health field are executing these interventions. Having more funds would also give us leverage to donate ring-fenced funding for effective interventions, such as bednet distributions, to bigger charities. For instance, AMF has only distributed about 6 million nets overall so far. In contrast, between 2002 and 2013, UNICEF procured over 213 million bednets and its share of the total global bednet delivery ranges from 20 to 37 per cent every year[25]. However, while UNICEF implements a wide range of very effective global health interventions (bednets, vaccines, autodisable syringes, Vitamin A supplementation, etc.), they also support less effective interventions. A foundation or the collective bargaining power of a number of effective altruists, could ask UNICEF to implement an additional, very effective bednet distribution programme in an extra country, but with more limited resources one’s donations would just go to UNICEF as a whole and so the effectiveness would be diluted[26]. In sum, there’s much funding needed in global health (see appendix) and the effective altruist community could potentially play a big part closing in on eradicating poverty!
Acknowledgments
I would like to thank Ben Kuhn, Toby Ord, and some anonymous reviewers for their helpful comments.
Appendix: The cost of fighting Malaria, Malnutrition, Neglected Tropical Diseases, and HIV/AIDS, and providing Essential Surgeries, compared to spending on Global Health
How much funding is required to substantially reduce the global disease burden? And how many Giving What We Can members would we need to finance the fight against diseases? One of our pledgers has recently given a great TEDx talk on this topic:
We have collected some more figures of how much it would cost to fight diseases and how many lives that would save:
Malaria: US$ 7.83 billion annually
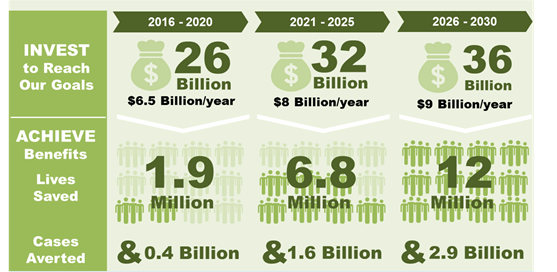
Preliminary estimations from a forthcoming WHO report[27] on Malaria suggest that, on average, $7.83 billion would have to be spent annually to reduce deaths and illness due to malaria by at least 90 percent. The figure below shows how many malaria cases would be averted and how many lives would be saved by this plan. Moreover, this plan might avert about 270 billion dollar 2030 in lost economic potential.
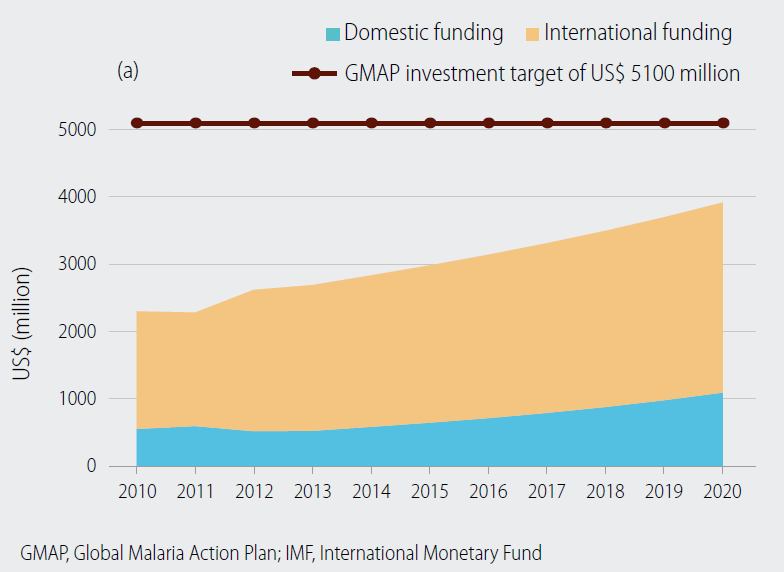
However, currently, only about 3 billion is spent on malaria (see figure below).
