Much attention recently has focused on far-UVC light, part of the spectrum of germicidal UV (GUV), and its promise for pandemic prevention. In the following medium investigation, we examine different kinds of GUV, their strengths, weaknesses, and crucial considerations in the real-world deployment of these interventions.
Throughout the report, we emphasize four points that we believe have been lost in some public discussions of far-UVC:
- A great deal of uncertainty remains around far-UVC interventions, to the point that we remain uncertain over the relative cost-effectiveness, all things considered, of far-UVC light versus conventional (~254nm) GUV in many settings.
- Cost-effectiveness depends on deployment context, including the dimensions of rooms, installation type (upper-room, full-room, etc.) assumptions about the mixing of air, etc. Combined with certain physical facts about air and light (e.g. the inverse square law), this complicates strong claims about far-UVC’s promise.
- GUV of any kind will not be a silver bullet for pandemics, but should be thought of as one potentially powerful tool in the health security toolbox, as part of a varied and layered defense.
- Small accelerations in adoption speed are likely not worth sacrificing safety and public perception. This is because catastrophic biological risks are relatively rare, and because public perception problems (if they arise) may be difficult or impossible to overcome.
In other words, we remain excited about the promise of GUV, but caution against over-hyping and over-investment in specific technologies and wavelengths. Far-UVC GUV is a relatively new technology. While it may have a larger upside than 254 nm upper-room GUV, many unknowns — both known unknowns and unknown unknowns — remain about this technology.
Much of this implies that some of our philanthropic and policy actions ought to be wavelength-agnostic. In the end, we expect that a mixture of systems and wavelengths — alongside other pandemic prevention measures — will be necessary depending on the deployment space and the type of threat.
With thanks to the many people who have generously reviewed and commented on earlier drafts, here's our report (and here is a PDF version with better formatting). Some readers may wish to skip to the sections on "Is far-UVC technology overhyped?" and "The complexity of comparing different GUV systems and wavelengths."

Medium Investigation: Germicidal Ultraviolet Light and Disease Transmission Reduction
This report summarizes a Founders Pledge shallow investigation into germicidal ultraviolet (GUV) light as a public health and pandemic prevention intervention. The report provides an overview of different types of GUV and outlines crucial considerations for grantmakers and policymakers. Additionally, we suggest potential “impact multipliers,” or features of the world that can guide effective giving under uncertainty about the cost-effectiveness of different interventions. Note that this report is scoped to focus specifically on GUV; for a comparison of other indoor air quality interventions, we recommend the recent report Air Safety to Combat Global Catastrophic Biorisk.[1] Our report is a cross-worldview investigation — Rosie Bettle’s research usually focuses on current generations and global health interventions, while Christian Ruhl’s research usually focuses on global catastrophic risks. GUV could have benefits both for a near-term reduction in the global burden of disease and for the prevention and mitigation of future catastrophic pandemics.
UV light has long been used for its germicidal effects, for instance for water treatment.[2] A less well-known application of UV light, until recently, is for airborne disease transmission reduction; UV light (of the appropriate wavelengths) can inactivate pathogens, rendering them unable to replicate and cause infection. However, some wavelengths of UV light are damaging to skin and eyes—meaning that these UV sanitization systems need to either avoid direct contact with people, or must be of a sufficiently short wavelength such that the UV cannot penetrate the outer surface of people’s skin and eyes. We review different types of GUV systems and wavelengths to determine whether funding this space could be impactful. On installation types:
- Full-room UV systems, where light is shone throughout the room. Far-UVC full room systems take advantage of recent developments in our understanding of which wavelengths can be safely used in occupied settings to inactivate pathogens.
- Upper-room UV systems, which have been used for decades and rely on air flow in the room to circulate air upwards, where viral particles within the air are inactivated by the UV light.[3]
- In-duct UV systems, where the air is sanitized by UV light as it passes through an HVAC system, as well as portable GUV systems, which function similarly to in-duct systems.
On wavelengths:
- Conventional UVC of 254 nm light, which has a long history of (upper room) deployment, but is damaging to human eyes and skin.[4]
- “Far-UVC” between 200-235 nm, which has some advantages and a potentially high upside as well as remaining uncertainties around safety.
We find evidence that GUV is a potentially impactful intervention towards improving indoor air quality that could reduce the transmission of pathogens and consequent pandemic risk (including for bioengineered pathogens); one recent analysis suggested that outfitting US public buildings with these systems could reduce overall population transmission of respiratory viruses between 30% and 75% (N.B., more research is needed on real-world estimates of transmission reduction, as discussed below, and there are large uncertainties surrounding such estimates).[5] In turn, air quality improvement appears to have been relatively neglected by mainstream funders such as government bodies and science funders, perhaps due to a historical belief that airborne transmission was not a key transmission route of respiratory disease.[6] Hence, we believe this cause area is promising for effective philanthropy.[7]
We then compare the different GUV systems (full-room, upper room, and in-duct systems) and wavelengths (far-UVC and conventional GUV), focusing on safety and efficacy. We are optimistic about the potential of far-UVC technology and its large upside especially for extreme pandemic events, and find that existing evidence suggests that this technology may have advantages for a wide range of applications. Nonetheless, we believe that more safety studies are needed both to reduce real uncertainties (especially with regards to eye damage, long-term exposure effects, effects on vulnerable populations, and uncovering unknown risks) and to bolster public confidence. In addition, a key uncertainty of far-UVC technology is its potential to increase indoor air pollution—these externalities and the necessary measures to mitigate them may push against future cost-effectiveness of far-UVC technology. Moreover, although GUV technology is highly effective at reducing the amount of airborne pathogens, it remains unknown how well such reduction translates into disease transmission reduction, and how far-UVC differs from 254 nm GUV in different contexts (e.g. there are some theoretical reasons to believe that far-UVC may be especially useful for certain extreme events).[8] We are therefore wary of over-hyping far-UVC technology over other indoor air quality interventions, especially existing GUV technology. Bearing in mind that existing GUV technology (such as 254 nm upper room systems) are already fairly effective, we argue that philanthropists should favor “wavelength-agnostic” advocacy rather than advocating for a specific UV system or wavelength—we don’t think the evidence for superiority of far-UVC is sufficiently strong as of late 2023 as to outweigh the risks of focusing specifically upon this technology, and potentially locking in inferior technology or turning the public against all GUV by rushing far-UVC deployment. Either way, we emphasize that — contrary to some public portrayals — GUV of any kind will not be a silver bullet for pandemics, but should be thought of as one potentially powerful tool in the health security toolbox, as part of a varied and layered defense.
We then identify specific impact multipliers within this space, with the aim of identifying promising funding opportunities. These include (1) leveraging societal resources via advocacy, since very large resources will be needed to roll out GUV technology (and we think it is possible that government funding bodies might move to produce more funding here), (2) focusing on high-income countries first, where there are already resources to potentially develop and use these technologies, (3) shaping research and design incentives (since there is a commercial interest here, we think it might be possible to promote private sector investment and therefore minimize the amount of philanthropic money needed), and (4) focusing on public perception over rapid deployment. With regards to the last point, we think there is a risk that (if GUV is rolled out poorly) public backlash might prevent the deployment of GUV for a very long time, perhaps when pandemic risk is higher than at present. With these impact multipliers in mind, we identify several potential funding opportunities; funding journalists to write about GUV (thereby potentially influencing fund managers and policy makers, and increasing public acceptance of GUV)[9], funding public advocacy groups, shaping market incentives to promote private sector research, and directly funding safety and efficacy studies. Our top recommendation is advocacy to leverage societal funds for large-scale research programs on real-world GUV pathogen transmission reduction.
Overall, we think this is a promising area and recommend proceeding to investigate potential funding opportunities within this space.
Disclaimers and Acknowledgments
The report was informed by semi-structured interviews of experts in UV germicidal irradiation. With thanks to Vivian Belenky, David Brenner, Ewan Eadie, Gavriel Kleinwaks, Matt Lerner, Kenneth Rockwood, Daniel Sacks, Jake Swett, Richard Williamson, and Kenneth Wood for their input and advice on this topic. All errors are the authors’ own.
Key Terms and Abbreviations
GUV/UVGI — Germicidal Ultra-Violet (GUV) light, also known as ultraviolet germicidal irradiation (UVGI). Some in the field prefer “GUV” because it does not include the word “irradiation” and its potential negative connotations in the public imagination.
Far-UVC — Far-UVC light refers to light with a wavelength of between 200-235 nm, but is currently near-synonymous with 222 nm light due to the path-dependent development of 222 nm emitting lamps (note that 222 nm is merely the primary emission peak of a wider band).[10] This wavelength range is thought to occupy a “goldilocks zone” where it is heavily absorbed by proteins in a way that can inactivate pathogens, but cannot penetrate mammalian skin or eye. Some prefer the phrase “low wavelength” over “far-UVC."[11]
Upper-Room GUV — The use of GUV devices in the upper part of an occupied room. These systems are designed to minimize exposure of room occupants to UV to safe levels (although leakage and accidents happen, and any claims about improved safety need to be accompanied by the caveat of correct installation and use). As air circulates to the top of the room, airborne pathogens are continuously inactivated by the GUV light. This approach has been around since around the 1940s.[12]
In-Duct GUV — The use of GUV within ducts, such as HVAC systems. As air circulates through the HVAC system, airborne pathogens are inactivated. This form of GUV can use wavelengths that would be damaging to people’s skin or eyes, but (similarly to upper-room systems) they are designed so that people never come into contact with the GUV light.
Portable GUV systems — The use of GUV within portable units, including HEPA air filtration units. These units typically contain a fan to draw in air, where the airborne pathogens are inactivated by UV light. Like in-duct GUV, these systems are designed so that people never come into direct contact with the GUV light.
nm — Nanometers, unit of measure equal to one-billionth of a meter and a scale used to measure the wavelength of light.
eACH — Equivalent air changes per hour, a measure used to compare different kinds of indoor air quality solutions on a commensurate scale. For example, 2 eACH means the air is cleaned at a rate equivalent to changing the volume of air in the space two times per hour.
KrCl excimer lamp — Krypton-chloride excimer lamps are the specific kind of lamp that has a peak wavelength around 222nm, and is currently used most frequently for far-UVC light emission.
Importance: Why Biological Indoor Air Quality Matters
Key Points:
|
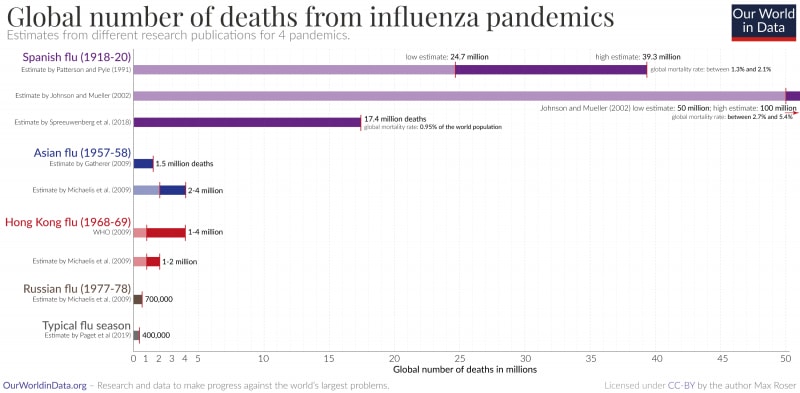
Respiratory diseases spread by the air impose a large burden of disease on the world. Hundreds of thousands of people die every year from influenza alone — the Global Influenza Mortality Project estimated that an average of 389,000 people (294,000-518,000) die every year from the flu.[13] These data, however, were based on information between 2002 and 2011. For pandemic influenza years, the numbers can be orders of magnitude higher:
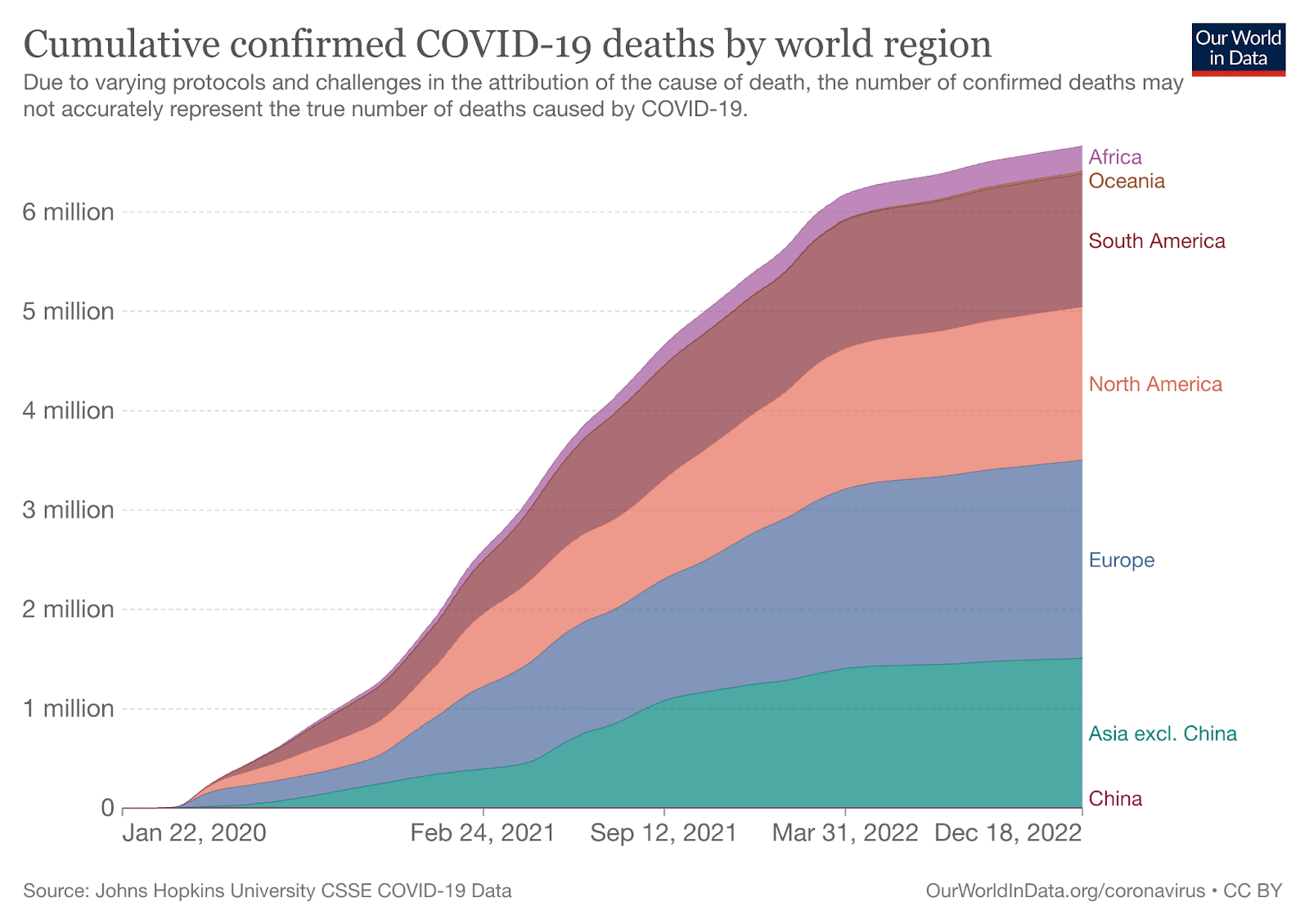
Cumulative confirmed deaths for the COVID-19 pandemic, too, are well over 6 million as of December 2022:[14]
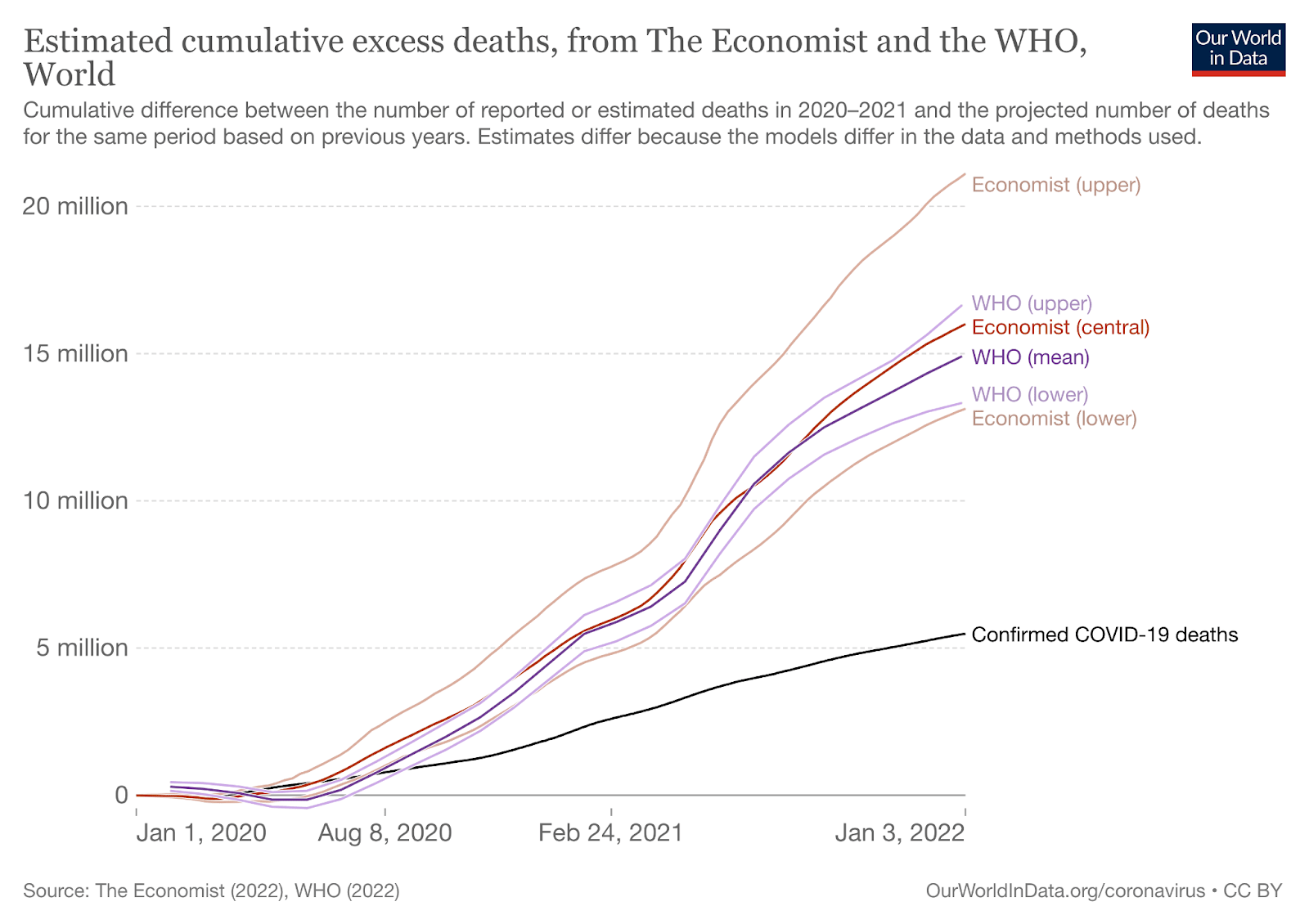
Cumulative excess deaths are likely far higher. As of December of 2022, median estimates were around 15 million:
The estimated annual burden of airborne disease is high:
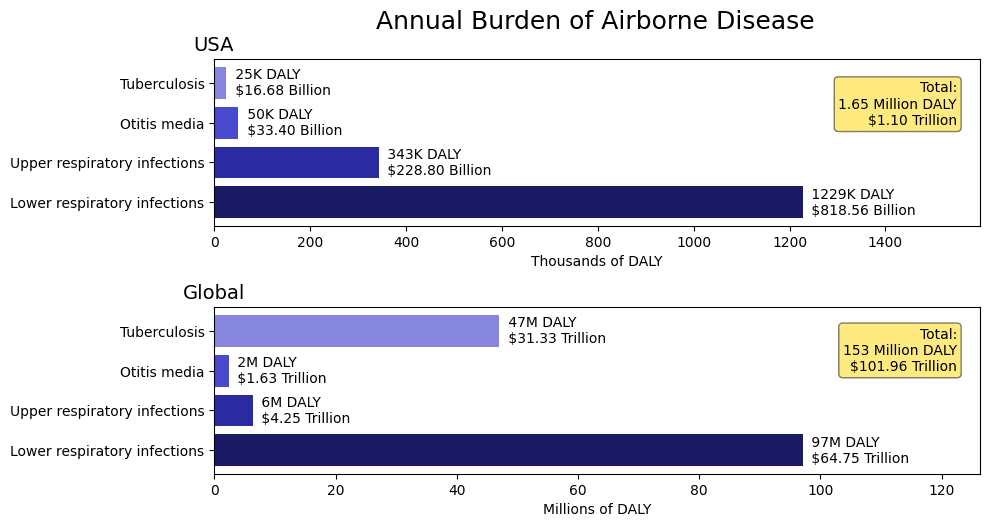
Source: 1DaySooner, shared by Vivian Belenky.
