Comments
How many people die from the flu? (OWID)

Saloni Dattani and Fiona Spooner at Our World in Data (OWID) have recently published a new article on the annual death toll of the flu — I thought the article was interesting and am link-posting it.
The article also explains some issues with measuring this, how this has changed over time, factors that increase the chances of dying from the flu, and why some flu seasons are worse than others. The headline (emphasis mine):
The risk of death from influenza has declined over time, but globally, hundreds of thousands of people still die from the disease each year.
[...]
The annual mortality caused by seasonal influenza was estimated by the Global Pandemic Mortality Project II using data between 2002 and 2011. They estimated that, during this period, seasonal influenza caused between 294,000 and 518,000 deaths each year globally.
For reference on what 300,000 to 500,000 looks like, here's a chart (from a different article) that shows deaths by cause:
An excerpt and a couple of charts — or just see the article itself.
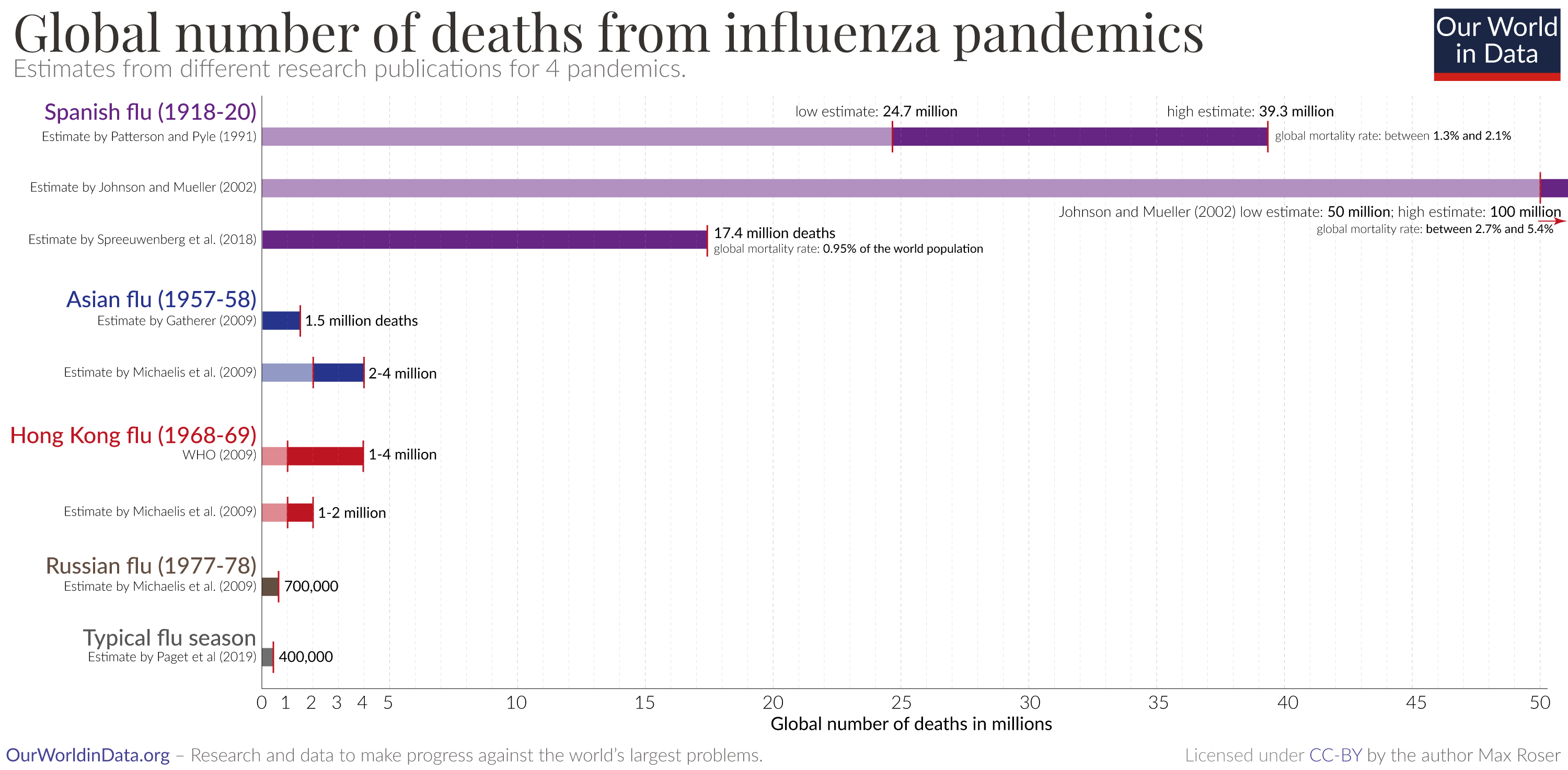
Globally, hundreds of thousands of people die from seasonal influenza every year. During large flu pandemics, when influenza strains evolved substantially, the death toll was even higher.
But the risk of dying from influenza has declined substantially over time from improvements in sanitation, healthcare, and vaccination.
People born in 1940 had around a third of the risk of dying from influenza as those born in 1900 – even when they reached the same age. This decline continued, and those born in 1980 have a risk of half that of those born in 1940.
Influenza still remains a large burden around the world, because of an aging population and a lack of access to healthcare and sanitation in many countries.
In this article, we look into these developments in detail: how many people die from seasonal influenza and how this has changed over time.
We will also look at which factors increase the risk of dying from the flu and understand why, in some years, influenza has led to large pandemics that caused millions of deaths. This knowledge can inform us about the risks of influenza in the future.


Would be worth using Disability-Adjusted Life Years rather than deaths in this sort of analysis because influenza is most deadly in the elderly and those with end-stage lung disease or severe immunocompromise, who may not have many DALYs left even if they are protected from influenza.
Any way you cut it, though, there are probably great cost-effective interventions we could do so save precious DALYs like expanding access to flu vaccinations.