Figure adapted from[28]: Domestic and international investments increase in line with total government expenditure growth estimated by the IMF for 2014–2020 (note that the figures and the target are based on estimations from 2008); GMAP = Global Malaria Action Plan (GMAP)
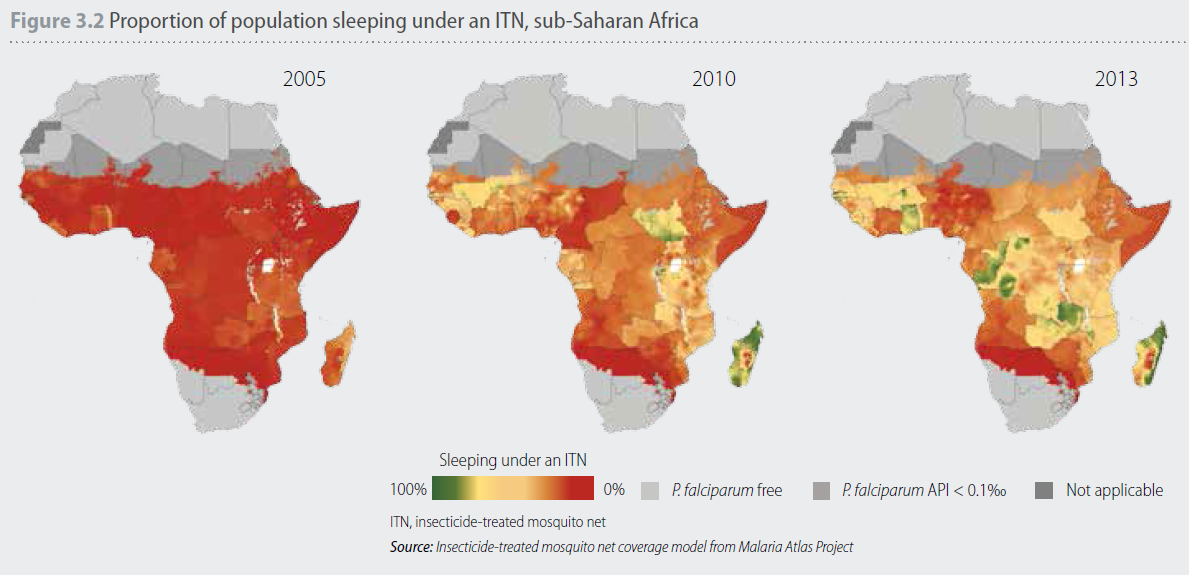
In 2005, the proportion of the population sleeping under a bednet was generally low, with only six countries achieving coverage levels greater than 20% (see Figure 3.2)[29]. Now many more people sleep under bednets, but not everyone who needs a net is able to sleep under one.
Malnutrition: US$ 10 billion annually
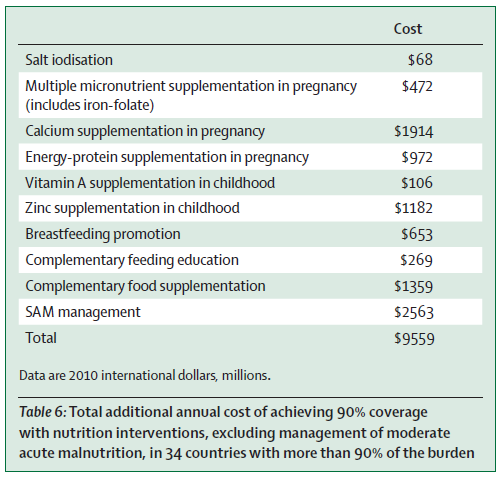
A recent review[30] suggests the total annual costs of achieving 90% coverage with nutrition interventions in the the 34 countries that are mostly affected by nutritional deficiencies would cost around $9.6 billion.
These estimates are similar to those of recent World Bank study[31], which estimated the nutrition scale up cost gap at $10.3 billion per annum globally. These investments would provide preventive nutrition services to about 356 million children, save at least 1.1 million lives and 30 million DALYs, and reduce the number of stunted children by about 30 million worldwide (globally 161 million under-five year olds were estimated to be stunted in 2013[32]).