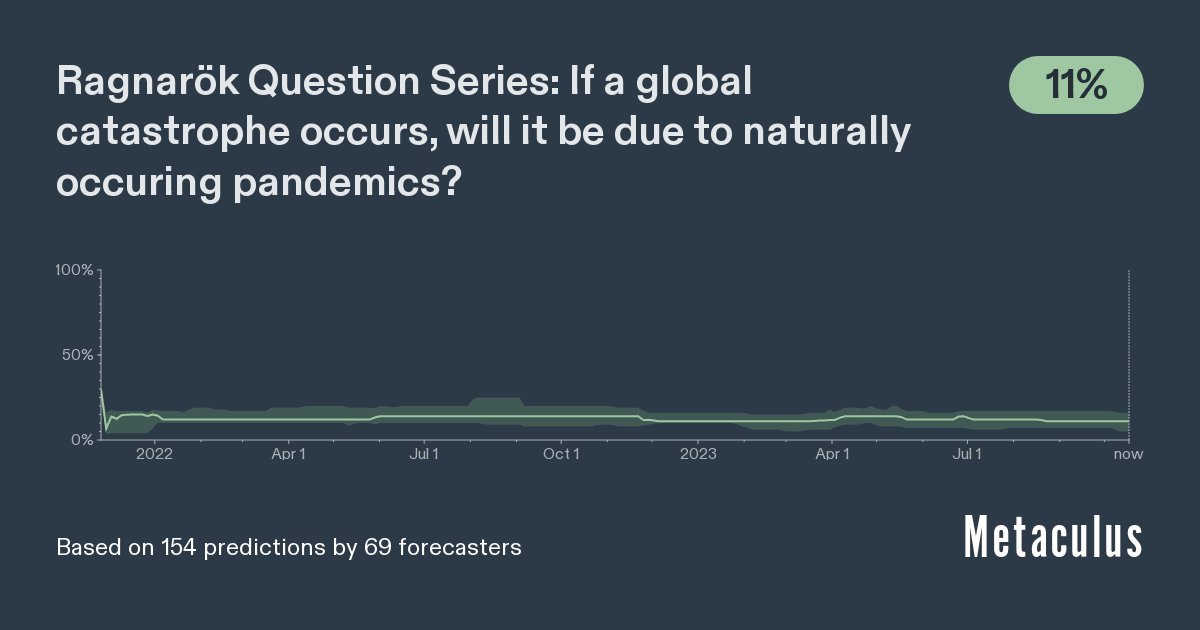
Natural pandemics could have catastrophic effects. On the crowdsourced forecasting site Metaculus, forecasters estimate that, conditional on a >10% decrease in global population by 2100, there is a 12% chance that this will be due to a natural pandemic (forecast as of October 2023):[15]
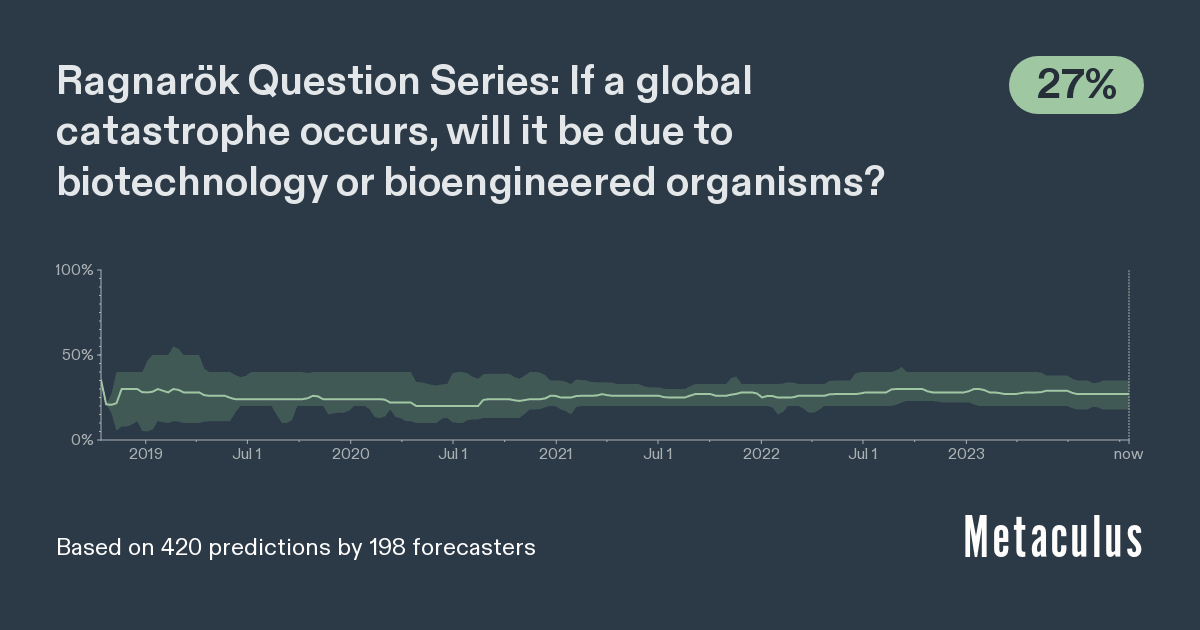
Evolutionary processes optimize pathogens for reproductive fitness, not lethality, suggesting that engineered pandemics could have even more catastrophic effects on humanity. As explained in Founders Pledge’s report Global Catastrophic Biological Risks, biological weapons, leaks from high-containment laboratories experimenting with enhanced potential pandemic pathogens, and other biotechnology disasters could all wreak havoc on the population and may even pose an existential risk to human civilization.[16]
In short, endemic disease poses a large burden on human wellbeing every year, and extreme events like engineered pandemics could cause global catastrophe or even human extinction. Interventions that seek to reduce the transmission of dangerous pathogens could therefore have high expected value from multiple worldviews. Humanity has taken concrete steps to reduce the burden of water-borne illnesses; we ought to do the same for airborne disease. As one recent report on indoor air quality frames the issue, “Indoor air quality, especially concerning infectious diseases, should be a priority public good, like fire safety, food safety, and potable water.”[17] One recent analysis estimated that a widespread program of indoor air quality improvement, including GUV, could reduce the transmission of respiratory viruses between 30% and 75%.[18] Airborne transmission is also an important factor in biodefense, where maliciously aerosolized agents have historically been a main delivery mechanism for bioweaponeers and would-be bioterrorists.[19] Crucially, GUV light is a “passive defense” that could be particularly useful for “stealthy” pandemics — those that may be spreading through the air without even being noticed, potentially with a long pre-symptomatic infectious period — which are particularly challenging to combat with traditional pandemic-preparedness measures.[20]
In short, interventions that help promote indoor air quality to reduce disease transmission could therefore be potential funding priorities for philanthropists concerned with having a high impact with their donations.
Current status of indoor air quality in the US
To understand the current status of indoor air quality in the US (and thus, whether this is an opportunity to significantly improve indoor air quality), it is necessary to consider how we can measure and compare indoor air quality. Indoor air quality is typically measured in air changes per hour (ACH); a calculation of how many times per hour the entire volume of air in a given space is replaced with supply or recirculated air. With a higher number of air changes per hour, the number of pathogens in the air decreases (as the pathogens are circulated out of the room); in a well-mixed room, each air change represents a reduction of around 63% in this pathogen load (whether the well-mixed assumption holds true in various scenarios is unclear).[21] The relationship between pathogen load and infection rate is complex, but we can also expect infection rate to decrease with pathogen load; we explore this relationship further in the efficacy section.
In this report, we focus on air quality in high income countries. Our thinking is that (in the immediate future) high income countries are more likely to have the resources necessary for rapid deployment and further research.[22] In the US, ventilation recommendations for most indoor buildings in America are set by ASHRAE (the American Society of Heating, Refrigerating, and Air-Conditioning Engineers), and the CDC. ASHRAE’s recommendations vary by building type, with a minimum recommendation in most households for 0.35 ACH (air changes per hour), and a recommendation for around ten times that in schools.[23] In healthcare settings, recommendations are higher; with a minimum of around 2 in patient rooms and 20 in operating rooms during surgical procedures.[24]Although it is not formal guidance, the CDC recommends at least 5 ACH inside buildings.[25] However, it is unclear whether these existing ventilation recommendations are met in practice; 1DaySooner estimates that 1-2 ACH is fairly typical for American buildings.[26] In line with this, Yamamoto et al. (2010) found averages of between 0.37-1.1 ACH in residences across different American states.[27] Given that the technologies described below are able to achieve ventilation rates in the realm of 20-30 ACH (and perhaps significantly higher; 1DaySooner estimated that far-UVC can achieve ventilation rates >100 ACH)[28], there is substantial room for indoor air quality improvement—and hence to reduce disease transmission.
Questions for Further Investigation
|
What is GUV?
Key Points
|
The germicidal properties of ultraviolet (UV) light have been well-documented since the late nineteenth century.[29] Shortwave “UVC” radiation is a subset of UV radiation with a wavelength of 100-280 nanometers (nm), which has been used in some public spaces, like schools and hospitals, for disinfection for nearly a century.[30] The use of UVC light to fight pathogens in human-occupied spaces has been limited, however, in part because much of this spectrum of light may cause harmful effects — erythema and photokeratitis — and the longer wavelengths may cause cancer and cataracts, as UVB does.[31] Some recent work on UVC light to fight pathogens has therefore focused on how to harness its germicidal power while avoiding the harmful effects to human skin and eyes.
These include three broad applications: upper-room UVC light, full-room UVC light (possibly via far-UVC), and irradiation of air as it passes through HVAC systems:[32]
NB: In the following sections, we occasionally refer to full-room systems and far-UVC systems seemingly interchangeably, because one major benefit of far-UVC is for occupied room systems, but the mechanical installation of UV systems is not wavelength specific; one can install >235nm systems for full-room irradiation (e.g. in a surgical room), and there may be promising applications of upper-room far-UVC systems as well as mixed systems.
| Irradiation Method | Full-Room GUV Systems | Upper-Room GUV Systems | In-Duct GUV Systems, and portable GUV systems |
| Description | Irradiating an entire room from above, possibly using far-UVC light, which may be safer for human skin and eyes. | Irradiating only a limited disinfection zone at the top of the room. This can be done with any wavelength of UV light. | Irradiating the air as it passes through the ducts of an HVAC system or a portable device. |
| Benefit | Very high rates of air disinfection.[33] Possibly useful for short-range transmission reduction. Possible safety and installation benefits with far-UVClight (e.g., easier to retrofit normal light fixtures) | Low safety risk if installed and used correctly,[34] since light is not in contact with people. Already used for over 70 years (e.g. to control spread of TB).[35]
Production costs are currently far cheaper than far-UV, and (as an established technology) there are already some technical standards in place. UVC LEDs, if the technology develops successfully, could make upper-room systems more aesthetically pleasing. | Low safety risk if installed and used correctly,[36] since light is not in contact with people. |
| Potential drawbacks | Not suitable for continuous irradiation with conventional 254nm UV light. Possible safety concerns regarding use of far-UVC light (this is a newer technology), and cost of existing far-UVC light sources. | More limited disinfection zone. Not suitable for low-ceiling rooms. Bulky installation. Operational complexity of installation, and potential lack of technicians.[37] | Rate-limited by the flow of air, therefore likely much less effective than conventional or far-UVC full and upper room systems. |
| Visualization |
Full-Room Systems
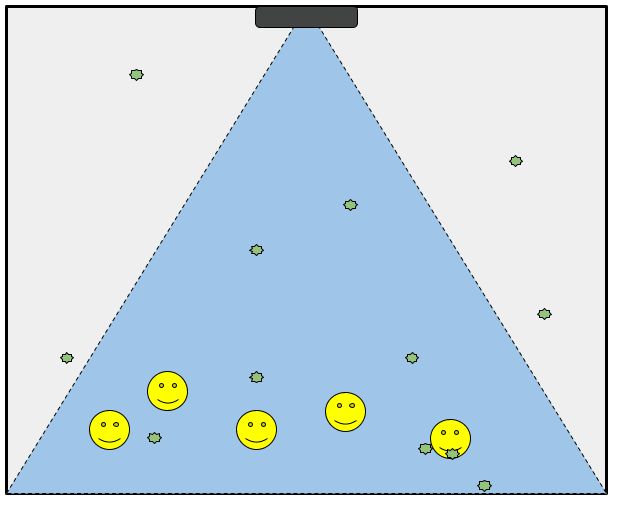
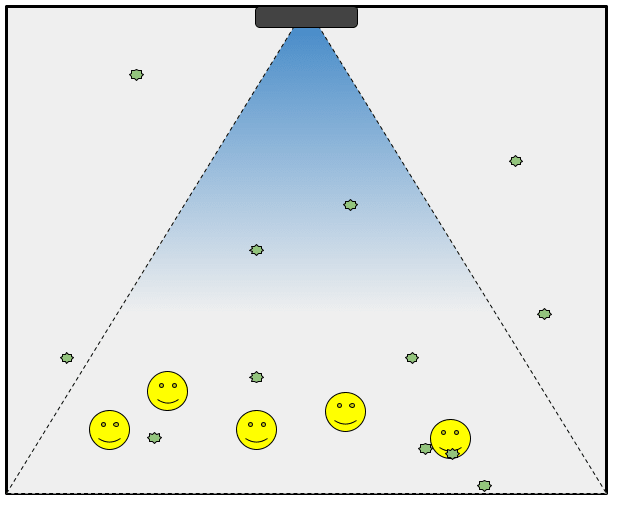
Full-room irradiation is conceptually simple; UVC lights, possibly mounted on the ceiling like normal overhead lights, irradiate an entire space:
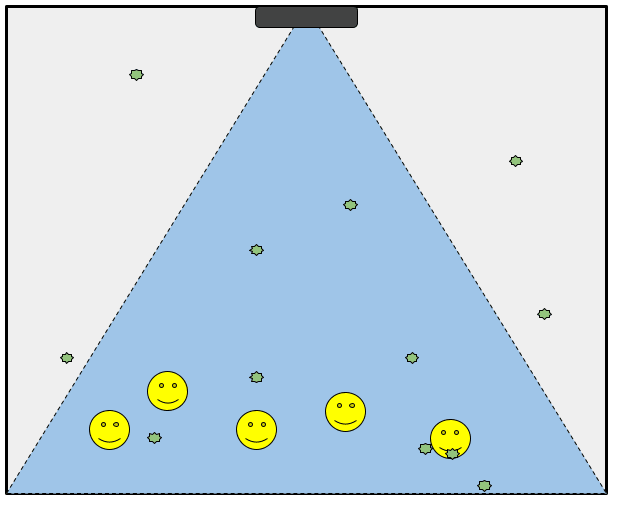
The difficulty with full-room irradiation, however, occurs when the room is occupied. An unoccupied room (like a surgery room after the patient and surgeons have left) can be easily irradiated in this way. In an occupied room, however, constant exposure to some wavelengths of UVC light can damage human skin and eyes, as explained in greater detail below. This makes occupied full-room irradiation with 254 nm UVC light unsafe, and unlikely to be adopted even if the pandemic-prevention benefits outweighed the skin damage. One kind of UVC light known as far-UVC, however, may help to solve this problem, as explained in the next section.
Far-UVC Light
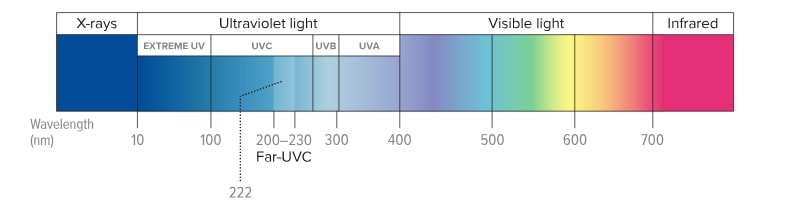
Far-UVC light is a wavelength of light in the 200-235 nm range (see diagram below).[38] In theory, far-UVC light could be a safe option because it occupies a Goldilocks zone of absorption — it can penetrate far enough into biological material to inactivate bacteria and viruses, but not far enough to pass the outer layers of human skin and eyes.[39] Notably, the rest of this report will often refer to “222 nm light” when discussing far-UVC; 222 nm is not necessarily the best wavelength, but is simply the wavelength emitted by most currently-available far-UVC lamps.
Diagram shows the electromagnetic spectrum and the position of UV light within it. Far-UVC light is a category of UV-C light, and has a wavelength of around 222nm[40]
Upper-Room GUV
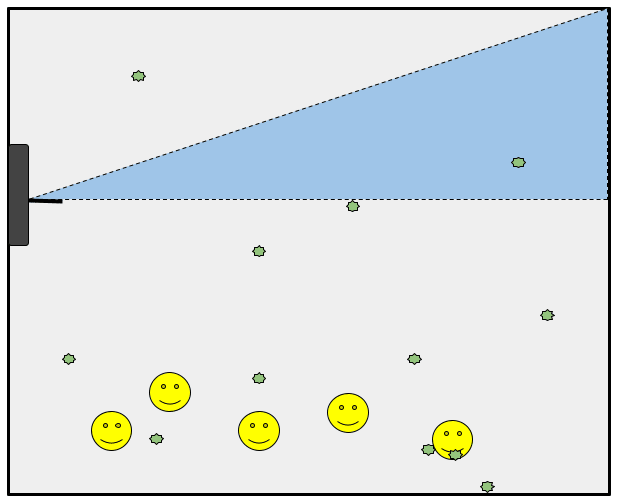
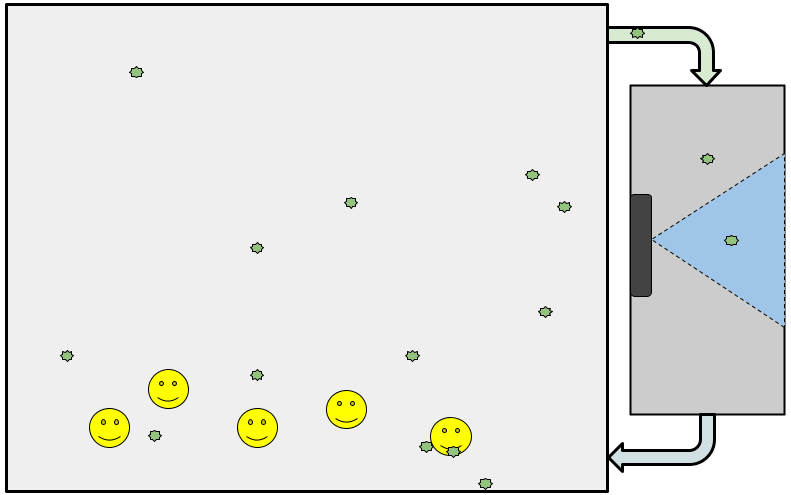
Upper-room GUV, by contrast, does not place humans in direct contact with UV light, and therefore does not require the use of far-UVC spectrum light. As illustrated in the figure below, however, this means that only a fraction of the room is directly irradiated. The human-occupied zone, however, is also the zone where transmission occurs. Therefore, upper-room irradiation alone is not enough; some air movement towards the irradiated zone is required (e.g. by good air flow design, fans, air purifiers, and HVAC — and potentially from the radiant heat of human bodies and other human activity).[41] The complexities of this are discussed in greater detail below.
