This post is co-authored with Ben Garfinkel. It is cross-posted from the CEA blog. A PDF version can be found here.
Summary: Some strategic decisions available to the effective altruism m...
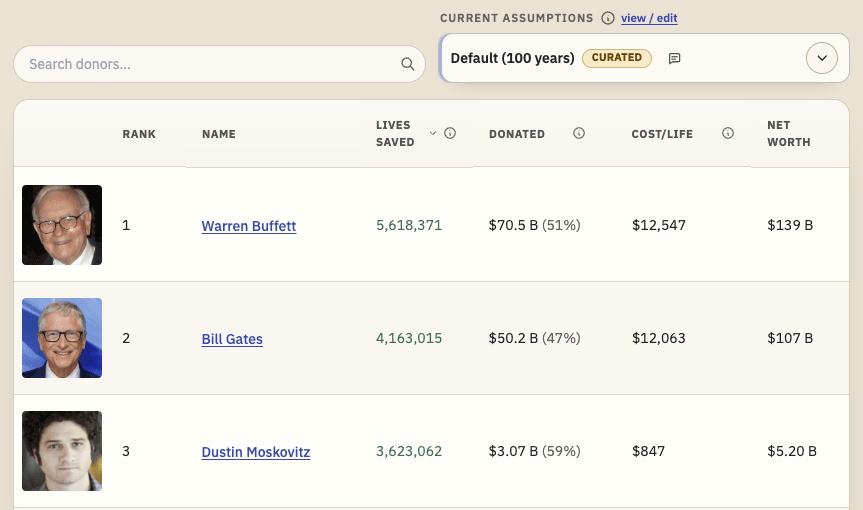
TL;DR: I'm releasing a website that ranks philanthropists according to EA principles and research, and allows users to re-rank the list using their own assumptions. I'd like feedback and help making it better. I'd especially like ideas for how to make the results more trustworthy. Funding may be available.
Crossposted to LessWrong.
...
Linkpost for my Substack piece, lightly adapted. Disagreement very welcome.
What happened
Coefficient Giving (cG) announced a $1 billion gift to GiveWell on 23rd July. This increases a previous commitment of $175m for 2026. cG say this could be a one-off surge, but it has implications for other donors either way. Both organisations...


I have the impression that the most effective interventions, especially in global health/poverty, are usually temporary, in the sense that you need to keep reinvesting regularly, usually because the intervention provides a consumable good; for example malaria chemoprevention: it needs to be provided yearly. In contrast, solutions that seem more permanent in the long-term (e.g. a hypothetical malaria vaccination, or building infrastructure), are typically much less cost-effective on the margin because of their high cost.
How do we balance pure marginal effectiveness vs eventually moving towards more permanent solutions? Could it be that by overly optimising for marginal cost-effectiveness, we might be missing a better ‘global maximum’ in the utility landscape, but we just need to descend from the current ‘local maximum’ to be able to get there eventually?
I think you're conflating intervention durability with outcome durability? A child who survives cerebral malaria due to seasonal malaria chemoprevention gets to live the rest of their life; SMC programs are rerun because (mostly) new beneficiary cohorts are at highest risk, not because last year's cohort's survival expires somehow. Similarly with nets and child vaccinations and vitamin A deficiency prevention (i.e. the GW top charities), as well as salt iodisation and TaRL in education and many other top interventions recommended by the likes of TLYCS and FP and so on.
I'd also push back a bit on the "permanent solutions" phrasing. Infrastructure isn't that permanent and requires ongoing expenditures and has a shelf half-life (I used to work in ops in fluid resource-constrained environments so I feel this keenly), diseases can develop resistance to vaccines so you need boosters, etc. Ex-AIM CEO Joey Savoie has a great blog talking more about how Someone Always Pays: Why Nothing Is Really "Sustainable".
Phrasing nitpicking aside, some big funders are in fact funding more "permanent / sustainable" solutions.
Open PhilCoefficient Giving's new $120M Abundance and Growth Fund aims to "accelerate economic growth and boost scientific and technological progress while lowering the cost of living", and Founders Pledge (which is almost OP-scale in giving) just launched a new Catalytic Impact Fund that targets "ecosystem leverage points" where small investments can build "sustainable, long-term solutions to global poverty and suffering".Jason's comment above on timetable speedup is essentially how e.g. GiveWell models their grants for malaria vaccines. The model says their grant would need to speed up co-administration for all highest need children in all of subsaharan Africa by at least 9 months to clear their 10x bar, so you can interpret their grant as a bet that funding that clinical trial would in fact achieve at least 9 months speedup. Notice how it's an uncertain bet; I think most donors (weighted by dollars moved) care quite a fair bit about certainty of direct benefits, so they'd probably donate to e.g. the Top Charities Fund instead of the more experimental EV-maxxing All Grants Fund.
Given EA's small share of the total global health/poverty funding landscape, the most likely effect of its investment on an expensive-but-permanent project is to speed the timetable up. So, for instance, perhaps we would get a hypothetical vaccine a year or two earlier if there had been EA investment. So, in comparing the effects of a yearly intervention vs. an expensive-but-permanent one, we are still looking at near-term effects that are relatively similar in nature and thus can be compared.
I don't suggest that is true for all "permanent" interventions, though, so it isn't a complete answer. It also might not scale well to a field in which EA funding is a large piece of the total funding pie.
I disagree with your point that saving the child's life is something you need to continuously reinvest in[1]. But I do think that you're pointing at something adjacent more along the lines of:
I kind of agree with this. Imo the only real long-term solution is economic growth. But that said, two points:
Funnily enough, your Malaria vaccine is an example of something that
Open PhilanthropyCoefficient Giving has funded. They funded a bunch of malaria vaccine research, notably the stage 3 trials of one of the two vaccines (I forgot which one)Once the child is >5y/o their chance to die drops a lot. Once you save their live once, you really don't have to reinvest to save their life again.
(I couldn't find the graph for sub-Saharan Africa, but it looks kind of the same)