For universal coverage (at least 80% of the population) against neglected tropical diseases, which include Dengue fever, Guinea-worm disease, Foodborne trematodiases, Lymphatic filariasis, Schistosomiasis, Soil-transmitted helminths (e.g. hookworm), and Blinding trachoma, the total investment targeted for the period 2015–2030 is US$ 34 billion excluding medicines (most of which has been pledged as in-kind donations by pharma companies)[33].
Developing countries will also fund a significant amount of this themselves.
Investment targets to overcome the global burden of NTDs are more than double current levels of foreign aid (10 times as much when including investments in vector control. It is unlikely that an increase in aid of this magnitude can be achieved[34].
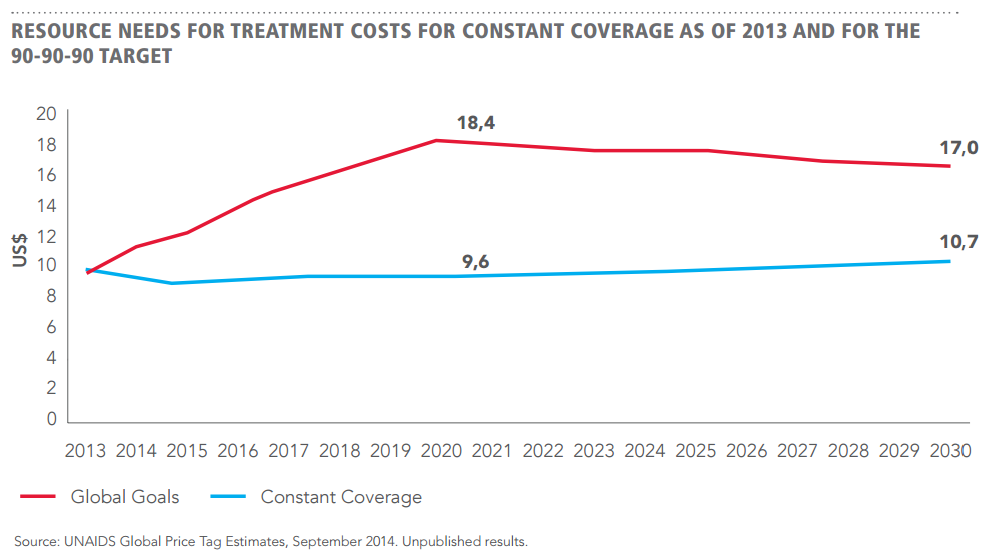
HIV/AIDS: US$ 16 billion annually
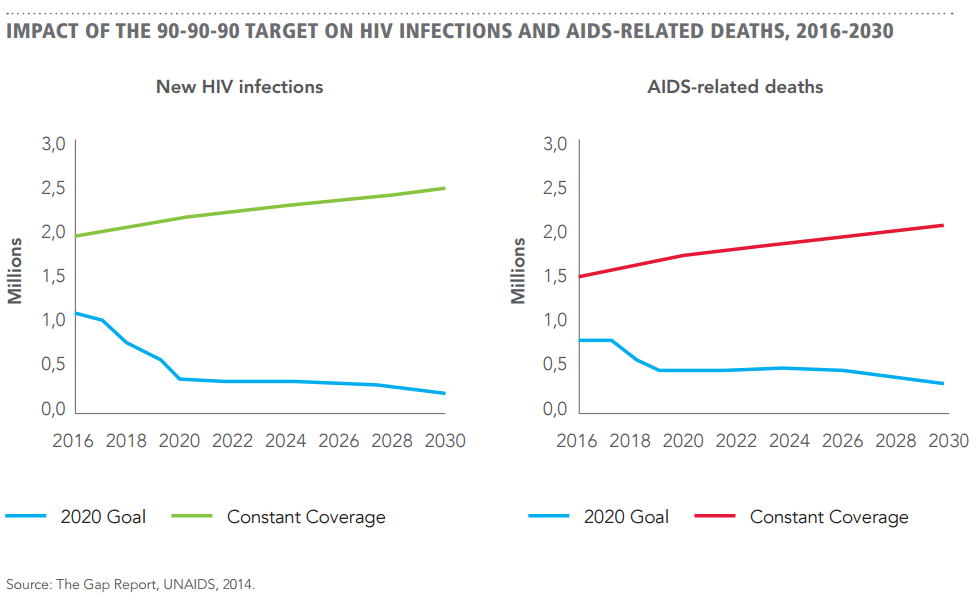
To have 90% percent of people living with HIV diagnosed, on treatment, and virally suppressed by 2020 requires about US$ 16 billion annually for HIV treatment, including drug costs, service delivery, community mobilization to ensure access to testing and retention in treatment, and pre-ART costs (see figure above)[35]. Achievement of this target by 2020, it is projected that nearly 350 000 people will die of AIDS-related causes in 2030, compared to 2.1 million deaths with continuation of current ‘constant coverage’ (see figure below)[36].