In-Duct GUV
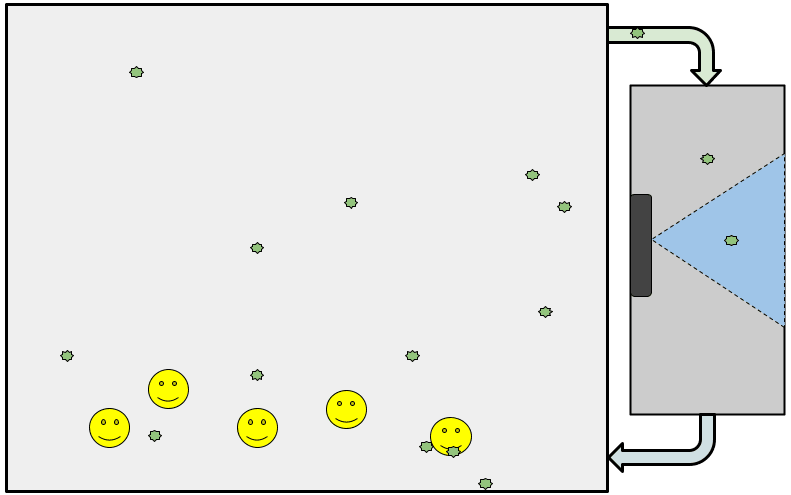
A third kind of GUV is known as “in-duct GUV,” and sometimes HVAC irradiation (although portable systems can also serve this function). In-duct GUV has the advantage of being able to use higher intensities of UV light, because humans are not exposed to the light.[42] As with upper-room irradiation, this form of GUV requires good airflow.[43] Most importantly, in-duct GUV is rate-limited and often further away from the site of infection. Experts we spoke with therefore believe that in-duct GUV is likely in a class far below full-room and upper-room GUV in terms of effectiveness. For this reason, most of this report does not discuss HVAC systems.
In general, in-duct GUV performs a different function from the other types of GUV, however, and may therefore be useful in some situations. For example, in situations where recirculation occurs, where transmission between rooms occurs via HVAC systems (e.g. in hotels), or where pathogens enter from the outside (as mold and fungi might). In these situations, with some kinds of pathogens, in-duct GUV may serve important pandemic-prevention and response functions.[44]
Benefits of GUV as a biosecurity intervention
Compared with other biosecurity interventions, GUV has a number of theoretical advantages that make it especially appealing to philanthropists concerned with maximizing the impact per dollar spent:[45]
- GUV can combat “stealthy” pathogens — because of the features highlighted in the following bullet points (it is a passive defense that is not pathogen-specific), GUV can help protect against the particularly insidious threat of pandemics that spread with little or no notice.[46]
- GUV is not pathogen-specific — unlike vaccines or most therapeutic interventions, GUV does not need to be tailored to specific pathogens. This has two follow-on benefits:
- No development time — finding and testing appropriate vaccines and therapeutics takes time; GUV, on the other hand, buys time for a more coordinated societal response by suppressing spread.[47]
- No dangerous research — work into active pandemic countermeasures is often used to justify research with enhanced potential pandemic pathogens, which may itself increase global catastrophic biological risk. GUV does not require this, and therefore intervenes more asymmetrically on pandemic risk.
- GUV does not require individual behavior changes — many biosecurity interventions require changing the behavior of individuals (convincing people to wear masks, to get vaccinated, etc.). As a “passive defense” GUV does not require this, as it simply disinfects a space as people go about their everyday lives.
- GUV can be a set-it-and-forget-it intervention — Pandemic preparedness follows cycles of attention and neglect, and societal responses to a newly identified pathogen can be sluggish. This suggests prioritizing interventions that do not require continued societal investment. Requiring GUV in building codes now could beneficially “lock in” improved biosecurity in a way that reliance on social distancing measures or continued vaccine uptake does not.
- Notably, there are also scenarios where additional GUV capacity could be installed in times of crisis, e.g. where the public tolerates the risk-benefit calculus of higher doses in order to respond to especially dangerous outbreaks. For these cases, stockpiling may be a useful intervention.[48]
What does GUV do that existing indoor air quality interventions (ventilation and filtration) do not? First and most importantly — as discussed in greater detail below (see Cost) — GUV has the potential to more effectively clean indoor air at dramatically lower cost than mechanical ventilation. Full-room GUV could potentially also reduce short-distance person-to-person transmission, and GUV could be used in spaces where mechanical ventilation is impractical, and with lower retrofitting costs. In short, it is possible that GUV could create a step-change in the cost-effectiveness of indoor air quality for disease transmission reduction. This possibility hinges on several uncertainties, however, which we discuss in the following sections.
Questions for Further Investigation
|
What do we know about the safety of far-UVC light?
Key Points
|
Primary Concerns: Skin and Eye Damage
This section tries to answer the question “are the safety concerns (in terms of damage to skin and eyes; other risks are covered below) of far-UVC light large enough that a deeper investigation would likely conclude this area is unpromising?” From this work, the authors subjectively estimate a ~15% chance that there are health risks which, once uncovered, will be severe enough to cause societal reactions that prevent or halt the scale-up of full-room far-UVC technology (and we don’t think these risks are sufficiently large that they make this cause area unpromising as whole).[49] Nonetheless, we highlight potential safety risks from long-term eye exposure, and to particular subgroups of the population (see below).[50] Recently-published and forthcoming work addresses safety issues in greater detail.[51]
- Mechanistic evidence
- Compared to other wavelengths of UV light, far-UVC (with a wavelength of 222nm) is strongly absorbed by proteins. Hence, the vast majority of photons are absorbed by the outermost (dead) layers of skin cells and do not reach living skin cells, and none penetrate deeply enough to impact replicating stem cells in the skin or eyes (where they could cause the mutations that might otherwise lead to cancer).[52] Consequently, far-UVC does not seem to incur similar safety risks (e.g. carcinogenic impacts) as other forms of UV light, although there is some uncertainty here.[53]
- Experimental evidence
- Skin: Existing evidence suggests that far-UVC is safe to skin;[54] far-UVC light’s photochemical effects are limited to the stratum corneum, such that exposing the outer layers of human skin to this wavelength does not increase yields of damaged DNA (pre-mutagenic DNA lesions, the mutations that can eventually cause skin cancer), while exposure of these cells to 254nm UV light does.[55] Filtered 222 nm light does not cause adverse skin reactions, and only minimal damage to the very outer (dead) layers of skin.[56][57] (Erythema — skin reddening — may occur if KrCl lamps are improperly filtered and include longer wavelengths alongside the 222 nm light.[58]) However, there is a lack of population-based studies, and (inevitably, given that this technology has been developed fairly recently) of long-term studies. Consequently, we think it is possible that particular subgroups of people (perhaps people who are using skin-affecting medications, or who respond especially strongly to UV light) may suffer adverse effects. Beyond carcinogenic effects, other risks that have been highlighted to us include immune dysregulation on the skin, and premature skin aging/ effects to the skin barrier.[59] Moreover, the use of far-UVC light is new, and the photochemical changes of far-UVC light exposure (such as skin discoloration) are not yet well-understood; as with many parts of this technology, there may well be unknown-unknown risks that we are not yet aware of.[60]
- Eyes: We have more uncertainty around whether far-UVC light could harm people’s eyes. Existing work on eye safety comes primarily from experiments with rodent eyes, which have suggested that far-UVC is safe at the kind of dosages we would expect a person to be exposed to[61] (but whether this will translate to human eye safety is unclear, and it is further unclear if eye discomfort might occur at lower levels of exposure—even if biomarkers of damage are not observed). Note that it is harder to test for impacts upon the eye ex-vivo, since the eye is an integrated and moving system that is difficult to replicate (e.g. with tear film, blinking, etc).[62]
Of relevance to both skin and eye safety, there is now one ongoing real-world study in Nova Scotia.[63] Residents of two elderly care homes will be cluster-randomized to be in either a neighborhood with newly installed far-UVC lighting, versus a neighborhood with placebo lights that do not have any far-UVC capacity.[64][65] While this study is primarily aimed at effectiveness (the primary outcome is whether diagnoses of respiratory viruses decline in communities that use far-UVC light), the researchers will also examine the health of the residents. Note that since the residents are elderly, the relative importance of carcinogenic exposure is presumably lessened (since these effects would take many years to appear). Consequently, we think this study is an important part of research into real-world effects, but believe much more work is needed, and note that the data will not be able to answer the question of whether long-term exposure to far-UVC increases the risk of conditions such as cataracts.
NB: Ultimately, the usefulness of this particular study will depend greatly on study design (e.g. whether it accounts for the movement of workers, whether it is powered appropriately, etc.). We understand that there have been recent modifications to the study design, and parts of the description above may be outdated. More on this study can be found in Dr. Rockwood’s presentation here.
Additional Safety Concerns
Ozone Production
We also briefly considered whether UV light sources could pose health risks through production of ozone. We found that the lamps used to produce 254nm light (used for upper room GUV and in-duct irradiation) are typically low-pressure mercury lamps, which do not produce ozone.[66] In comparison, the current lamps that are used to produce far-UVC light (KrCl lamps) can produce ozone. Moreover, although the amount of ozone that low power KrCl lamps produce appears to be fairly small, far from recommended limits for ozone concentrations in rooms, these limits are somewhat arbitrary and depending on the shape of the curve of ozone concentration to harms, even low concentrations may present health risks.[67] It is possible that certain high-power KrCl lamps will produce an amount of ozone that is a risk to health. Research and design advancements may reduce this problem (i.e. through advancements in far-UVC lamp technology that are already required due to various engineering problems; see section below). On balance, even with technological improvements, however, we remain concerned about the ozone generation problem.
Indoor Air Pollution
One concern sometimes raised about GUV is that UV lamps could create indoor air pollution by breaking down compounds in the air into secondary chemicals that have negative effects on human health. We consider this a potential crucial consideration when evaluating GUV as an intervention, given the large negative effects of air pollution, as outlined in Founders Pledge’s recent report on air pollution.
One study suggests that both 222nm and 254nm light can create such pollutants but that “these products do not necessarily have significant negative effects on human health because of their relatively low concentrations.”[68] This study caused a stir in December 2022 (and continues to), however, as it was accompanied by a Twitter thread and Substack post by one of the co-authors (Jimenez) that suggested that the particulate matter health effects (like increasing lung cancer rates) might be of a similar magnitude as the COVID-death-reduction effects.[69]
The BOTEC in the Substack post only focused on deaths avoided from COVID and flu, not on the potential total benefit to reducing airborne pathogen transmission in general (the full paper was recently published). Moreover, Jimenez assumes a linear reduction in deaths without justifying this assumption: “Let’s assume that GUV was installed in 1% of indoor spaces in the US, potentially avoiding 1% of those deaths, or about 1300 deaths per year.” It is not obvious that this assumption holds. If we believe, for example, that airborne transmission happens in part through “superspreader” events, for example, then installing GUV in 1% of indoor spaces, with a focus on high-transmission areas (schools, airports, etc.) could have a much greater impact than 1% reduction in deaths when counting the knock-on effects of preventing further infections. Viruses are contagious; air pollution is not. In a deeper investigation, we could attempt to calculate this and gain a better understanding of the potential trade-offs.
Moreover, the study simply used an open-source chemical simulator to run a computer model of these effects.[70] We are therefore uncertain about whether the inputs and assumptions of the model have “real world” external validity; in particular, we wonder whether many places where far-UVC light could be used might already have air ventilation measures in places, and how much the input assumptions about the composition of indoor air drive the results.[71]
Interestingly, insofar as we believe the results of the study, they suggest that air pollution is a greater factor in low-ventilation environments for far-UVC 222 nm light than for 254 nm light.[72] This is due to the specific photochemistry of 222 nm light; photons in the 222 nm light are more able to photolyze (break down) oxygen in the air to create ozone, relative to the 254 nm light.[73][74]
This suggests that smog-creation may be much more of a factor for far-UVC than for upper-room GUV, further increasing our uncertainty about far-UVC’s safety. The extent to which this affects real-world applications remains an open question. Some potential use cases for far-UVC technology — such as airports and other public spaces — already have existing mechanical air purification and ventilation technology, for example, such that we are uncertain on how much of a problem indoor air pollution will ultimately be. Moreover, not all spaces have the same amount of volatile organic compounds that figure into these issues. This may be important as some compounds related to cleaning products may be higher in spaces where air disinfection would be particularly useful (e.g. hospitals).[75]
Skin Microbiome
The skin’s microbiome contains millions of bacteria, fungi and viruses, which play a role in the protection against invading pathogens, the education of our immune system and the breakdown of natural products.[76] Some authors have suggested that far-UVC light might disrupt the skin’s microbiota.[77] While we think that further data examining this would be helpful, there are several reasons that we expect that this is unlikely to be a significant problem. First, far-UVC cannot reach within pores or other areas where light cannot reach (such as wrinkles). Given that the pores contain much of the skin’s microbiome, we think this limits the impact of far-UVC upon the skin’s microbiome—affected areas of skin can be recolonised from microbes within these areas. Perhaps more obviously, much of the human body is covered in clothing when humans occupy public spaces. Secondly, existing research examining the effect of handwashing and antimicrobial hand gels on the hand’s microbiomes have generally found small effects.[78]
Overall view on safety
Overall, we estimate a ~85% chance that there are no health risks from far-UVC which, once uncovered, will be severe enough to prevent or halt the scale-up of this technology. We update on the mechanistic evidence—although we think there is a possibility of unknown unknowns—and the existing experimental evidence. One of the primary reasons that we are not 100% confident is that we think it is possible that subgroups of people (such as old people with fragile skin/ eyes, or those who are prone to sunburn) might experience harm from far-UVC, whose reaction might not have been captured from the existing work with skin cells. In addition, it is possible that there are health effects from long-term exposure to far-UVC (such as risk of cataracts). Further, we note that there will need to be a series of safety trials prior to large-scale societal acceptance of this technology in Europe/ UK/ US. We think this technology is therefore at least a few years away from this kind of societal acceptance, which may make it more difficult to find current funding opportunities (with the possible exception of funding or incentivizing safety work).
Certain kinds of use cases could reduce safety concerns. For example, Max Görlitz has suggested that UVC systems could be outfitted with two possible “modes:” business-as-usual and emergency.[79] Emergency mode could be activated when the benefits of suppressing an ongoing severe respiratory pandemic clearly outweigh potential safety costs. In addition to the problems that Görlitz mentions (e.g. that businesses have no incentives to build expensive rarely-used capabilities into their units) we have two concerns with this proposal. First, business-as-usual mode might forego many of the passive defense benefits against “stealthy” pathogens mentioned throughout this report. Second, there may be strong public backlash against the use of “emergency mode” if that mode is specifically framed as having unknown safety effects.
Additional Risks
Public Reaction Considerations
Nearly everyone we spoke to about GUV raised the problem of public reaction to UVC technology. For decades, the public has been told that UV radiation is dangerous and must be avoided to avoid cancer — how do we tell them now that “actually, this specific kind of UV light is safe, and we want to install it in public spaces?” The apparent vaccine hesitancy and resistance to other pandemic prevention measures (masks, social distancing) during the COVID-19 pandemic also suggests that public communication about risk reduction measures is difficult. In one case, accidental exposure to 254 nm UVC light in a Northern African health system caused public outcry such that recently-installed lights were immediately shut off again.[80]
Some preliminary survey evidence from late 2022 suggests:[81]
- There is generally low awareness of GUV, and specifically of far-UVC light;
- Survey respondents had generally favorable attitudes towards GUV;
- There was “no statistically significant difference in support when using terms that mention UV vs don’t mention UV”
Moreover, contrary to belief that the direct contact of full-room far-UVC light with human skin would make people more likely to support upper-room GUV, the survey found that “respondents consistently showed slightly greater support for far-UVC over upper-room UVC.” As the investigators note, however, these responses were likely biased by the framing of the survey, which describes UVC in terms that understate remaining uncertainties (control framing):
“Some types of germicidal UV light can be harmful to the eyes or skin if people are directly exposed to them. If this kind of light were used in buildings, it would need to be set up in ways that did not directly expose humans to the light, but would still clean germs in the air (e.g., through installing the lights in air ducts, or in the upper part of a room (called upper room UVC), where they clean circulating air). Another type of germicidal UV light (called low-wavelength light or far-UVC), may be safer. It has little to no effects on the skin or eyes, while still killing germs.”[82]
Overall, we do not update much on this survey evidence, other than to note that public attitudes about GUV do not seem to have clearly crystallized yet. “Elite” attitudes (e.g. healthcare professionals, hospital administrators, policymakers) will also matter, both directly (in shaping policies) and indirectly (in providing “elite cues”).[83] We do not view the slight preference for far-UVC light to reflect anything other than the framing of the survey itself. Future surveys may probe whether there are partisan or demographic differences, to better understand whether this issue is likely to be politicized the way that e.g. vaccines have been. From a philanthropic perspective, greater funder diversity could be useful to help ensure that GUV interventions are not politicized or seen as pet projects of certain kinds of funders. Public science funding could be especially helpful here, as discussed later.
Dual-Use Potential and Security Risks
As with all potential biosecurity interventions, it is important to consider the possible dual-use applications of GUV. There are several potential sources of concern. First, it is possible that more research on GUV will facilitate work on dangerous pathogens. For example, if one factor keeping scientists and militaries from pursuing more of the most dangerous gain-of-function or biodefense experiments is the potential for accidental infection and laboratory leaks, then if GUV reduces the perceived risk, there may be more of this research. It is unclear whether this is a real risk pathway, or whether the benefits to biosafety simply outweigh any such effects. We therefore believe this concern is minor compared to the concern outlined in the following paragraph.
One potential concern is that GUV may become a victim of its own (perceived) success. Imagine a near future in which GUV becomes humanity’s primary protection against pandemics, with decreased emphasis on social measures, vaccine development, and therapeutics (e.g. because these are perceived to be redundant). This need not be because GUV is actually good enough to serve as a single defensive layer (we believe this is highly unlikely), but because it is perceived as a “silver bullet” solution. In such a world with single-layered biosecurity, bad actors could focus on engineering UV-resistant pathogens in order to cause a massive pandemic.[84] Importantly, however, while such risk-shifting is theoretically possible, wide-scale application of GUV would still restrict malevolent actors so heavily that the benefits may well outweigh the costs of a new vulnerability.
Moreover, while it is possible to think of dual-use applications of GUV, there are feedback loops that would allow us to assess whether these concerns are real. For example, if it really were the case that the world moved to a single-layered biodefense, philanthropists and policymakers could notice this trend and work to correct it. Moreover, GUV does not seem to directly enable bioweapons development or deployment in the way that other technology does.
As a counterpoint to these security concerns and worries about risk-shifting, however, it is important to note that robust defenses can have a deterrence-by-denial effect. In security studies, deterrence by denial refers to the idea that strong defenses can convince an adversary that an attack will not achieve its objective.[85] In the case of biodefense, deterrence-by-denial via widespread GUV technologies in a country could have the following effects:
- Convincing malicious actors with existing bioweapons capabilities that biological attack on the relevant country would be futile;
- Convincing malicious actors without existing bioweapons capabilities that the pursuit of such capabilities has low payoff (because of point 1).
In summary, we believe that the security concerns accompanying GUV technology are manageable and likely outweighed by their security benefits via both defense and deterrence.