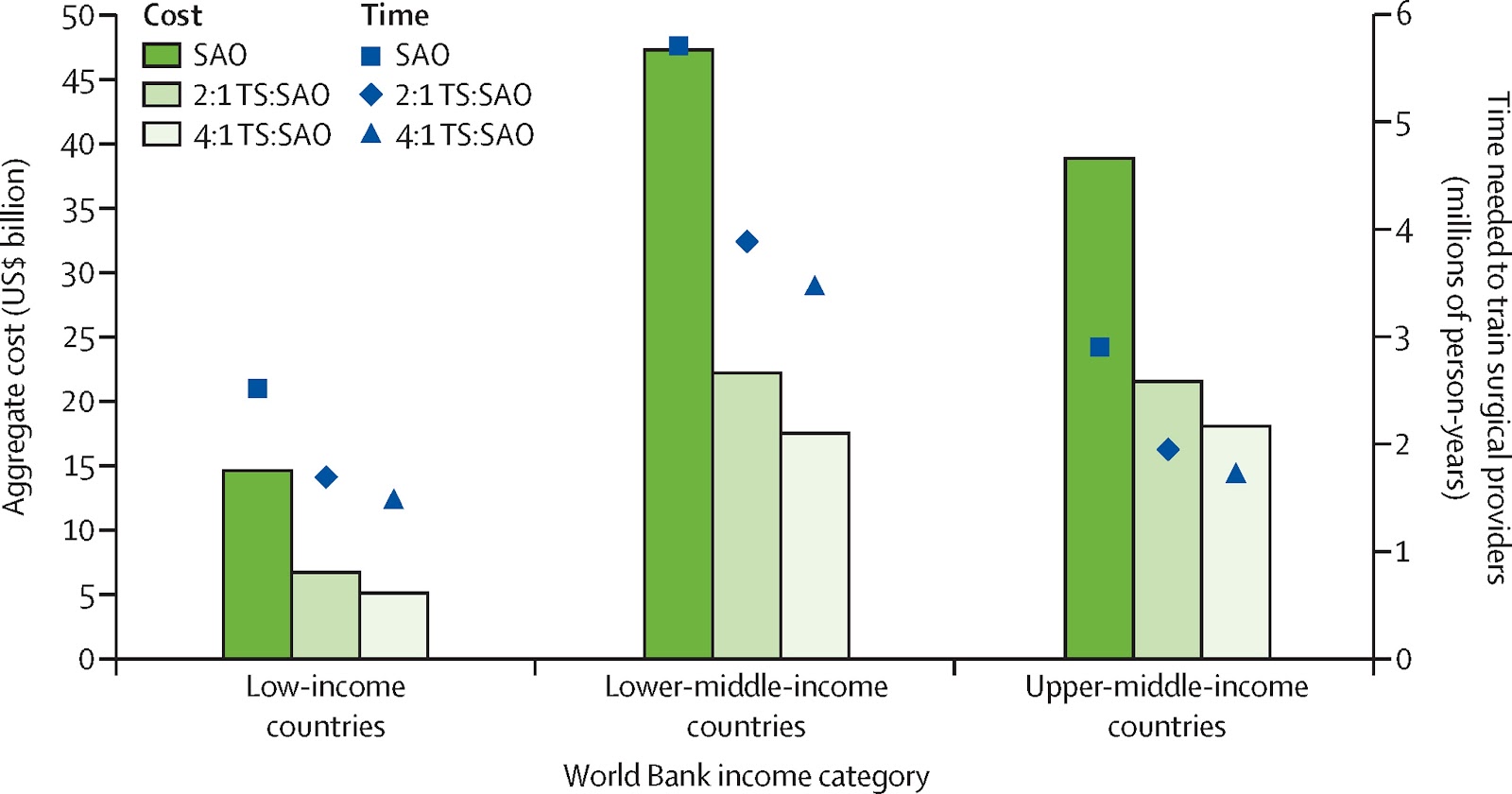
Essential Surgeries: US$24 billion annually
Figure: The cost and time needed to scale up the surgical workforce in low-income, lower-middle-income, and upper-middle-income countries in an SAO-only model versus a hybrid task sharing SAO model. The use of task sharing can decrease costs and time needed to scale up the surgical workforce to 20 providers per 100 000 population by 40%. SAO=surgical, anaesthetic, and obstetric. TS=task sharing. For information on Task-Sharing, see[37]
A recent study suggested that the total cost of scaling up essential surgical services over 2012–30 would be 298-552 billion dollars, which translates to annual average costs of about $16 billion to $31 billion per year[38]. Not only does this compares very favourably with estimates of the costs of scaling up services to tackle infectious, maternal, and child deaths above, but providing essential surgeries can be surprisingly cost-effective and cost as little as $33 per surgical DALY averted in sub-Saharan Africa[39].
Annual Global health spending:US$ 31 billion annually
Development Assistance for Health is only $31.3 billion a year (see figure below[40]).
Overall costs and Giving What We Can members required to fund this
Overall costs
Disease:
Annual Costs in Billion US$ dollars
Malaria
7.83
Malnutrition
10
Neglected Tropical diseases
2.3
HIV/AIDS
16
Essential Surgeries
24
Sum
60.13
Annual Global health spending
31.3