Resistance risks
Viruses in particular are notorious for their ability to rapidly evolve in response to new challenges, such as drugs and host immunity.[86] Analogously to antibiotic resistance, we think that there is some risk posed by the possibility of UV-resistant pathogens in the future (if this technology was widely adopted)—but we think the risk is less severe than that posed by drug resistance. UV light deactivates pathogens by passing through their cell wall/ viral envelope, and breaking molecular bonds that bind the pathogen’s DNA or RNA together. Consequently, the adaptations necessary for a pathogen to become resistant to UV light would inherently affect fundamental properties of the pathogen (such as the make-up of the cell wall, or structure of DNA molecular bonds), which experience competing selection pressures to stay constant.[87][88] Note, however, that scientists do not have a full understanding of the mechanism of inactivation of far-UVC light, increasing our uncertainty about potential resistance risks.[89]
Nonetheless, we note that there are some naturally-occuring bacteria which appear to be resistant to UVC light.[90] As far as we are aware, UVC-resistance has not become a major issue in medical spaces where GUV has been in use for nearly a century.[91] Whether UV-resistant potential pandemic pathogens could be engineered in the future and released deliberately (by malevolent actors) or accidentally (i.e. via a laboratory leak) is unclear. The mere existence of such pathogens created by natural selection, however, underscores the importance of “defense-in-depth” or “layered defense” — GUV could be an important tool in our pandemic preparedness and response toolkit, but cannot on its own eliminate the threat of pandemics.[92]
Damage to Plastics and Other Materials
Ultraviolet light in the UVC spectrum is known to cause significant degradation in many types of plastics.[93] The damage depends on the type of plastic, the duration and intensity of exposure, the presence of UV stabilizers or protective coatings, and the presence of environmental factors like temperature and humidity.[94] Because “sensitivity of plastics decreases exponentially with wavelength,” far-UVC irradiation may be more damaging than other kinds of UV exposure.[95]
In a recent report on indoor air quality and GUV, the authors argue that “the rate of degradation may overall be negligible compared with the standard lifetime of consumer products.”[96] We remain highly uncertain about this, in part because many UV-resistant plastics are targeted mainly at UVA and UVB spectrum light from the sun, and not at intense long-term exposure to far-UVC light. In spaces housing expensive equipment with exposed plastics, we believe this may become a serious issue that can affect both the actual cost-effectiveness and the perceived cost-effectiveness (and therefore public openness to adoption). A 2023 study on materials used in public bus interiors found significant damage and discoloration, with serious increases in brittleness for some materials (up to 26% decrease in “elongation at break,” with low elongation at break indicating brittleness).[97] Indeed, the study claims to have studied the equivalent exposure of “6.2 years of city bus disinfection,” but this is assuming only intermittent disinfection (10-15 minutes after 1 hour of driving for 16 hours a day); for effective indoor air quality applications, exposure would be longer, such that we may assume even worse degradation of materials.[98] We believe that this could be an important consideration for adoption in spaces with many susceptible materials on critical (and expensive) systems, such as healthcare spaces.[99]
In addition to non-living materials like plastics, there are also additional concerns about the unknown effects of UV light on other forms of life, such as houseplants, which may be important for adoption.
This is mainly an issue for full-room irradiation with far-UVC light; upper-room conventional UV would not come into contact with any plastics in the lower parts of a room.
Questions for Further Investigation
|
Comparing Different Types of GUV
Key Points:
|
This section briefly attempts to compare different types of GUV. While we view GUV as a promising intervention overall, and have some reasons for believing far-UVC light will be especially cost-effective in the future, we remain highly uncertain about the balance of comparative advantages and disadvantages of different wavelengths of UVC light. Our overall view, discussed below, is summarized in the following table (we do not include in-duct UV, since we think in-duct UV is likely to have similar considerations as upper-room UVC, but with lower effectiveness):[100][101]
| Consideration | (Full-room[102]) far-UVC | (Upper-room) conventional UVC |
| Effectiveness | Full-room far-UVC may achieve ~128-322 eACH in ideal conditions for some pathogens.[103] Transmission reduction is unclear, due to lack of real-world studies and questions about the validity of existing models of airborne transmission. Consequently, we have uncertainty here, but estimate a 70-90% transmission reduction (see “Efficacy” section below). An advantage of far-UVC is that it could be deployed for short-range transmission reduction (but this remains highly uncertain at current exposure levels[104]).
| Upper-room GUV achieves ~24-100 eACH, potentially reducing transmission rates by approximately 60-80%.[105] Proven technology.
NB: there is uncertainty on the eACH estimates for various kinds of GUV, too, given complex questions like the creation of air currents and “pockets” of pathogens.
|
| Safety (skin and eyes) | In theory, far-UVC light physically cannot penetrate the layer of dead cells on human skin or the film of tears on human eyes, suggesting it is likely safe. Uncertainties remain on long-term exposure, on certain vulnerable groups, and on eye effects. | Lower uncertainty. Upper-room GUV with 254 nm light does not come into contact with humans when installed and used properly; therefore safety considerations are much better understood. Accidental exposure can cause temporary skin and eye damage, which, even if not dangerous, may have important effects on public perception and adoption. |
| Safety (indoor air pollution) | Concerns have been raised about potential effects on indoor air quality. More real-world studies are needed. | Lower concerns about indoor air pollution. |
| Cost | Currently more expensive. Costs may drop, but necessary additions to account for air pollution and plastic degradation may limit cost declines. | Currently most cost-effective indoor air quality intervention. The cost of 1 ACH by GUV is about $14 USD, nearly an order of magnitude cheaper than ventilation. |
| Installment/retrofitting Considerations | Far-UVC light can be used in rooms of various heights, does not require specific ventilation conditions, but may not reach areas in shadows. | Can only be installed in rooms with appropriately high ceilings (above ~7 ft), may require vertical air movement. |
| Public perception | Unclear; there could be public backlash against the use of far-UVCtechnology, if it is perceived to be unsafe | Unclear, but the fact that it has been somewhat in use since the 1940s might reassure the public |
| Usefulness for Global Catastrophic Biorisk Reduction | Theoretical advantage in reducing short-range person-to-person transmission. Effect size unclear; more work to understand real-world effectiveness is needed. | May be sufficient for reducing transmission of pandemic pathogens, with an old study showing significant reduction in influenza incidence. |
Is far-UVC technology overhyped?
Much recent attention on GUV since the COVID-19 pandemic has focused on far-UVC (222nm) lights specifically. Far-UVC has some theoretical advantages, as discussed below. Nonetheless, we are concerned that the biosecurity funding community may have a bias towards exciting new technology of far-UVC lights, when 254nm UVC lights are a proven technology with a century of use. Of course, it is possible that “new” technology may be able to find widespread application more easily than the more conventional technology that has languished without much adoption for decades Within the Effective Altruism community specifically, we note that far-UVC light has received significant attention (e.g. brought up by Will MacAskill in The Guardian here, and referenced on the EA forum here), yet we are not aware of a similar focus upon upper-room systems.[106]
It is possible that this difference is justified (for instance, if far-UVC is significantly more effective than upper-room systems), but we have several key uncertainties about far-UVC lights:
- What are the potential safety hazards of far-UVC lights, especially for less-studied issues like eye damage, and in sub groups of the population that might be especially vulnerable to far-UVC light? What can we know about the long-term effects of constant UVC irradiation?
- In real-world applications, how much more effective is full-room far-UVC light at reducing not just pathogen load, but also at reducing disease transmission?
- Which wavelength (far-UVC or conventional GUV) can be installed across a wider range of buildings (e.g. because of aesthetics, ceiling height, plastic degradation, indoor air quality, etc.)?
- What are the costs of reducing uncertainty about these questions (study costs, opportunity costs, public perception costs) when potential “good enough” technology exists?
- What are the market obstacles that currently keep far-UVC lights relatively expensive? What market interventions can help decrease cost and thereby catalyze greater demand?
Depending on the answers to these questions, we believe it is possible that the recent focus on far-UVC technology has been misplaced. Below, we attempt to answer some of these questions.
We divide our analysis into three sections: efficacy, safety, and cost. On efficacy, there are several reasons to believe that full-room 222 nm (far-UVC) irradiation will be more effective in reducing transmission than other types of GUV, though the magnitude of the difference remains uncertain. On safety, full-room far-UVC irradiation ranks below upper-room and in-duct irradiation; although far-UVC light is probably safe, and accidents occur even with upper-room UVC, upper-room and in-duct GUV simply does not come in contact with humans, and therefore poses a much lower safety risk in expectation. On cost, our uncertainties are high; 222 nm lights remain expensive, but costs may decline, and full-room irradiation may have some cost-advantages in retrofitting — many rooms have overhead lights, but not all rooms are suitable for upper-room or in-duct GUV. We also suggest that public perception of safety may be just as important as actual safety.
We conclude that our uncertainty is high-enough to warrant a wavelength-agnostic approach to funding UVC GUV interventions, as described under “What Could a Philanthropist Do?”
The Complexity of Comparing Different GUV Systems and Wavelengths
Before the discussions that follow, it is important to note that comparing different GUV systems and wavelengths is a deeply complex endeavor. It is not strictly possible to say that one wavelength is “better” than another (safer, more efficacious, etc.) without discussing that wavelength in its deployment context.
For example, conventional 254nm light could not be deployed in full-room systems (for occupied rooms) without causing significant damage to skin and eyes, whereas far-UVC light can be. On the other hand, both far-UVC systems and conventional GUV can be deployed in upper-room systems, but historically such systems have used only conventional 254nm UV light. Even upper-room systems have accidents and leaks, can be installed incorrectly, and people may simply enter the irradiation zone (e.g. when using a ladder to access the ceiling). Thus, the safest deployment combination would appear to be far-UVC light deployed in upper-room systems, and we believe that this is a promising approach for more widespread adoption if concerns about indoor air pollution are resolved.
Safety is not, however, the only relevant consideration. Comparing different systems and wavelengths on efficacy, too, turns out to be deeply complicated. For example, when we began our investigation, we believed that full-room irradiation was strictly better than upper-room irradiation — after all, we reasoned, shining germicidal light on a greater fraction of the air surely eliminates a greater fraction of the threat. Thus, because only far-UVC light is suitable for full-room deployment, we expected to recommend targeted investment into far-UVC light, as many other funders have also focused on the exciting new far-UVC technology. This turns out to be more complicated than we expected, and highly context-dependent.
Part of the complexity is the result of the inverse square law, which applies to various physical phenomena, including light, which dictates that the intensity of the light decreases with the square of the distance from the source of the light.[107] In other words, doubling the distance from the source decreases the intensity by a factor of 4. Our original drawings ought to therefore be modified thus:
Assuming constant intensity vs. Reality: the Inverse Square Law
In other words, the efficacy of full-room vs. upper-room systems ultimately will depend on the dimensions of the room, the air movement, and where in the room the threshold limit values are reached. For certain high-ceilinged spaces, it is possible that full-room systems deployed from the ceiling may be significantly less effective than upper-room systems deployed in great numbers and high power just above the inhabited zone (though this remains highly uncertain). This depends ultimately on the specific deployment of the lights — for high ceilinged spaces, the flux of the lamps may be increased such that the threshold limit values are reached at the occupied zones; for other spaces, wall-mounted far-UVC lights could also be useful.[108]
This could be an effective intervention for some high-transmission public spaces, but we remain highly uncertain about the importance of irradiation in the breathing zone — again, more work to understand real-world effectiveness is needed.
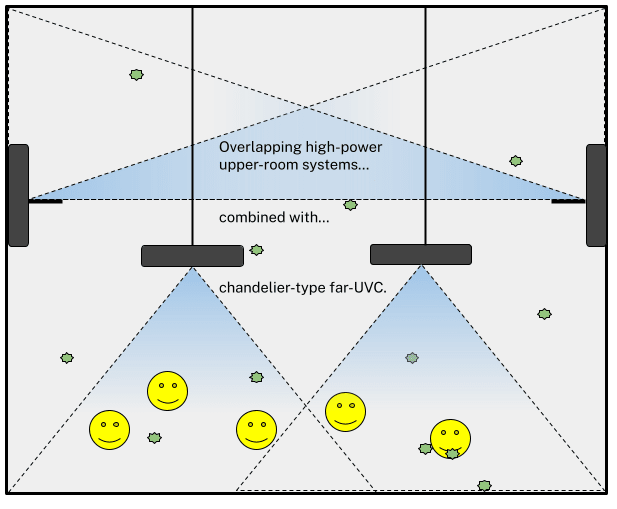
Imaginative deployment techniques using mixed wavelengths could help to cover different parts of the room in different ways:
Mixed-Wavelength Deployment with Upper-Room and Chandelier-Type Systems
(NB: The far-UVC lamps could also be deployed at the ceiling at high flux, such that the irradiation of the occupied zone is similar, but there is additional inactivation above the occupied zone. Far-UVC lamps could also be deployed as wall-mounted lights.[109])
Indeed, given uncertainty around the characteristics of potential threats — and the sensitivity of different pathogens at different wavelengths — a mixed approach may provide more threat-agnostic protection.
In summary, although the following sections attempt to compare different types of GUV, their ultimate comparison will depend on a variety of factors, including the dimensions of the relevant rooms. In addition to further investments in far-UVC research because of its safety benefits, more research is needed to map the different indoor spaces, their importance in transmission events, and their dimensions in order to fully understand which system is likely to be most promising in the long run. In other words, we cannot claim confidently that one wavelength or deployment method is universally better than another; this will depend entirely on deployment context. Ultimately, we expect that mixed deployment systems will dominate in large public spaces and that different users with different cultures, spaces, transmission-suppression priorities, and risk tolerances will adopt different systems (consider, for example, the differences between a neonatal ICU in a hospital and a tech company office). This is partly why we recommend real world studies and wavelength-agnostic funding.
Efficacy
All forms of GUV work to inactivate pathogens, in order to decrease infection rate; all systems also require some form of ventilation, and as discussed in the previous section, different use cases, different room sizes, and different priorities will likely determine which systems are most useful.
All else equal, is full-room far-UVC more effective than upper-room GUV in reducing infection risk? There are some mechanistic reasons to expect this to be the case; full-room far-UVC can cover a broader area than upper-room systems, and far-UVC can directly target the air between humans (e.g. when speaking, singing, etc.) However, this issue is more complex than we initially realized (outlined above under The Complexity of Comparing Different GUV Systems and Wavelengths). The researchers we interviewed for this project, Dr. Kenneth Wood and Dr. Ewan Eadie, expressed skepticism about the ability of full-room far-UVC lights to stop short-range transmission, although it may help with so-called “superspreader” events (notably, however, upper-room GUV could also help with these events).[110] Our best understanding is that far-UVC would only be able to significantly reduce short range transmission if deployed at a far higher power than is likely to be permitted.[111] There is some reason to believe that far-UVC full-room UV may have some advantages for tackling so-called global catastrophic biological risks, therefore. One additional reason for this is the “tunability” of full-room far-UVC. As mentioned elsewhere in this report, it may be possible in extreme circumstances to increase full-room far-UVC exposure dramatically (and above recommended levels during non-crisis situations), whereas upper-room systems have a ceiling on effectiveness determined by air flow.[112]
While our belief is that full room far-UVC is probably more effective than upper-room systems, we think that this question is difficult or impossible to answer (with a reasonable degree of certainty) without more work to understand real-world transmission and the relative effectiveness of different kinds of GUV, including 222 nm light, and without specifying the deployment context. So far, although there have been transmission studies conducted with 254 nm upper-room GUV—and even these studies are quite different from real-world usage — there is only one ongoing real-world transmission study with full-room 222 nm light, which we discussed with the lead investigator, Kenneth Rockwood. This means that we simply do not have good information on how big the effect size difference really is. It also means that catalyzing a research program around real world GUV effectiveness could be among the most important things that philanthropists can fund. We discuss one pathway for cost-effectively funding such studies — policy advocacy for a research funding program, rather than individually funding studies — below, under Potential Funding Pathways.
The Challenges of Studying Real-World GUV EffectivenessThroughout this report, we recommend funding policy advocacy for a research program around the effectiveness of GUV (and the advantages of different wavelengths of UVC) in reducing transmission in the real-world. There are, however, many challenges associated with “real-world” effectiveness studies, several of which are outlined by Don Milton in a presentation at the first International Congress on Far-UVC Science and Technology.[113] The challenges outlined by Milton include:
We believe that some of these problems could be addressed with larger scale research programs. These may require government investment and resources (e.g. in VA hospitals), which is one reason we recommend policy advocacy. More broadly, however, studying real-world effectiveness could be a multi-pronged approach, including:
|
Nonetheless, we can attempt to estimate any potential differences in efficacy. We note that infectious disease transmission is a highly complex issue, and transmission rates may depend on factors such as the infectious dose of a pathogen, human behavior, and environmental factors.[114] As such, these estimates are rough and carry considerable uncertainty.
First, according to some estimates, full-room far-UVC GUV can achieve about 128-322 eACH whereas standard upper-room GUV achieves 24-100 eACH (for comparison, “comfort” ventilation achieves about 1-2 eACH, high-risk hospital rooms about 6-12 eACH, and most HVAC systems currently installed cannot achieve more than 6 eACH — part of the problem is that these systems are “flow limited”).[115] At first blush, these differences appear large:
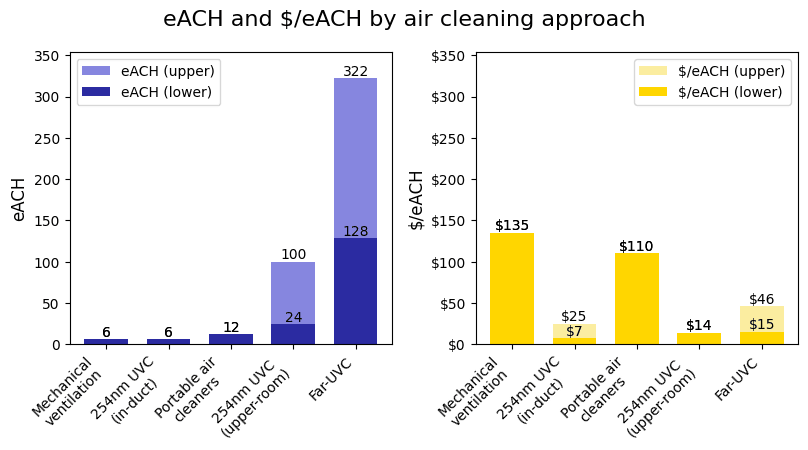
Source: 1DaySooner, shared by Vivian Belenky.
There are two problems with such a comparison, however. The first problem is the complexity described above: the comparisons depend entirely on a variety of factors, such as:
- Deployment context, like room height, ventilation, and more.
- GUV installation, including the possibility of mixed systems.
- Pathogen characteristics, including infectiousness and susceptibility to different wavelengths of UV light
The second problem is that even with simplifying assumptions, increases in room ventilation do not neatly translate linearly into decreases in disease transmission. The Wells-Riley equation — one simplistic but commonly-used way to model infection probability — suggests that the relationship between eACH and transmission is non-linear. In particular, one eACH removes about 63% of contaminants, but a second ACH removes 63% of what is left (i.e. a total of 86%) — in a situation where infectious agents are constantly being emitted, the calculation of how much of the contagion is actually removed on net thus becomes more complicated.[116]
The Wells-Riley equation gives the probability of infection in a well-mixed room as:
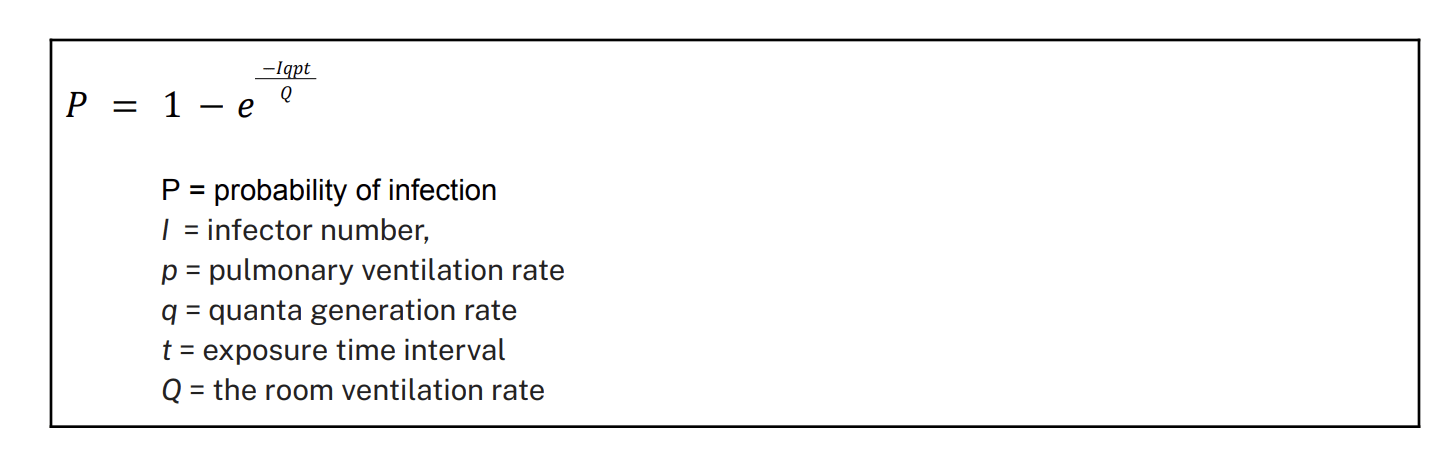
Q is measured in cubic meters per hour, such that we can represent eACH as , or . Taking this approach to generate the overall probability of infection for different forms of UVGI technology seems overly simplistic given the complexities outlined above, but a key takeaway emerges from the use of this basic model: the probability of infection decreases at a decreasing rate as room ventilation rate increases. On the one hand, this means that large gains in eACH may lead to relatively small gains in transmission reduction in controlled environments. On the other hand, at the epidemiological level, even marginal gains in transmission reduction could have large nonlinear effects, given how disease spreads through a population.[117] This means that reductions in transmission around R0 of 1 may be far more important than similar-sized reductions at higher R0 above 1. In short, the effectiveness of different wavelengths is once again highly complicated, and will once again ultimately depend on context, including the pathogen in question.
What other evidence exists? Another avenue to explore differences in efficacy comes from looking at existing data from infection rates and pathogen inactivation. Starting with upper room GUV, existing data suggests a ~70-80% reduction in infection transmission rates for TB as a result of this technology. For example, Escombe et al. showed a 77% reduction in human to guinea pig transmission in a hospital setting.[118] In a conceptually similar experiment, Mphaphlele and colleagues also found ~80% protection from upper room GUV,[119] despite considerable methodological differences between the two experiments.[120] Modeling studies (using rates of pathogen inactivation) have found broadly similar results, albeit with larger bounds; for example, Xu et al. (2005)[121] found rates of ~60% and 95% pathogen inactivation at relative humidity levels of 25% and 50% respectively, with a 6 air change per hour ventilation rate for Mycobacterium parafortuitum. These figures may seem high, but note that upper room GUV can decontaminate large volumes of room air at one time; for example, the upper two feet (22% of room volume) of a room with a nine-foot ceiling.[122] However, Kowalski (2009)[123] tabulated real-world upper-room GUV studies and found a lower median infection reduction rate of 39%; our best understanding is that this variation is because Kowalski considered a wider range of more challenging scenarios (the GUV performed close to 100% in ideal scenarios, but relatively poorly in high-challenge scenarios).[124]
Overall, we expect that the modeling studies may overestimate the efficacy of upper room GUV somewhat, due to (1) the effect of direct transmission through speaking and coughing, which are not explicitly modeled out/possible to examine within the experimental data here, and (2) a general assumption that real-world set-ups will be less efficient than experimental set-ups. This implies that upper-room setups might lower infection rates by (very roughly) ~35-80% dependent upon the pathogen and situation at hand. Importantly, these rates may be on the lower end for high-challenge scenarios (such as an especially virulent pathogen).
There is not yet existing data on infection rate for full room irradiation. However, in one experiment in the Leeds Chamber, UK, researchers put out aerosolized Staph. Aureus (constantly emitted, rather than one-time, to simulate a situation analogous to breathing, coughing, etc.) at a room ventilation rate of 3 air-changes-per-hour.[125] Despite using a lower air change ventilation rate relative to Xu’s modeling study above, and despite the fact that Staph. Aureus is more resistant to UV light than coronaviruses and influenza viruses,[126] Eadie found a reduction in viable pathogen load of 98.4% compared to ventilation alone, when using 5 lamps in a room measuring 32 Within a slightly lower exposure (designed to be below ICNIRP guideline exposure limits) a ~92% reduction in viable pathogens was demonstrated. If we assume that this will roughly parallel transmission rates (a significant assumption that might be incorrect, but note that work from upper-room studies found broadly similar estimates when modeling pathogen inactivation rates versus experimentally assessing transmission rates) this suggests that experimental studies of transmission reduction will also found an effect of ~92%.[127] While we think this is promising, it is very unclear to us (in the absence of better understanding of real-world transmission reduction) how this effect on pathogen activation will translate to infection rates.
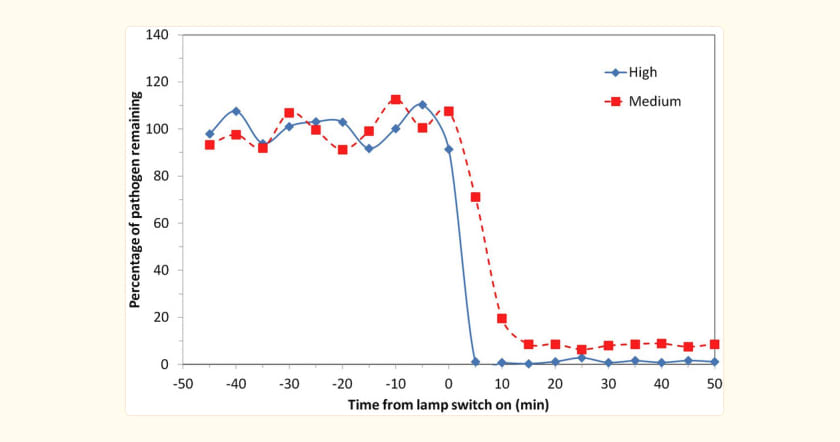
Fig 1: percentage of viable S. aureus remaining plotted on a linear y-axis for two exposure scenarios. The pathogen was continuously released into the room through the experiment, with a mechanical ventilation rate of 3 air changes per hour.[128]
All else equal, we therefore think that full-room irradiation is likely to be more effective than upper-room systems— depending on the specific deployment context —perhaps especially for high-challenge scenarios (such as highly virulent pathogens) that characterize the most threatening catastrophic biological risks. At the same time, we have significant uncertainty here, and highlight that upper-room systems nonetheless appear to be an effective method of improving biological air safety. Given the importance of air safety and remaining uncertainty around far-UVCsystems, we don’t think that these efficacy considerations imply that funders should neglect upper-room GUV systems—for example, funding upper-room systems might be a critical “hedge” if usable full-room or far-UVCsystems fail to materialize.
Safety
We divide our discussion into two parts: skin/eye safety and indoor air pollution.
Skin/Eye Effects
Upper room GUV and in-duct GUV have some theoretical safety advantages over full-room GUV; when installed and used properly, human contact with the UV light is minimized (although leakage and accidents occur). Upper-room GUV with 254 nm light has been used for nearly 100 years (e.g. in hospital settings), with no apparent major health implications, but importantly, this is not necessarily representative of the use cases for pandemic prevention. Safety risk comes from leakage, incorrect installation, and accidental exposure to upper-room 254 nm UVC light, which can cause temporary but painful photokeratitis (akin to “snow blindness”) of the eye, and temporary but painful erythema (reddening) of the skin.[129]
As discussed above, we think the available evidence suggests that far-UVC light is safe—but there is a small chance of health risks that cannot yet be ruled out, due to the lack of population-based studies or longterm studies. In particular, we think it is possible that there may be certain groups within the population that are especially vulnerable to far-UVC light. For example, we think it is currently unclear whether people who are especially prone to skin reactions from UV light, or those who have unusual eye physiology (i.e. suffer from dry eye), might suffer health problems as a result of its use—we are not sure whether the mechanistic evidence holds for these groups of the population, and we are not aware of any experimental evidence that speaks to this possibility. Second, we think that there have thus far been very few studies on the effects of far-UVC light upon eyes in general.
Indoor Air Pollution
As discussed in detail above, researchers have recently raised the prospect that UVC light may have adverse effects on indoor air quality by producing pollution, and that this is more concerning for far-UVC light. So far, the indoor air pollution concerns are based on computer models alongside some mechanistic evidence, but we do not have high confidence in the validity of these models — more real-world studies may be needed.[130]
Cost
One unpublished study by a Russian academic and a CDC researcher allegedly estimated that the cost of 1 ACH by ventilation is about $135.91 USD and by GUV is about $14.44 USD.[131] 1DaySooner and Rethink Priorities have estimates that "The price of current systems is currently too high for at-scale deployment, though there are reasons to think the price can be lowered significantly;" they estimate that the cost of upgrading all U.S. buildings for improved indoor air quality would be about $120 billion - $420 billion.[132] Our best understanding is that far-UVC light cost is dropping quickly, can fall further, and may become cheaper than 254 nm upper-room light when total installation costs are included.[133] There are, however, countervailing factors that may increase the cost of widespread installation of far-UVC lights even if market factors were more favorable. These include:
- The costs associated with far-UVC light’s potential production of air pollution (installing additional filtration/ventilation systems);[134]
- The costs associated with far-UVC light’s potentially degrading effect on plastics.
In “Air Safety to Combat Global Catastrophic Biorisk,” the authors have compiled rough current cost-effectiveness estimates of various indoor air quality interventions:
1DaySooner and Rethink Priorities Cost-Effectiveness Estimates[135]
1DaySooner and Rethink Priorities ‘Air Safety to Combat Global Catastrophic Biorisk’ report includes estimates of the cost of different air quality measures; see figure below. We note one important caveat for far-UVC (noted within this report), which is that rooms outfitted with far-UVC may also need appropriate ventilation or filtration to limit harm from pollutants (see ‘Indoor Air Pollution’ section above). Our best understanding is that a small amount of ventilation (>1ACH) or filtration is needed for the effectiveness of most GUV systems (potentially limiting their applications to commercial and public buildings rather than lower-ventilation private homes).[136] Again, the same graphic as above:
Source: 1DaySooner, shared by Vivian Belenky. Notably, these effects depend on a variety of factors, including the pathogen in question.
Limits to real-world use
There are a number of real-world factors that will limit where far-UVC versus upper-room GUV can be successfully implemented, which could be important. For example, if it is the case that far-UVC light can be successfully installed in twice as many places as upper-room GUV, this would make it more likely—all else equal—that far-UVC would be more impactful.
- Room height: upper-room UVC requires that the room is high enough that the machines can be installed such that there is no risk that the beams will come into contact with people. This appears to be a critical consideration; researchers wanted to test different kinds of UVC lights in school systems in Bradford, England, and had originally planned to install upper-room GUV in ten schools, but were ultimately only able to install them in two schools, because the other rooms were unsuitable for upper-room GUV.[137]
- Ventilation: upper-room UVC requires sufficient ventilation that air travels to the upper levels of the room. It is common to install a fan to ensure this[138] but there may be rooms where it is impossible to ensure adequate ventilation.
- Shadows: far-UVClight will not hit areas that (from the perspective of the far-UVClamps) are in shadow. This is likely to be mostly an issue with surface disinfection (rather than airborne transmission, the focus of this report) which could itself be managed by ensuring that lamps shine from different directions, but nonetheless might be a problem in some rooms.
- Humidity: a common finding in the literature is that there are decreases in the UV-inactivation rate with increasing humidity, at least for upper-room UV.[139] As far as I am aware, there is no data examining the effect of humidity upon UV-inactivation from full-room irradiation.[140] While the effects of humidity upon UV-inactivation are relatively poorly understood, humidity in the air can affect the absorption and scattering of far-UVC light in the air, potentially diminishing its effect.
Additional benefits
Skin-safe GUV (such as far-UV) could additionally be used during hospital procedures, for example to combat the spread of antibiotic-resistant bacteria. This is because it is possible to use far-UVC light during procedures without damaging skin (e.g. via handheld devices), to disinfect the air during procedures and prevent re-aerosolized bacteria entering the wound. While the focus of this investigation is the potential role of GUV for pandemic prevention, this may be an additional benefit of far-UVC compared to other GUV systems.
Overall View
To summarize key points from above, our overall view of this comparison is:
- There are mechanistic reasons and some experimental evidence to believe that far-UVC is safe, but more safety studies are needed both to reduce real uncertainties (eyes, long-term exposure, vulnerable populations) and to bolster public confidence.
- There are mechanistic reasons to believe that full-room far-UVC irradiation would be more effective at reducing transmission, but the magnitude of the effect at different exposure limits remains highly uncertain. More research on real-world effectiveness are needed.
- Far-UVC remains much less cost-effective today, but it could become competitive with conventional UVC technology.
- Key uncertainties remain about far-UVC technology, including its potential to increase indoor air pollution. These externalities and the necessary measures to mitigate them may push against future cost-effectiveness of far-UVC technology.
- Widespread adoption of conventional upper-room GUV may significantly reduce the global burden of airborne disease and may provide significant pandemic-preparedness benefits against all but the most virulent engineered pandemics.
In short, we are optimistic about the promise of far-UVC technology, but believe that uncertainty remains too high to pick winners. This points towards a wavelength-agnostic approach to funding GUV, described in greater detail below.
Questions for Further Investigation
|
Neglectedness
Key Points
|
Assessing the overall neglectedness of GUV as a philanthropic intervention is challenging, but literature review, stakeholder interviews, and searches of public funding information suggest that GUV remains highly neglected as a pandemic prevention intervention relative to its importance, despite a recent flurry of interest in far-UVC technology.
Over the past three years, several other research and grantmaking organizations interested in pandemic preparedness and global health have studied indoor air quality and specifically GUV. These include:
- 1DaySooner (e.g. “Air Safety to Combat Global Catastrophic Biorisk” with Rethink Priorities);
- Convergent Research;
- Longview Philanthropy (e.g. far-UVC event with Kevin Esvelt and David Sliney, supported by Open Philanthropy);
- Open Philanthropy (various grants, e.g. to Columbia University on far-UVC);
- Pacific Northwest National Lab
- Rethink Priorities, (e.g. “Air Safety to Combat Global Catastrophic Biorisk” with 1DaySooner)
There has also been capital influx from non-philanthropic funders, to companies using GUV technology such such as RZero, LumenLabs and Lit Thinking.
Within much of this work, the focus has often been explicitly on far-UVC technology. For example, all GUV-relevant grants listed in Open Philanthropy’s grants database — $3,425,000 in total — focus on far-UVC (Open Philanthropy is one of the largest funders of biosecurity interventions).[141]
From speaking with experts in the field and surveying the ongoing research projects, our best guess of the amount of money spent on far-UVCresearch is around $3-4 million, with <$2million coming from industry. We are unsure what amount is spent on upper-room systems, but suspect recent philanthropic investment has concentrated on far-UVCsystems. A 90% confidence interval on the annual amount of funding for GUV safety and efficacy research is between $500,000 and $5,000,000.[142] This latter estimate does not include private for-profit investment in GUV systems, which is much larger and growing (though notably still focused on applications like water purification and food irradiation).[143]
GUV appears to be neglected in several post-COVID pandemic preparedness policy documents and proposals. It is not explicitly mentioned in the Apollo Program for Biodefense, although the Commission does address “Pathogen Transmission Suppression in the Built Environment” broadly.[144] The recent Delay, Detect, Defend Geneva Paper by Dr. Kevin Esvelt does specifically call out far-UVC technology as a passive defense.[145] The Biden Administration’s American Pandemic Preparedness Plan (AP3) focused largely on medical countermeasures, only very briefly mentions pathogen transmission in the built environment, and does not mention GUV specifically.[146] In the absence of better data on neglectedness, we may use AP3 as a rough proxy measure of the amount of attention that GUV receives in current pandemic preparedness planning.[147] AP3 would have allocated USD 3.1 billion to point 8, “Personal Protective Equipment,” which has two items:
- 8.1 Promote next-generation PPE innovation
- 8.2 Enhance pathogen protection in the built environment
For simplicity, we assume that AP3 would have allocated 50% of the 3.1 billion to point 8.2, and within that 50% to GUV-related interventions, so $775 million. This would be about 1.2% of the total $65.3 billion in the plan; given how much indoor air quality improvements could reduce pathogen spread relative to other interventions like medical countermeasures, this appears to have been a severe underinvestment. Of course, the AP3 was never implemented, but the Administration has since then highlighted indoor air quality as an important area for pandemic preparedness, including by hosting the Clean Air in Buildings Challenge, hosting a White House Summit on Indoor Air Quality and outlining key actions on indoor air quality.[148] The December 2022 Indoor Air Quality Fact Sheet, however, only briefly mentions GUV, in point 2 as an emerging air quality technology, and in point 4 as one of the systems schools can purchase and install using funding provided through the American Rescue Plan; the majority of the document highlights ventilation and filtration.[149]
In part, we can also look to scientific and regulatory attitudes towards airborne disease to form rough estimates of neglectedness. From the Rethink/1DaySooner report:
“Prior to COVID-19, the dominant public health paradigm treated airborne transmission as negligible for most major respiratory diseases. This resulted in a historical reluctance to implement air hygiene controls. However, interdisciplinary research inspired by the COVID-19 pandemic has shown that airborne transmission is a major mode of transmission for this disease, and likely a significant one for many other respiratory infectious diseases.”[150]
Questions for Further Investigation
|
What Could a Philanthropist Do?
Key Points
|
In short, despite some remaining uncertainties, we believe that GUV is a promising and under-funded intervention on the large-scale problem of reducing airborne transmission of infectious diseases, with potential applications for the most high-consequence events — global catastrophic biological risk. This section turns to the question of what philanthropists can do to support progress on GUV.
The section is divided into two sub-sections. The first, Grantmaking under Uncertainty: Impact Multipliers for GUV, outlines possible features of the world and attributes of interventions that may make some funding opportunities relatively more cost-effective than others. The second, Specific Funding Options, outlines and evaluates several possible grantmaking strategies based on these impact multipliers.
Grantmaking under Uncertainty: Impact Multipliers for GUV
When facing high uncertainty about absolute cost-effectiveness of interventions, philanthropists can focus on relative cost-effectiveness via impact multipliers, features of the world that make one intervention relatively more cost-effective than another. For example, in global health and development, one impact multiplier is simply focusing on the world’s poorest people; because of the large wealth and income inequalities and the decreasing marginal utility of money, a dollar spent in the poorest areas of the Global South can do much more good than a dollar spent in the richest areas of the Global North. Identifying multiple impact multipliers and multiplying them together can point philanthropists towards funding opportunities that are orders of magnitude more effective than others.
Other Founders Pledge research has used impact multipliers to narrow the field of funding opportunities. In nuclear security, we have identified “right-of-boom” interventions as funding opportunities that simultaneously are unduly neglected and are critical for targeting the most high-consequence types of nuclear war.[151] In climate change, too, considerations about the non-linearity of climate damage, the leverage of policy advocacy, and the neglectedness of some unpopular types of interventions inform Founders Pledge’s grantmaking strategy.[152]
Here, we outline several possible impact multipliers for philanthropists interested in GUV. We do not believe that these are exhaustive, but rather that they are sufficient for separating the wheat from the chaff of funding opportunities and thus narrowing the option space to increase the probability of having a high impact per dollar spent.
Potential impact multipliers include:
- Placing wavelength-agnostic bets — Uncertainty on the relative cost-effectiveness of different wavelengths of GUV remains high; philanthropists ought not focus on one wavelength to the detriment of another (at least until there is stronger evidence that a particular technology is more likely than the other to reduce pandemic risk—a region that we don’t believe we yet reached);
- Leveraging societal resources via advocacy — As in many areas, the vast resources of governments (money, talent, and regulatory power) can multiply the impact of private funds. Moreover, the large amounts of philanthropic money spent on health research is also an attractive target for advocacy;
- Prioritizing shaping R&D incentives over funding specific R&D — Attempting to “pick winners” and directly fund technological R&D is likely less efficient than shaping incentives for increased R&D, and perhaps for incentives aimed at better coordinating R&D;
- Focusing on high-income countries first — Geographically, we believe that the highest impact is likely to be found via philanthropic investment in high-income countries like the United States;
- Focusing on public perception over rapid deployment — Because there is a risk that negative public perception will permanently curtail future adoption of promising UVC technology, and because catastrophic biological risks are relatively rare, small accelerations in adoption speed are likely not worth sacrificing public perception.
Currently, we do not have sufficient information to quantify these multipliers, a task for further research. Thus, they serve mostly as guidelines for philanthropists to navigate the uncertainties surrounding GUV.
Placing Wavelength-Agnostic Bets
As described above, there remain key uncertainties about the differences between 254 nm UVC light (as upper-room fixtures) and 222 nm far-UVC light (as full-room irradiation). These uncertainties may be large enough to affect the relative cost-effectiveness of each wavelength. As described above, some funders appear to have gone “all in” on far-UVC light. We believe that this approach is misguided and that far-UVC may be an over-hyped technology; we don’t think the evidence for superiority of far-UVC (relative to other GUV systems) is overwhelmingly strong as to outweigh the risks of focusing specifically upon this technology. Nonetheless, far-UV’s novelty and uncertainty also gives it a potentially higher ceiling than conventional GUV, and may allow it to avoid some of the obstacles that have prevented widespread adoption of conventional GUV.
Hence, we think that philanthropists ought to not “pick winners” prematurely, but instead fund interventions that:
- Reduce uncertainty about absolute and relative cost-effectiveness of different GUV interventions;
- For example, see our recommendation for policy advocacy for more research on real-world effectiveness, below.