The cost of fighting Malaria, Malnutrition, Neglected Tropical Diseases, and HIV/AIDS, and providing Essential Surgeries is about US$ 60 billion, but the total development assistance for health is only US$ 30 billion. Of course, some low to middle income countries are able to use some of their limited domestic funds to fund their own health. However, most poor countries are not able to do this. Moreover, this calculation does not take into account the many other sources of ill-health.
We would need about 9,6 million people who give $3000 a year to effective organisations to close this gap.
Reid, Savanna. "Estimating the burden of disease from unsafe injections in India: a cost–benefit assessment of the auto-disable syringe in a country with low blood-borne virus prevalence." Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine 37.2 (2012): 89.
Mvundura, Mercy et al. "estimating the hypothetical dual health impact and cost-effectiveness of the Woman’s condom in selected sub-saharan african countries." International journal of women's health 7 (2015): 271.
Bhutta, Zulfiqar A et al. "Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?." The Lancet 382.9890 (2013): 452-477.
Verguet, Stéphane et al. "Timing and cost of scaling up surgical services in low-income and middle-income countries from 2012 to 2030: a modelling study." The Lancet Global Health 3 (2015): S28-S37.
Verguet, Stéphane et al. "Timing and cost of scaling up surgical services in low-income and middle-income countries from 2012 to 2030: a modelling study." The Lancet Global Health 3 (2015): S28-S37.

[Edit: I wrote a question in the wrong thread!]
Ha, oops!
Was this question meant to be posted here? https://forum.effectivealtruism.org/posts/GHFY6SpLkjML2Ld62/ask-everyone-anything-ea-101-1