- Preserve option value by not focusing on the exciting new technology when the proven 254 nm light may be a valuable intervention, and;
- Leave options open by not committing to one option to the potential detriment of the other. For example, one potential ‘failure mode’ would be if far-UVCwas rolled out too early, resulting in a public backlash against GUV systems more broadly.
Note that the importance of leaving options open runs both ways: there may be a risk that investments in 254 nm light either “lock in” an inferior technology or “poison the well” for the entire class of GUV.[153] That is, it is possible that:
- Widespread adoption of 254 nm light goes well, but is “locked in” (as other inferior technologies have been locked in before) even if far-UVC light turns out to be better.
- Attempted adoption of 254 nm light results in accidents (e.g. due to incorrect installment or use) that lead to a public backlash against all kind of GUV.
We therefore generally advocate against rushed deployment of any wavelength of GUV, towards a truly wavelength-agnostic approach. As we write below, small accelerations in adoption timelines are unlikely to be worth the risk of lock-in or backlash, given the infrequency of catastrophic pandemics.
If we believe, for example, that it is 60% likely that far-UVC technology is meaningfully more cost-effective than 254 nm upper-room GUV, but 40% likely 254 nm technology is equal or superior, we would want to identify interventions that don’t close the door to this 40% of impact.
Such interventions might include:
- Studies around real-world effectiveness that study the absolute and relative effectiveness of different wavelengths of UVC light (potentially funded via policy advocacy to fund a large group of such studies using public funds);
- Safety studies that seek to better understand the air pollution concerns, and how much they apply to different wavelengths of UVC light;
- General GUV policy advocacy, without reference to far-UVC light;
- Public perception work, about GUV technology broadly (not focused on a particular wavelength).
Wavelength-agnostic interventions would likely exclude:
- Attempts to accelerate far-UVC technology only (e.g. private investments in solid-state far-UVC sources);
- Policy advocacy that focuses on pushing far-UVC technology to the exclusion of other GUV, without further evidence on transmission reduction and safety.
We do note that there are areas where research funding is needed to ‘bring one wavelength up to speed’ with the other; for example, we are far more uncertain about the safety of far-UVC relative to upper-room GUV systems. We don’t think that this is against a wavelength agnostic approach, since this work would entail reducing uncertainty about the impact and cost-effectiveness of different US systems rather than advocating for one over the other. However, we suspect that philanthropists are likely to be more impactful by operating at the meta-level (i.e. advocating for more funding for researchers to examine this) rather than by attempting to fund these safety studies directly—see below.
Leveraging Societal Resources Via Advocacy
The second impact multiplier is leveraging government resources via policy advocacy. One recent analysis estimates that the cost of upgrading indoor air quality technology in U.S. public buildings is between $120 and $420 billion; far beyond the capabilities of even the largest philanthropists.[154] Our current understanding is that—while the UK and US governments have made some investments into GUV research, via the NIH and programs such as UKRI—air quality interventions receive a small quantity of funding relative to their potential to reduce disease/pandemic risk, potentially reflecting historical assumptions that airborne transmission is of negligible importance to the transmission of major respiratory diseases.[155]
As in climate change, therefore, philanthropists ought to use the leverage that vast government resources can provide via policy advocacy — redirecting defense spending and public health spending towards promising causes like UVC safety research. Moreover, some of the largest philanthropic funders in the world — like the Wellcome Trust and the Gates Foundation — focus on health; advocacy can also help to leverage these funds.
Prioritizing shaping R&D incentives over funding specific R&D
Third, philanthropists ought to prioritize shaping incentives for research and development (R&D) in GUV over funding specific R&D and technical projects. Specific technical projects may be appealing to grantmakers because they have “tangible” outcomes. In our research, we learned about several specific technical projects — like funding particular more efficient far-UVC technology projects. However, we are skeptical about whether philanthropists have the technical expertise to “pick winners” among different R&D projects, and think they ought to cast their net wider; we think that it may be possible to increase the quality and quantity of this research by shifting incentive systems, and that this approach could be very high impact. For example, it may be possible to use market-shaping incentives to increase private R&D (i.e. by underwriting commitments from companies to buy these technologies if they become cost-effective, as suggested to us by 1DaySooner-thus providing enhanced incentives for developers). Other ideas include incentivising companies to use far-UVC and share their data, and to promote/ incentivise efficient coordination of research across different research groups.
Overall, we believe that stimulating private R&D via regulatory levers, public funding, using funding incentives for well-coordinated research, and innovative market-shaping incentives is likely to be far more effective than trying to fund specific technologies.
Focusing on high-income countries first
Fourth, to narrow down funding options geographically, we believe philanthropists ought to target interventions in high-income countries like the United States first — at least for full-room far-UVC(we are less sure whether this holds for upper-room systems) . The reasons for this are outlined in the recent Indoor Air Quality report by Rethink Priorities and 1DaySooner, which provides reasons for scoping to the United States. We reproduce these reasons verbatim below:[156]
- “American standards tend to influence other countries (e.g. car emissions standards).”
- “Globally, 1.2 billion people live in high-income countries, for which deployment should be roughly similar to the US.”
- “We expect building changes to be implemented first in richer countries because of their greater resources and institutional capacity.”
- “People in high-income countries fly more often on average, so blocking or reducing pathogen transmission in these countries, including the US, would do more to reduce air travel spread”
- “Technological investments by wealthy countries will reduce costs, which would facilitate later deployment in developing countries.”
Notably, however, conventional upper-room GUV may be deployed easily in other countries, potentially helping to stimulate the global market for GUV generally.
Focusing on good information over rapid deployment
As discussed throughout this report, we believe that there is a risk that negative public perception will permanently curtail future adoption of promising UVC technology — including conventional GUV, where occasional accidents can cause major public backlash. Because catastrophic biological risks are relatively rare, small accelerations in adoption speed are likely not worth sacrificing public perception. Far-UVC GUV is a relatively new technology. While it may have a larger upside than 254 nm upper-room GUV, many unknowns — both known unknowns and unknown unknowns — remain about this technology.[157]
Other work on this issue has been explicitly framed around accelerating deployment of GUV. The recent 1DaySooner and Rethink Priorities report on indoor air quality explicitly mentions this risk: “Doing a poor job with the rollout of IAQ interventions or attempts at altering standards and regulations might ‘poison the well’ for better attempts later, e.g. due to a very small number of high-profile failures.”[158]
Global catastrophic biological risk is an urgent problem, but the difference between deploying GUV in 5 years or 25 years is not as large as it may seem. In one public forecasting tournament, crowdsourced predictions currently give the following probabilities:
- 38% chance of a 10% decline in the human population by 2100;[159]
- 14% chance that such a decline will be due to naturally-occuring pandemics;[160]
- 28% chance that such a decline will be due to “biotechnology or bioengineered organisms”[161]
Assuming that (2) and (3) are independent, we can estimate the chance of a catastrophic biological event at about 0.38*(0.14+0.28) = 0.1596, or a ~16% chance of a catastrophic biological event by the end of the century.
This is not, however, distributed uniformly across the next 77 years. As the forecasts above imply, experts believe that the majority of the risk’s mass is from biotechnology and bioengineered organisms rather than from naturally-occuring pandemics. As explained in a fourth forecasting question, “Since biotechnology is becoming more advanced and cheaper as time goes on, potentially faster than humanity's abilities to prevent pandemics, it is plausible that the time of greatest risk from bioengineering will be in the future.”[162] Moreover, as outlined in a recent policy report on catastrophic pandemics, “We don't yet know of any credible viruses that could cause new pandemics, but ongoing research projects aim to publicly identify them.”[163] All of this implies that risk is increasing; barring a shift in the offense-defense balance, we ought to be disproportionately more concerned about pandemics 20 years from now than pandemics 10 years from now than we would be assuming a uniformly-compounding risk every year. Experts we have interviewed on global catastrophic biological risk also expressed the belief that risk is increasing.[164] This suggests that we may wish to sacrifice a few years of accelerated deployment in favor of stable deployment (because there is no public backlash) over the rest of the century; see hypothetical graph below.
Note that we do have significant uncertainty here. We think that public acceptance is likely to increase with time, since (1) it is more likely that scientists will uncover any significant health risks prior to roll-out (e.g. therefore switching to upper room systems rather than far-UVC), and (2) there is more time for public acceptance measures to be run, via the media and other information sources. However, an argument going the other way is that people might be unusually accepting of such measures now, in the immediate aftermath of COVID. We also assume that pandemic risk will increase with time due to advancements in the accessibility of technology that enable the development of bioengineered pathogens, but it is also possible that this risk is higher in the immediate future (for example, if AI technology takes off quickly and regulations/ other measures to prevent the use of this technology for bioengineering pathogens come in later).
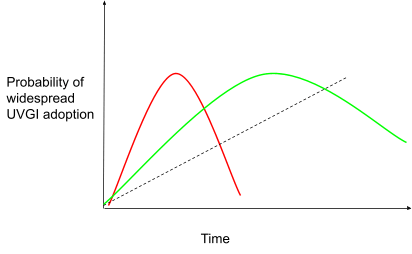
This graph shows our mental model of the potential risk of pushing rapid roll-out of GUV technology, prior to achieving public acceptance. Red line; hypothetical scenario of having quick roll-out, followed by a higher risk of backlash against GUV. Green line; hypothetical scenario of slower roll out, with lower risk of significant backlash. Dotted line; pandemic risk. In the green scenario, GUV is more likely to be in place during times with greater pandemic risk. This graph is not based on real data, but rather to demonstrate our mental model of the risk of pushing roll-out too quickly.
Potential funding pathways
Here, we give examples of specific funding options for philanthropists who seek to support GUV work.
- Fund policy advocacy, with the aim of leveraging government budgets for more safety and efficacy studies.[165] For example, funding influential think tanks to conduct research on the feasibility of GUV-related interventions could help catalyze government action.
- Specifically, we believe that the following intervention could be especially high-impact: Policy advocacy for research around real-world GUV transmission reduction
- As discussed above, a major bottleneck is an understanding of the actual differences in transmission (as opposed to pathogen load in an air chamber experiment) using different kinds of GUV light. Notably, as pointed out in the “Challenges to Studying Real World Effectiveness” box, above, understanding real-world transmission is a complex problem, and may require government resources and a multi-pronged approach that seeks to validate existing models of airborne transmission.
- Safety studies, too, could follow this model. We suspect that high-quality transmission studies could catalyze interest in more safety studies in a way that high-quality safety studies would not necessarily stimulate more investment in transmission studies, due to excitement about the intervention. We are highly uncertain about this.
- Rather than fund single studies directly, we recommend advocating for public funding of a larger group of studies. This not only provides leverage (by using much larger government funding pots), but also institutional credibility (and public relations benefits of showing that GUV is not just the purview of funders with certain worldviews).
- This could be done by funding think tanks and advocacy groups with credibility and track record on health security and pandemic preparedness.
- There are government-affiliated spaces that are well-suited for some trials, including but not limited to:[166]
- Military barracks (and bases generally), submarines, aircraft carriers, missile silos, and other military spaces;
- Space exploration-related environments, which already have a long-standing interest in rigorous disinfection protocols;
- Government-funded or -run hospitals (e.g., Veterans Affairs hospitals in the United States);
- Other spaces that allow for well-controlled experiments. Note that we strongly object to the use of experimental technologies in spaces where (often innocent) people are held against their will (prisons) and cannot meaningfully consent to being a participant in a trial.
- As discussed above, a major bottleneck is an understanding of the actual differences in transmission (as opposed to pathogen load in an air chamber experiment) using different kinds of GUV light. Notably, as pointed out in the “Challenges to Studying Real World Effectiveness” box, above, understanding real-world transmission is a complex problem, and may require government resources and a multi-pronged approach that seeks to validate existing models of airborne transmission.
- Specifically, we believe that the following intervention could be especially high-impact: Policy advocacy for research around real-world GUV transmission reduction
- Shape market incentives, with the aim of promoting private sector investment (and consequent R&D by companies developing GUV technology). One potential example of this comes from 1DaySooner’s plan to try and reduce the risk to companies seeking to invest in far-UVC (by underwriting commitments in the case that the technology does not become cost-effective)—they believe this is a key lever to enable the development of far-UVC technology. Other ideas are to use prize challenges for breakthroughs in GUV technology, or matching funds for corporate investment in GUV research.
- Fund media interventions, such as funding journalists to write about GUV work. We think this could be very cost-effective (especially given the previous success of the GCR grant to Vox for bioweapons reporting) but also note some risk for a negative impact if this work is poorly received by the public: it would be important that this work is of high quality. Nonetheless, we think the potential benefits of this would be twofold; increasing awareness among policymakers and funders (hence making policy change slightly more likely), and increasing public acceptance of these technologies. We could specifically focus on media outlets that we believe are likely to increase awareness of GUV among policymakers (i.e. by surveying experts on the U.S. Congress, Executive Branch, etc, to identity these outlets), and/ or that we think are most likely to increase the public’s acceptance of these technologies. We think there is some crossover here to Matt’s Information Ecology report, in terms of understanding how to best spread accurate information and encourage attitude change.
- Crucially, such an intervention ought to ensure that GUV not become a politicized partisan issue, which we believe may do more harm than good. Thus, a well-balanced portfolio of reporting that includes work from mainstream outlets perceived as center and center-right may be an important part of this advocacy.
- Directly fund safety and efficacy studies (including eye safety). We think this option is reasonable, but probably the one of the least impactful on this list; given that philanthropists are unlikely to have the technical expertise to effectively judge different research protocols, and that it appears to be possible to shape research incentives at the level above this kind of direct funding.
Questions for Further Investigation
|
Conclusions and Next Steps
GUV technology appears to be potentially highly impactful, yet indoor air quality interventions in general seems to have attracted relatively little interest from mainstream funders. This is despite the potential of these technologies to reduce pandemic risk (in the case of both natural and bioengineered pathogens). We therefore think that the GUV space as a whole is a promising area for philanthropic investment, and recommend proceeding to work to find specific FOs.
Within GUV, we do not think that far-UVC systems are clearly superior to other systems—we think they are likely to be more effective and may have a higher upside, but there are other factors that could limit their use (such as health impacts, whether they are real or merely perceived by the public, cost, and indoor air pollution risk). Consequently, we think there is benefit from ensuring a range of future options (such as potential roll-out of upper-room systems). We therefore suggest interventions that are ‘wavelength-agnostic’ rather than funding the promotion of one system in particular.
In particular, we highlight the potential impact of supporting journalistic work that provides awareness into GUV work, policy advocacy, and of shaping R&D incentives.
About Founders Pledge
Founders Pledge is a global nonprofit empowering entrepreneurs to do the most good possible with their charitable giving. We equip members with everything needed to maximize their impact, from evidence-led research and advice on the world’s most pressing problems, to comprehensive infrastructure for global grant-making, alongside opportunities to learn and connect. To date, they have pledged over $10 billion to charity and donated more than $950 million. We’re grateful to be funded by our members and other generous donors. founderspledge.com
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
“Catskill–Delaware Ultraviolet Water Treatment Facility, New York - Water Technology,” accessed August 29, 2023, https://www.water-technology.net/projects/catskill-delaware-ultraviolet-water-treatment-facility/.
- ^
In practice, many far-UVC systems may also be upper-room systems. Thanks to Vivian Belenky for this point.
- ^
The 254 nm peak is for traditional low-pressure mercury lamps. This may shift as technology changes. Thanks to Jake Swett for this point in a round of external reviews.
- ^
“… by using the complete described program of air quality interventions to address transmission in public spaces, overall transmission in the population can be reduced by 30-75%, with a median estimate of 52.5%.” Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 20, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view. Note though that this estimate does not appear to count for the efficacy of existing indoor air quality measures; as far as we understand, this estimate measures ‘reduction in population transmission as a result of adoption of air quality measures in all public spaces, relative to having no indoor air quality measures in place’.
- ^
Jose L. Jimenez et al., “What Were the Historical Reasons for the Resistance to Recognizing Airborne Transmission during the COVID-19 Pandemic?,” Indoor Air 32, no. 8 (2022): e13070, https://doi.org/10.1111/ina.13070.
- ^
For more, see Chia C. Wang et al., “Airborne Transmission of Respiratory Viruses,” Science 373, no. 6558 (August 27, 2021): eabd9149, https://doi.org/10.1126/science.abd9149.
- ^
Max Görlitz writes, for example, “Crucially, we don't know how well this translates into an actual reduction in total number of infections. Of course, on priors, you would expect a reduction in the number of airborne pathogens to result in reduced infection risk. Yet the real world is messy and a lot could depend on air circulation in the specific environment, transmissibility of the pathogen, susceptibility of people etc.” Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
- ^
As discussed below, however, such work may be challenging to do well, and has several downside risks. See Leveraging Societal Resources via Advocacy for more.
- ^
In the literature on GUV, it is sometimes defined as 200-230 nm, but emerging evidence suggests that 235 nm may be a more appropriate cutoff. Thanks to Vivian Belenky for pointing us to this detail.
- ^
“Due to its dramatically greater biological safety relative to germicidal UV-C, ‘low-wave’ light – which is somewhat misleadingly termed ‘far-UVC’ and deserves a more accurate moniker – could constitute an extraordinarily effective pandemic defence.” Kevin M Esvelt, “Delay, Detect, Defend: Preparing for a Future in Which Thousands Can Release New Pandemics,” Geneva Papers (Geneva Centre for Security Policy, 2022), 39, https://dam.gcsp.ch/files/doc/gcsp-geneva-paper-29-22?_gl=1*xm44p1*_ga*ODQxMDI0NjY4LjE2ODM2NTg5MTg.*_ga_Z66DSTVXTJ*MTY4MzczNTIzNi4yLjAuMTY4MzczNTIzNi4wLjAuMA..#page=49&zoom=100,0,0.
- ^
Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 15–27, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2789813/.
- ^
John Paget et al., “Global Mortality Associated with Seasonal Influenza Epidemics: New Burden Estimates and Predictors from the GLaMOR Project,” Journal of Global Health 9, no. 2 (December 2019): 020421, https://doi.org/10.7189/jogh.09.020421.
- ^
Edouard Mathieu et al., “Coronavirus Pandemic (COVID-19),” Our World in Data, March 5, 2020, https://ourworldindata.org/covid-deaths.
- ^
“Ragnarök Question Series: If a Global Catastrophe Occurs, Will It Be Due to Naturally Occuring Pandemics?,” November 24, 2021, https://www.metaculus.com/questions/8745/gc-caused-by-natural-pandemic-if-gc-occurs/.
- ^
Piers Millett and Andrew Snyder-Beattie, “Existential Risk and Cost-Effective Biosecurity,” Health Security 15, no. 4 (August 2017): 373–83, https://doi.org/10.1089/hs.2017.0028; “Ragnarök Question Series: If a global catastrophe occurs, will it be due to biotechnology or bioengineered organisms?,” https://www.metaculus.com/questions/1502/ragnar%25C3%25B6k-question-series-if-a-global-catastrophe-occurs-will-it-be-due-to-biotechnology-or-bioengineered-organisms/.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 2, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
“… by using the complete described program of air quality interventions to address transmission in public spaces, overall transmission in the population can be reduced by 30-75%, with a median estimate of 52.5%.” Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 20, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Philip Brickner et al., “The Application of Ultraviolet Germicidal Irradiation to Control Transmission of Airborne Disease: Bioterrorism Countermeasure,” Public Health Reports 18 (2003): 101, https://doi.org/10.1093/phr/118.2.99. Note that Anthrax spores do not appear to be as susceptible to GUV as other agents (ibid., 100); because weaponized Anthrax is not human-to-human transmissible, however, it is an unlikely candidate for a catastrophic biological event of global proportions.
- ^
Max Görlitz has made this same point, writing, “Far-UVC seems like the only technology we currently know of that has the potential to passively mitigate a future catastrophic pandemic before we even know it is happening.” Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
- ^
Edward A. Nardell, “Air Disinfection for Airborne Infection Control with a Focus on COVID-19: Why Germicidal UV Is Essential,” Photochemistry and Photobiology 97, no. 3 (2021): 493–97, https://doi.org/10.1111/php.13421.
- ^
Rethink Priorities and 1DaySooner made similar points in their “Air Safety to Combat Global Catastrophic Biorisks” report, arguing that US standards tend to influence other countries, building change may be implemented more easily in high income countries, and that people in high-income countries fly more often on average (do reducing pathogen transmission in these countries may be especially effective in reducing air travel spread). Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
W. J. Fisk, “The Ventilation Problem in Schools: Literature Review,” Indoor Air 27, no. 6 (2017): 1039–51, https://doi.org/10.1111/ina.12403.
- ^
- ^
Thanks to Jake Swett for this addition in an external round of reviews. CDC, “Improving Ventilation in Buildings,” Centers for Disease Control and Prevention, https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/improving-ventilation-in-buildings.html.
- ^
Gavriel Kleinwaks, Alastair Fraser-Urquhart, and Josh Morrison, “[Cause Exploration Prizes] Indoor Air Quality to Reduce Infectious Respiratory Disease,” Effective Altruism Forum, 2022, https://forum.effectivealtruism.org/posts/j4eTj9dGqzEC5LEzK/cause-exploration-prizes-indoor-air-quality-to-reduce.
- ^
N. Yamamoto et al., “Residential Air Exchange Rates in Three Major US Metropolitan Areas: Results from the Relationship Among Indoor, Outdoor, and Personal Air Study 1999-2001,” Indoor Air 20, no. 1 (February 2010): 85–90, https://doi.org/10.1111/j.1600-0668.2009.00622.x.Note that some buildings (such as hospitals, where there has been particular attention to minimizing infection rates) may have higher ACHs than this. For example, Gormley et al. state ‘in practice, most hospitals use 20-30 ACH for their operating rooms, with known anecdotal outliers using 40 ACH’.
- ^
Gavriel Kleinwaks, Alastair Fraser-Urquhart, and Josh Morrison, “[Cause Exploration Prizes] Indoor Air Quality to Reduce Infectious Respiratory Disease,” Effective Altruism Forum, 2022, https://forum.effectivealtruism.org/posts/j4eTj9dGqzEC5LEzK/cause-exploration-prizes-indoor-air-quality-to-reduce.
- ^
William Firth Wells and Gordon Maskew Fair, “Viability of B. Coli Exposed to Ultra-Violet Radiation in Air,” Science 82, no. 2125 (September 20, 1935): 280–81. The germicidal properties of light in general were discovered as early as 1877 (Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16.)
- ^
Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16.
- ^
Ernest Blatchley III et al., “Far UV-C Radiation: An Emerging Tool for Pandemic Control,” Critical Reviews in Environmental Science and Technology 53 (June 10, 2022): 1–21, https://doi.org/10.1080/10643389.2022.2084315.
- ^
Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16.
- ^
- ^
This is an important caveat. People can climb into irradiation zones (e.g. to switch regular lightbulbs or to clean), technicians can install the technology incorrectly, and leakage can cause some UV light to leak into the inhabited areas. Thanks to Vivian Belenky for this point.
- ^
- ^
This is an important caveat. People can climb into irradiation zones (e.g. to switch regular lightbulbs or to clean), technicians can install the technology incorrectly, and leakage can cause some UV light to leak into the inhabited areas. Thanks to Vivian Belenky for this point.
- ^
Thank you to Vivian Belenky for making this point to us. See this EA forum post from Jesse Smith.
- ^
David Welch et al., “Far-UVC Light: A New Tool to Control the Spread of Airborne-Mediated Microbial Diseases,” Scientific Reports 8, no. 1 (February 9, 2018): 1, https://doi.org/10.1038/s41598-018-21058-w.
- ^
David Welch et al., “Far-UVC Light: A New Tool to Control the Spread of Airborne-Mediated Microbial Diseases,” Scientific Reports 8, no. 1 (February 9, 2018): 1, https://doi.org/10.1038/s41598-018-21058-w. Note that shorter wavelength light has higher energy than longer wavelength light, allowing it to penetrate more deeply into different materials. Existing evidence suggests that the specific wavelength—and thus energy—of Far-UVC light (207nm -222nm) allows it to penetrate only the outermost layer of the skin and eyes, where it cannot generate the kind of DNA damage associated with shorter wavelength UV light (such as UVA, UVB and UVC).
- ^
https://knowablemagazine.org/article/health-disease/2022/how-fight-covid-with-light
- ^
“Effective air disinfection in the breathing zone then depends on good vertical air movement between the upper and lower room, which can be generated naturally by convection, the HVAC system, or low-velocity paddle fans where needed.” Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16. Thanks to Richard Williamson for pointing out the possibility that human radiant heat may play an important role in air flow.
- ^
“... in-duct GUV irradiates the entire cross-section of a duct at high intensities not accessible to room occupants, and may include the use of highly UV-reflective materials to further increase irradiance levels.” Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16.
- ^
“Effective room air disinfection depends on circulating maximal room air through the duct and the velocity at which it is circulated.” Nicholas G. Reed, “The History of Ultraviolet Germicidal Irradiation for Air Disinfection,” Public Health Reports 125, no. 1 (2010): 16.
- ^
Thanks to Jake Swett for all the points in this paragraph in a round of external reviews.
- ^
Several of these benefits apply to all built-environment pathogen transmission suppression interventions, as outlined in the final report of the Apollo Program for Biodefense: “Suppressing pathogen transmission, especially in high-risk and high-traffic spaces, would reduce the spread of infectious diseases, extinguish some outbreaks, and buy critical time to combat more aggressive pathogens. With permanent incorporation into the environment, we could continuously defend against threats, even prior to detection, and without the dramatic changes in human behavior needed to reduce pathogen transmission.” (“Pathogen Transmission Suppression in the Built Environment” in Apollo Program for Biodefense (Final Report), Appendix A, 23, https://biodefensecommission.org/wp-content/uploads/2021/01/Apollo_report_final_v8_033121_web.pdf. )
- ^
“Far-UVC seems like the only technology we currently know of that has the potential to passively mitigate a future catastrophic pandemic before we even know it is happening.” Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
- ^
Thanks to Matt Lerner for this point in a round of external reviews.
- ^
Thanks to Jake Swett for these points in a round of external reviews.
- ^
This does not necessarily mean that far-UVC systems themselves are considered unacceptable – they could be installed as upper-room GUV, with small but significant safety improvements. On the other hand, ozone generation from far-UVC systems complicates upper-room installation significantly, potentially to the point of not being viable as an intervention (with thanks to Richard Williamson for this point in a round of external reviews). Note that we would place a higher likelihood on the potential for minor skin or eye irritation effects in small segments of the population.
- ^
In our view, analyses that flippantly dismiss these safety concerns because of the apparent physical properties of light in these wavelengths may do more harm than good from a public communications perspective.
- ^
See, e.g. Justen et al., “Accelerating Far-UVC Safety Science to Combat Infectious Diseases.” (Submitted) and Maximilian Görlitz et al., “Assessing the Safety of New Germicidal Far-UVC Technologies,” Photochemistry and Photobiology, accessed November 21, 2023, https://doi.org/10.1111/php.13866.
- ^
‘Towards the Responsible Deployment of Far-UVC for Infection Control’, a drafted paper by Justen et al.
- ^
https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months#Safety
- ^
Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
- ^
Manuela Buonanno et al., “207-Nm UV Light - A Promising Tool for Safe Low-Cost Reduction of Surgical Site Infections. I: In Vitro Studies,” PLOS ONE 8, no. 10 (October 16, 2013): e76968, https://doi.org/10.1371/journal.pone.0076968
- ^
Isla Rose Mary Barnard, Ewan Eadie, and Kenneth Wood, “Further Evidence That Far-UVC for Disinfection Is Unlikely to Cause Erythema or Pre-Mutagenic DNA Lesions in Skin,” Photodermatology, Photoimmunology & Photomedicine 36, no. 6 (2020): 476–77, https://doi.org/10.1111/phpp.12580; R.p. Hickerson et al., “Minimal, Superficial DNA Damage in Human Skin from Filtered Far-Ultraviolet C,” British Journal of Dermatology 184, no. 6 (2021): 1197–99, https://doi.org/10.1111/bjd.19816.
- ^
To put “minimal damage” into perspective, one model suggests that 10 minutes of sunlight on a sunny day in a temperate climate causes about the same amount of damage as 30,000 hours of exposure to properly filtered far-UVC light. In other words, if an average human were to live to about 70 years indoors under constant far-UVC exposure, and then were to spend the last 4 hours of their life outside enjoying a sunny day, they would incur more skin damage from the sun than from the filtered UVC lights.
- ^
With thanks to Dr. Ewan Eadie and Dr. Kenny Wood for explaining the importance of filtering KrCL lamps. For a discussion of the problem of unfiltered KrCl lamp-produced UVC light, see Paul O’Mahoney et al., “Potential Harm to the Skin from Unfiltered Krypton Chloride ‘Far-Ultraviolet-C’ Lamps, Even below an Occupational Exposure Limit,” Journal of Radiological Protection 42, no. 4 (November 2022): 043501, https://doi.org/10.1088/1361-6498/ac9e60.
- ^
‘Towards the Responsible Deployment of Far-UVC for Infection Control’, a drafted paper by Justen et al. Once published, we think that this paper will provide a more comprehensive overview of the safety concerns around far-UVC for the interested reader.
- ^
Thanks to Richard Williamson for this point in a round of external reviews.
- ^
Kaidzu, S., Sugihara, K., Sasaki, M., Nishiaki, A., Ohashi, H., Igarashi, T., & Tanito, M. (2021). Re‐evaluation of rat corneal damage by short‐wavelength UV revealed extremely less hazardous property of far‐UV‐C. Photochemistry and Photobiology, 97(3), 505-516.
- ^
Thank you to Richard Williamson for this point in a round of external reviews.
- ^
Kenneth Rockwood, “Do Far-UVC Light Devices Reduce the Incidence of Influenza-Like Illnesses, Respiratory Illnesses, and COVID-19 Infections in Long-Term Care Facilities?,” Clinical trial registration (clinicaltrials.gov, October 6, 2021), https://clinicaltrials.gov/ct2/show/NCT05084898.
- ^
Rockwood.
- ^
Note though that the lamps will only be installed in communal areas, which might limit the study’s ability to assess the impact of the far-UV lights
- ^
Holger Claus, “Ozone Generation by Ultraviolet Lamps†,” Photochemistry and Photobiology 97, no. 3 (2021): 471–76, https://doi.org/10.1111/php.13391.
- ^
Holger Claus, “Ozone Generation by Ultraviolet Lamps†,” Photochemistry and Photobiology 97, no. 3 (2021): 471–76, https://doi.org/10.1111/php.13391.
- ^
Zhe Peng, Shelly L. Miller, and Jose L. Jimenez, “Model Evaluation of Secondary Chemistry Due to Disinfection of Indoor Air with Germicidal Ultraviolet Lamps,” Environmental Science & Technology Letters, December 2, 2022, acs.estlett.2c00599, https://doi.org/10.1021/acs.estlett.2c00599.
- ^
Prof. Jose-Luis Jimenez [@jljcolorado], “11/ Let’s Assume That We Implemented GUV Now in 1% of Indoor Spaces in the US: - If We Reduced COVID Deaths by 1%, That’s -1300 / Year - If We Increase PM as in Our Paper, That’s +200-1100 / Year Very Uncertain. But of Similar Order. Definitely Need More Study.,” Tweet, Twitter, December 9, 2022, https://twitter.com/jljcolorado/status/1601083622093574145.
- ^
“The chemical mechanism for this study is a combination of the inorganic radical chemistry in an oxidation flow reactor (OFR) model and part of the Regional Atmospheric Chemistry Mechanism (RACM) relevant to this study. Section S1 of the Supporting Information provides more details of the mechanism. The mechanisms are run within the open-source KinSim chemical kinetics simulator” Ibid., D.
- ^
Note though that we understand that an updated and more detailed version of this model is currently in the works, which might have higher external validity (thanks to Richard Williamson for this point)
- ^
Jose-Luis Jimenez, “Germicidal UV: A Tradeoff between Disinfection and Indoor Smog,” Substack newsletter, Something in the Air (blog), December 8, 2022, https://jljcolorado.substack.com/p/germicidal-uv-a-tradeoff-between.
- ^
Ozone creation at UVC wavelengths above 242 nm is minimal. (With thanks to Richard Williamson for this point in a round of external reviews)
- ^
One of our external reviewers pointed out that ozone creation at UVC wavelengths above 242nm is approximately zero.
- ^
Thanks to Richard Williamson for pointing to the importance of the concentrations of VOCs of concern.
- ^
Byrd, A., Belkaid, Y. & Segre, J. The human skin microbiome. Nat Rev Microbiol 16, 143–155 (2018). https://doi.org/10.1038/nrmicro.2017.157
- ^
Hessling M, Haag R, Sieber N, Vatter P. The impact of far-UVC radiation (200-230 nm) on pathogens, cells, skin, and eyes - a collection and analysis of a hundred years of data. GMS Hyg Infect Control. 2021 Feb 16;16:Doc07. doi: 10.3205/dgkh000378. PMID: 33643774; PMCID: PMC7894148.
- ^
Edmonds-Wilson, S. L., Nurinova, N. I., Zapka, C. A., Fierer, N., & Wilson, M. (2015). Review of human hand microbiome research. Journal of dermatological science, 80(1), 3-12. (Thank you to Max Görlitz, whose comment on the EA forum led us to this review).
- ^
"One interesting deployment mode would be far-UVC fixtures with two modes: ‘business as usual’ mode and ‘emergency’ mode. In non-pandemic times, you would have the lamps running at exposure levels that pose a negligible or acceptable risk for the vast majority of the population. Once a pandemic threat is detected and infections are ramping up, the risk-benefit calculus changes and you could flip the switch to emergency mode for the lamps to run at substantially higher exposure levels” Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
- ^
“And we know, Ed [Nardell]'s told us about instances where they'd installed it in whole healthcare systems in Northern Africa. And then one person had an accidental exposure. And that was it. It was all switched off again” Dr. Ewan Eadie (call with Dr. Eadie and Dr. Wood, 3 March 2023).
- ^
Jam Kraprayoon, “Does the US Public Support Ultraviolet Germicidal Irradiation Technology for Reducing Risks from Pathogens?” (Rethink Priorities), accessed August 18, 2023, https://rethinkpriorities.org/publications/does-the-us-public-support-ultraviolet-germicidal-irradiation-technology. There are also other studies on these questions.
- ^
Jam Kraprayoon, “Does the US Public Support Ultraviolet Germicidal Irradiation Technology for Reducing Risks from Pathogens?” (Rethink Priorities), accessed August 18, 2023, https://rethinkpriorities.org/publications/does-the-us-public-support-ultraviolet-germicidal-irradiation-technology.
- ^
Thanks to Richard Williamson for pointing to the importance of elite perception in a round of external reviews.
- ^
There are some bacteria with higher resistance to UV light than others, including some extremophiles who are UVC-resistant, see; Marizcurrena, J.J., Morel, M.A., Braña, V. et al. Searching for novel photolyases in UVC-resistant Antarctic bacteria. Extremophiles 21, 409–418 (2017). https://doi.org/10.1007/s00792-016-0914-y
- ^
“Deterrence by denial strategies seek to deter an action by making it infeasible or unlikely to succeed, thus denying a potential aggressor confidence in attaining its objectives—deploying sufficient local military forces to defeat an invasion, for example.” Michael J Mazarr, “Understanding Deterrence” (RAND Corporation, 2018), https://www.rand.org/content/dam/rand/pubs/perspectives/PE200/PE295/RAND_PE295.pdf.
- ^
Eric F. Tom et al., “Experimental Evolution of UV Resistance in a Phage,” PeerJ 6 (2018), https://doi.org/10.7717/peerj.5190.
- ^
Eric F. Tom et al., “Experimental Evolution of UV Resistance in a Phage,” PeerJ 6 (2018), https://doi.org/10.7717/peerj.5190.
- ^
That is; it’s true that there will be selection pressure (from UV light) for the cell wall or DNA/ RNA structure to evolve in order to become less vulnerable to UV light. However, the kinds of adaptations necessary to make a virus immune to UV light would require significant changes to fundamental properties of the virus- such as RNA/ DNA structure, and make-up of the cell wall. Altering these properties would have a host of other ‘unintentional’ effects, since these components of the virus carry out a multitude of basic functions. For instance, altering RNA/ DNA structure could mean that protein synthesis (from the RNA/ DNA) becomes impaired or impossible. In this way, there are competing selective pressures to keep these fundamental properties of the virus constant. In comparison, antibiotics tend to work by blocking specific biochemical processes in bacteria (e.g. targeting a particular step in a metabolic pathway, or in the synthesis of a cell wall protein), where bacteria can more easily evolve adaptations to ‘get around’ this blockage without otherwise affecting the basic functioning of the cell.
- ^
Thanks to Vivian Belenky for this point.
- ^
Marizcurrena, J.J., Morel, M.A., Braña, V. et al, “Searching for novel photolyases in UVC-resistant Antarctic bacteria,” Extremophiles 21, 409–418 (2017), https://doi.org/10.1007/s00792-016-0914-y
- ^
David Brenner made this same point around minute 44 of his introductory presentation at the first international far-UVC congress in the summer of 2023. David Brenner, “Why Far-UVC Light?” (First International Congress on Far-UVC Science and Technology, Columbia University, June 21, 2023), https://www.youtube.com/watch?v=tH0zFk3cWC0.
- ^
On the concept of defense-in-depth in the context of global catastrophes, see Owen Cotton-Barratt, Max Daniel, and Anders Sandberg, “Defence in Depth Against Human Extinction: Prevention, Response, Resilience, and Why They All Matter,” Global Policy 11, no. 3 (2020): 271–82, https://doi.org/10.1111/1758-5899.12786.
- ^
UV light can also damage other types of materials found in the built environment, like wood, but this section focuses on plastics because of their ubiquity and importance in spaces like healthcare environments.
- ^
Emad Yousif and Raghad Haddad, “Photodegradation and Photostabilization of Polymers, Especially Polystyrene: Review,” SpringerPlus 2, no. 1 (August 23, 2013): 398, https://doi.org/10.1186/2193-1801-2-398. Mustafa Doğan, “Ultraviolet Light Accelerates the Degradation of Polyethylene Plastics,” Microscopy Research and Technique 84, no. 11 (2021): 2774–83, https://doi.org/10.1002/jemt.23838.
- ^
Luke Horton et al., “Spectrum of Virucidal Activity from Ultraviolet to Infrared Radiation,” Photochemical & Photobiological Sciences 19, no. 10 (October 1, 2020): 1262–70, https://doi.org/10.1039/d0pp00221f.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Darius Drungilas et al., “Evaluating the Impact of 222 Nm Far-UVC Radiation on the Aesthetic and Mechanical Properties of Materials Used in Public Bus Interiors,” Applied Sciences 13, no. 7 (January 2023): 4141, https://doi.org/10.3390/app13074141.
- ^
Darius Drungilas et al., “Evaluating the Impact of 222 Nm Far-UVC Radiation on the Aesthetic and Mechanical Properties of Materials Used in Public Bus Interiors,” Applied Sciences 13, no. 7 (January 2023): 4141, https://doi.org/10.3390/app13074141.
- ^
Thanks to Richard Williamson for pointing to this in a round of external reviews.
- ^
Table generated in part with the assistance of GPT4.
- ^
Because effectiveness is limited by the efficiency of the HVAC machine; for more on the limits of mechanical ventilation, see Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
As above, we consider “full-room” and “far-UVC” in one column here, but note that the type of UV system deployed could be independent from the wavelength — far-UVC lights can be deployed as upper-room systems.
- ^
Eadie, E., Hiwar, W., Fletcher, L., Tidswell, E., O’Mahoney, P., Buonanno, M., ... & Wood, K. (2022), “Far-UVC (222 nm) efficiently inactivates an airborne pathogen in a room-sized chamber” Scientific reports, 12(1), 4373. This estimate is from the high-exposure scenario, which is still below the he American Conference of Governmental Industrial Hygienists threshold limits for exposure. See also the Rethink Priorities/ 1DaySooner report here
- ^
Thanks to Vivian Belenky for this caveat.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view. On lower estimates, see Escombe, A. R. et al, “Upper-room ultraviolet light and negative air ionization to prevent tuberculosis transmission,” PLoS Med. 6, e1000043 (2009).
Matsie Mphaphlele et al., “Institutional Tuberculosis Transmission. Controlled Trial of Upper Room Ultraviolet Air Disinfection: A Basis for New Dosing Guidelines,” American Journal of Respiratory and Critical Care Medicine 192, no. 4 (August 8, 2015): 477, https://doi.org/10.1164/rccm.201501-0060OC.
- ^
We also asked some EA biosecurity researchers for their estimates of the amount of funding that has gone towards far-UVClight, but unfortunately they were unable to provide estimates. We are aware of several grants that have been made by some groups working on catastrophic biological risks towards far-UVCresearch, but are not aware of grants that have been made to upper-room systems.
- ^
Thanks to Vivian Belenky for their explanation of this.
- ^
Thanks to Jake Swett for this point.
- ^
Thanks to Jake Swett for these points and suggesting the improvement to this setup.
- ^
Dr. Wood: “I don't think it would stop transmission, say, at a very close range, but I think it could have an effect on super spreader events, which is where a lot of the transmission is happening.” Call with Dr. Eadie and Dr. Wood, 3 March 2023. Other experts we spoke with (e.g. Vivian Belenky) believe that upper-room room GUV would also have an effect on superspreader events.
- ^
Dr. Eadie: “we did look at this actually, in the Leeds [aerosol] chamber [...] So in that case, we had our source of pathogen and our collection device, and they were two meters apart. And we had a lamp in the middle. So up in the ceiling, in the middle of the two, and we got a reduction of 56%, which is roughly a mask. It's roughly equivalent to what some masks would achieve. But of course you have to think that that was the best-case scenario, when there was a lamp immediately between two people [...] So that's, again, that's why that real world deployment is so key.” Call with Dr. Eadie and Dr. Wood, 3 March 2023. (Note that this is the only chamber study so far, that 56% reduction could still be very useful, and that higher power could be used in some scenarios. Thanks to Jake Swett for these points in a round of external reviews)
- ^
Thanks to Richard Williamson for this point about tunability in a round of external reviews.
- ^
Thanks to Richard Williamson for pointing to these challenges in a round of external reviews.
- ^
“the relationship between amount of pathogen inhaled and cases of infection is only partially understood, and varies for different pathogens and individual susceptibility." 1DaySooner/Rethink report, 6.
- ^
Edward A. Nardell, “Air Disinfection for Airborne Infection Control with a Focus on COVID‐19,” Photochemistry and Photobiology 97, no. 3 (2021): 493–97, https://doi.org/10.1111/php.13421.
- ^
The eACH estimates are taken from 1DaySooner’s report, here. For discussion of eACH, see Nardell, “One ACH is defined as having occurred when a volume of air equal to the volume of the room is delivered, and an equal volume of well mixed air is exhausted from the room. In a well‐mixed room, one ACH removes approximately 63% of the air and air contaminants, including airborne pathogens, a second ACH removes 63% of what remains—a total of 86% removal, and so on. However, when infectious particles are being continuously generated in an occupied room, the calculation of ventilation efficiency is not so simple, and the mass balance Wells‐Riley equation is used to estimate the difference between generation and removal rates of infectious particles. When the mass balance approach is used, with good estimates of the rate of infectious particle generation, even 6 to 12 ACH may be inadequate to prevent transmission, depending on the duration of exposure” Edward A. Nardell, “Air Disinfection for Airborne Infection Control with a Focus on COVID‐19,” Photochemistry and Photobiology 97, no. 3 (2021): 493–97, https://doi.org/10.1111/php.13421. Thanks to GPT4 for helping to explain this (“However, it's important to note that the relationship between eACH and transmission reduction may not be directly proportional, as multiple factors can influence infection transmission in real-world scenarios [...] It is not accurate to directly infer that a system with 30 eACH would reduce infection transmission by three times as much as a system with 10 eACH. The actual impact on transmission reduction depends on the combined effect of the air disinfection system and the other factors influencing transmission in a given space.”)
- ^
With thanks to Richard Williamson for this point.
- ^
A. Roderick Escombe et al., “Upper-Room Ultraviolet Light and Negative Air Ionization to Prevent Tuberculosis Transmission,” PLOS Medicine 6, no. 3 (March 17, 2009): e1000043, https://doi.org/10.1371/journal.pmed.1000043.
- ^
Matsie Mphaphlele et al., “Institutional Tuberculosis Transmission. Controlled Trial of Upper Room Ultraviolet Air Disinfection: A Basis for New Dosing Guidelines,” American Journal of Respiratory and Critical Care Medicine 192, no. 4 (August 8, 2015): 477, https://doi.org/10.1164/rccm.201501-0060OC.
- ^
Note that these studies are different from real-world transmission; in these experiments, the guinea pigs breathe in air from TB wards that either contain, or do not contain, upper room GUV systems. In this way, the person-to-person (or ‘person-to-guinea pig’) transmission route is quite different compared to the real-world. It is difficult to know whether (in the real-world) upper room systems would be more or less impactful than these experiments suggest. It is possible that the effect of transmission through more direct contact (such as speaking with an infected person, as opposed to breathing in air from the room more generally) might make upper-room systems less impactful.
- ^
Peng Xu et al., “Impact of Environmental Factors on Efficacy of Upper-Room Air Ultraviolet Germicidal Irradiation for Inactivating Airborne Mycobacteria,” Environmental Science & Technology 39, no. 24 (2005): 9656–64.
- ^
Edward A. Nardell, “Air Disinfection for Airborne Infection Control with a Focus on COVID-19: Why Germicidal UV Is Essential†,” Photochemistry and Photobiology 97, no. 3 (2021): 493–97, https://doi.org/10.1111/php.13421.
- ^
Kowalski, W. (2010). Ultraviolet germicidal irradiation handbook: UVGI for air and surface disinfection. Springer science & business media.
- ^
Thank you to Vivan Belenky for pointing us to this reference, and describing the findings.
- ^
Ewan Eadie et al., “Far-UVC (222 Nm) Efficiently Inactivates an Airborne Pathogen in a Room-Sized Chamber,” Scientific Reports 12, no. 1 (March 23, 2022): 4373, https://doi.org/10.1038/s41598-022-08462-z.
- ^
Call with Dr. Ewan Eadie and Dr. Kenneth Wood, 3 March 2023.
- ^
Some uncertainties we have here: S. aureus is relatively resistant to UV compared to some pathogens of concern, like covid-19 and influenza, in which case we would expect better disinfection. On the other hand, on the other hand, the disinfection coefficient is very high, much higher than is seen in highly controlled benchtop experiments. Thank you to Richard Williamson for these points in a round of external review.
- ^
Eadie et al., “Far-UVC (222 Nm) Efficiently Inactivates an Airborne Pathogen in a Room-Sized Chamber.”
- ^
“And somebody can get quite painful -- and it's transient, it lasts a couple of days -- but, you know, painful keratitis, snow blindness, in the eye, and a painful erythema of the skin.” Dr. Ewan Eadie (call with Dr. Eadie and Dr. Wood, 3 March 2023.
- ^
Thanks to Dr. Eadie and Dr. Wood for pointing us to these considerations.
- ^
Grigory Volchenkov and Paul Jensen study, referenced in Edward Nardell’s talk at WHO, 20 minutes 34 seconds: https://who.zoom.us/rec/play/YPbVIilAHqjZolnrfCfXKhGK0Mwo3IovDJSRjdqE8-tCG7F_f_im1F-qU-GKJVwSYE7Yz0zvpn1uSh0o.Nf2JlQ3QPsv6JaYE?continueMode=true&_x_zm_rtaid=uMb4jyuGTRCpgLqMvITQBw.1679412010514.89f75873026185d7929248455532c685&_x_zm_rhtaid=948
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Referenced in Edward Nardell’s talk at WHO: https://who.zoom.us/rec/play/YPbVIilAHqjZolnrfCfXKhGK0Mwo3IovDJSRjdqE8-tCG7F_f_im1F-qU-GKJVwSYE7Yz0zvpn1uSh0o.Nf2JlQ3QPsv6JaYE?continueMode=true&_x_zm_rtaid=uMb4jyuGTRCpgLqMvITQBw.1679412010514.89f75873026185d7929248455532c685&_x_zm_rhtaid=948. Thanks to Vivian Belenky for the caveat on total installation costs.
- ^
“Given the pollution that far-UVC produces, rooms outfitted with far-UVC would also need to have appropriate ventilation or filtration to limit harms from pollutants. These mitigation measures would contribute to the eACH and raise the cost of far-UVC installation, so although we do not know the extent of ventilation/filtration needed, we can assume that far-UVC is somewhat less cost-effective than described in Table1” “Air Safety to Combat Global Catastrophic Biorisk,” 17, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view
- ^
Table 1, “Air Safety to Combat Global Catastrophic Biorisk,” 16-17, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Thanks to Vivian Belenky for this point.
- ^
“10 had, or were planned to have, upper room UV and they could only install in two out of those 10 schools because the rooms weren't suitable for upper room UV.” Dr. Ewan Eadie (call with Dr. Eadie and Dr. Wood, 3 March 2023.
- ^
“Community, Work, and School,” Centers for Disease Control and Prevention, February 11, 2020, https://www.cdc.gov/coronavirus/2019-ncov/community/ventilation/uvgi.html.
- ^
Notably (and mysteriously) this effect appears to exist for bacteria but not viruses (Thanks to Vivian Belenky for this point). For catastrophic pandemics, therefore, humidity may be less important.
- ^
Jordan Peccia et al., “Effects of Relative Humidity on the Ultraviolet Induced Inactivation of Airborne Bacteria,” Aerosol Science and Technology 35, no. 3 (January 2001): 728–40, https://doi.org/10.1080/02786820152546770.
- ^
“Grants,” Open Philanthropy, accessed August 18, 2023, https://www.openphilanthropy.org/grants/.
- ^
Thanks to Vivian Belenky for walking us through the key considerations and being willing to give this estimate. (Interview with Vivian Belenky, 11 May 2023, comments from Vivian Belenky on earlier draft, August 2023).
- ^
Interview with Vivian Belenky, 11 May 2023.
- ^
Suppressing pathogen transmission, especially in high-risk and high-traffic spaces, would reduce the spread of infectious diseases, extinguish some outbreaks, and buy critical time to combat more aggressive pathogens. With permanent incorporation into the environment, we could continuously defend against threats, even prior to detection, and without the dramatic changes in human behavior needed to reduce pathogen transmission.” (“Pathogen Transmission Suppression in the Built Environment” in Apollo Program for Biodefense (Final Report), Appendix A, 23, https://biodefensecommission.org/wp-content/uploads/2021/01/Apollo_report_final_v8_033121_web.pdf. )
- ^
Kevin M Esvelt, “Delay, Detect, Defend: Preparing for a Future in Which Thousands Can Release New Pandemics,” Geneva Papers (Geneva Centre for Security Policy, 2022), 13, https://dam.gcsp.ch/files/doc/gcsp-geneva-paper-29-22?_gl=1*xm44p1*_ga*ODQxMDI0NjY4LjE2ODM2NTg5MTg.*_ga_Z66DSTVXTJ*MTY4MzczNTIzNi4yLjAuMTY4MzczNTIzNi4wLjAuMA..#page=49&zoom=100,0,0
- ^
“American Pandemic Preparedness: Transforming Our Capabilities” (whitehouse.gov, 2021), https://www.whitehouse.gov/wp-content/uploads/2021/09/American-Pandemic-Preparedness-Transforming-Our-Capabilities-Final-For-Web.pdf?page=29.
- ^
Indeed, the plan may reflect “conventional wisdom” not just within the government, but also among private sector experts who were consulted for the plan.
- ^
“Clean Air in Buildings,” The White House, accessed August 18, 2023, https://www.whitehouse.gov/cleanindoorair/.
- ^
OSTP, “Fact Sheet: Departments and Agencies Commit to Cleaner Indoor Air Across the Nation,” The White House, December 8, 2022, https://www.whitehouse.gov/ostp/news-updates/2022/12/08/fact-sheet-departments-and-agencies-commit-to-cleaner-indoor-air-across-the-nation/.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 5, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Founders Pledge, “Philanthropy to the Right of Boom,” https://www.founderspledge.com/research/philanthropy-to-the-right-of-boom
- ^
“Johannes Ackva on Unfashionable Climate Interventions That Work, and Fashionable Ones That Don’t,” 80,000 Hours, accessed August 18, 2023, https://80000hours.org/podcast/episodes/johannes-ackva-unfashionable-climate-interventions/.
- ^
Thanks to Richard Williamson for raising both of these points in a round of external reviews.
- ^
For model: https://www.getguesstimate.com/models/21960; report Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Jose L. Jimenez et al., “What Were the Historical Reasons for the Resistance to Recognizing Airborne Transmission during the COVID-19 Pandemic?,” Indoor Air 32, no. 8 (2022): e13070, https://doi.org/10.1111/ina.13070.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 4, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
Thanks to Richard Williamson for pointing to the importance of considering unknown unknowns in a round of external reviews.
- ^
Gavriel Kleinwaks et al., “Air Safety to Combat Global Catastrophic Biorisk” (1DaySooner and Rethink Priorities, 2023), 27, https://drive.google.com/file/d/1QKusCnLzUs041nIuiq6nMxSIRcXaGiKq/view.
- ^
“By 2100, Will the Human Population Decrease by at Least 10% during Any Period of 5 Years?,” https://www.metaculus.com/questions/1493/global-population-decline-10-by-2100/.
- ^
“Ragnarök Question Series: If a Global Catastrophe Occurs, Will It Be Due to Naturally Occuring Pandemics?,” https://www.metaculus.com/questions/8745/gc-caused-by-natural-pandemic-if-gc-occurs/.
- ^
“Ragnarök Question Series: If a Global Catastrophe Occurs, Will It Be Due to Biotechnology or Bioengineered Organisms?,” https://www.metaculus.com/questions/1502/ragnar%25C3%25B6k-question-series-if-a-global-catastrophe-occurs-will-it-be-due-to-biotechnology-or-bioengineered-organisms/.
- ^
- ^
Kevin M Esvelt, “Delay, Detect, Defend: Preparing for a Future in Which Thousands Can Release New Pandemics,” Geneva Papers (Geneva Centre for Security Policy, 2022), 13, https://dam.gcsp.ch/files/doc/gcsp-geneva-paper-29-22?_gl=1*xm44p1*_ga*ODQxMDI0NjY4LjE2ODM2NTg5MTg.*_ga_Z66DSTVXTJ*MTY4MzczNTIzNi4yLjAuMTY4MzczNTIzNi4wLjAuMA..#page=49&zoom=100,0,0
- ^
Interview with Jaime Yassif, 12 May 2023; Interview with Vivian Belenky, 12 May 2023.
- ^
Relatedly, we could also fund policy advocacy with the aim of setting indoor air quality standards; current indoor air standards do not consider infectious disease risk, and it seems plausible that the lack of a clear standard is a bottleneck towards funding development into these technologies.
- ^
Max Görlitz has noted the importance of controlled/controllable environments for real-world trials, including the issues with original upper-room trials in the mid-Twentieth Century: “The design of trials that showed more ambiguous results has been criticized. While upper-room GUV was installed in school classrooms, the kids shared other indoor environments (e.g. the schoolbus) that weren't equipped with upper-room GUV. Presumably, infections just shifted away from classrooms to these other shared environments. It seems likely that this made people somewhat disillusioned with the technology and is part of the reason why upper-room GUV hasn't been more popular.” Max Görlitz, “Thoughts on Far-UVC after Working in the Field for 8 Months,” Effective Altruism Forum, 2023, https://forum.effectivealtruism.org/posts/z8ZWwm4xeHBAiLZ6d/thoughts-on-far-uvc-after-working-in-the-field-for-8-months.
Low-hanging fruit for someone interested in the public communications side... make a Wikipedia page for far-UVC! One day I'll get to this myself...
We discussed this, but it might make more sense to add/expand the section of the main GUV article: https://en.wikipedia.org/wiki/Ultraviolet_germicidal_irradiation Maybe opening a discussion in wikitalk about whether it merits its own page, too?
I support both ideas - adding/expanding the UVGI page and starting discussion of a new far-UVC page on wikitalk. There is already one mention of starting a separate page on wikitalk.
I think it's warranted given the distinct biophysical effects of this spectral band as well as the development of far-UVC as a commercial technology and area of broader interest.
Great to see your thinking laid out this way, and of course thank you for your interest in our (1Day Sooner/Rethink Priorities) report!
It was useful to see the discussion of possible overhype from the funding side of the field, since I don't have insight into funding decisions. On the other hand, there are reasons funders might want to focus attention on far-UV, without disregarding the usefulness of conventional-wavelength GUV: since far-UV requires more research than conventional-wavelength systems at this time, but might ultimately be easier to install, the far-UV research payoff could be very large for increasing adoption of GUV in general. I expect that conventional-wavelength systems would benefit from investment into R&D for easier installation, but that's not obviously a place for philanthropic funding. The safety studies necessary for far-UV are too expensive for the current market size, so if far-UV research does not get more philanthropic funding than conventional-wavelength GUV, far-UV safety studies might not be performed in a rigorous way. However, I would agree that funders should be wavelength-agnostic if they are directly funding installations.
Because of the challenges facing comprehensive far-UV analysis, I was surprised that you didn't think it would be very impactful for philanthropists to fund studies--broadly speaking, I agree about the lack of expertise, but this is a small enough field that the informed voices are fairly well-known within the field and I think interested philanthropic bodies would be able to consult those informed opinions. Again, I don't have insight into the funding side of the process, so that may be optimistic. I am certainly biased, since 1Day Sooner does regularly apply/advocate for philanthropic funding for technical research! On the reverse side, personal experience has left me pessimistic about policy advocacy for GUV research, but your report has swayed me somewhat to at least consider the fact that there is not a concerted, heavyweight policy advocacy effort in this area.
I appreciated the argument on capturing the bulk of the risk by later deployment; it was a very helpful presentation of the case. I do think that there is a learning-by-doing element to GUV rollout (for either type of GUV), where rollout and analysis in select environments is necessary for better understanding broader GUV use cases. Identifying those environments is an element of the current 1Day Sooner IAQ project. I also would love to see the cost of GUV installation fall sooner rather than later in order to address endemic disease burden worldwide, e.g. via widespread installation in TB clinics. (I'm fully aware that this use case might remain impractical, but it's nice to consider the potential to address global health! Of course if a funder is specifically trying to fight TB, I’d still recommend sinking their money into vaccine research or treatment.)
Finally, this report was extremely helpful for a current 1Day Sooner project! We're working on a report to assess the potential for market shaping techniques to accelerate the adoption of indoor air cleaning technology. This post, and writing up this comment, really helped clarify some of my thinking about the possible directions we'd been tossing around, so a huge thank you for that!
Executive summary: The report examines germicidal ultraviolet (GUV) light, finding it is a promising intervention for improving indoor biological air quality and reducing pathogen transmission including for future catastrophic risks. Uncertainty remains over the ultimate safety, cost, and real-world effectiveness of different GUV systems and wavelengths of UV light. Far-UVC in particular may have large upside but also risks, suggesting a "wavelength-agnostic" approach focused on catalyzing safety studies, market incentives, and large-scale government funded research could maximize impact.
Key points:
This comment was auto-generated by the EA Forum Team. Feel free to point out issues with this summary by replying to the comment, and contact us if you have feedback.
Perhaps I missed it in the article, but another challenge to potentially overcome is the seeming reluctance of many decisionmakers to take seriously aerosolized transmission of pathogens. I can probably dig up more and better sources for this issue but here is one I came across by quickly Googling. Here, in Sweden, I am not sure the authorities have yet communicated that one, if not the primary transmission route for COVID, is via aerosols. This barrier might make widespread adoption of UV tech even less likely to succeed.
Great post BTW!
Hi Ulrik, thanks for this comment! Very much agreed on the communications failures around aerosolized transmission. I wonder how much the mechanics of transmission would enter into a policy discussion around GUV (rather than a simplified “These lights can help suppress outbreaks.”)
This was very helpful! I found the diagrams particularly useful. Visible lighting design for rooms has a similar problem of uniform illumination, but it is mitigated by the fact that there is significant reflection of the light, which I presume does not apply for far UVC.
Has there been any work on planning to relocate existing UV systems to the most critical tasks, if an extreme pandemic hit soon, of making more super PPE/UV systems?
The units do not appear to be complete - cost of 1 ACH for how big of space? Footnote 131 requires a password. Footnote 132 says “all public buildings in the US” not “all US buildings.” If public building is defined as this, I would guess that would control less than 10% of transmission in the US.