Hi everyone, I’m working on an article for Recursive Adaptation about the death and disease burden of addiction and I think some folks here might be pretty experienced and structured on these types of questions, so I thought I’d post a veryyy rough initial draft / notes for feedback. And if you’d be interested in working on this article with me please let me know, I'd love the help.
Recursive Adaption is the publication of CASPR — we are a new organization focused on scalable strategies for addiction, particularly development and deployment of new medications, including scaling GLP-1s for addiction and ensuring suzetrigine access (which is an opioid-replacing painkiller that will be available next year but insurance generally won’t cover, which is... a bad situation).
We recently published a long article about the scientific and strategic case for us GLP-1s for addiction, which was in the most recent Astral Codex links post. Subscribe to our blog!!
So, here’s what I have so far about these questions on addiction and leading causes of death.
US deaths from addiction
Drug overdoses, opioids and stimulants, now cause more than twice as many annual deaths in the United States as HIV/AIDS caused at its peak in 1995 (109,000 vs 45,000). Overdose deaths are just one part of the mortality burden— addiction kills even more people slowly.
US deaths from excess alcohol use are 178,000 per year and deaths from smoking are 480,000 per year. That’s a total of about 767,000 annual deaths from substance use disorders.
For context, COVID deaths peaked at 450,000 annually and are now ~90% lower than peak.
How does this compare to deaths from cancer and heart disease? Looking at top line numbers in the US, cancer deaths are about 609,000 and heart disease deaths are 695,000. Both of those are lower than the 767,000 from substance use and actually those numbers are inflated because a big portion of heart disease and cancer death is caused by substance use. If we subtract those deaths, the gap gets bigger.
Deaths from non-addiction related cancer
In the USA
According to the American Cancer Society, “In 2022, there will be an estimated 1.9 million new cancer cases diagnosed and 609,360 cancer deaths in the United States.”
According the CDC, smoking causes 30% of all cancer deaths annually in the US. Higher in other countries?
If we subtract that 30% from the total cancer deaths and move those to addiction, we are left with 426,552 deaths.
Another 3% of cancer death is caused by alcohol, which brings non-addiction cancer down to about 408,271.
Deaths from non-addiction heart disease
According to the CDC, 695,000 people die of heart disease every year in the US. They call it the ‘leading cause of death’— but we have a slightly different idea of what is a “cause”!
About 30% of deaths from heart disease come from smoking, which brings us to 486,500 non-smoking related heart disease deaths.
As for alcohol, opioids, stimulants, this study, summarized here, looks at rates of substance-use related cardiovascular death but this doesn’t seem to be quite the same as attributing a cause. I haven’t found a number yet for heart disease deaths caused by substance use.
US addiction deaths vs heart disease and cancer
Where does this leave us?
- US Deaths from Addiction: 767,000
- US Deaths from Non-Addiction Related Cancer: 408,271
- US Deaths from Non-Smoking Related Heart Disease: 486,500 (still need to subtract alcohol, opioid, and stimulant deaths here).
Addiction #1 cause of DALYs in the USA
Here’s a chart we made from WHO data for a post that calls for an operation warp speed for addiction medication:
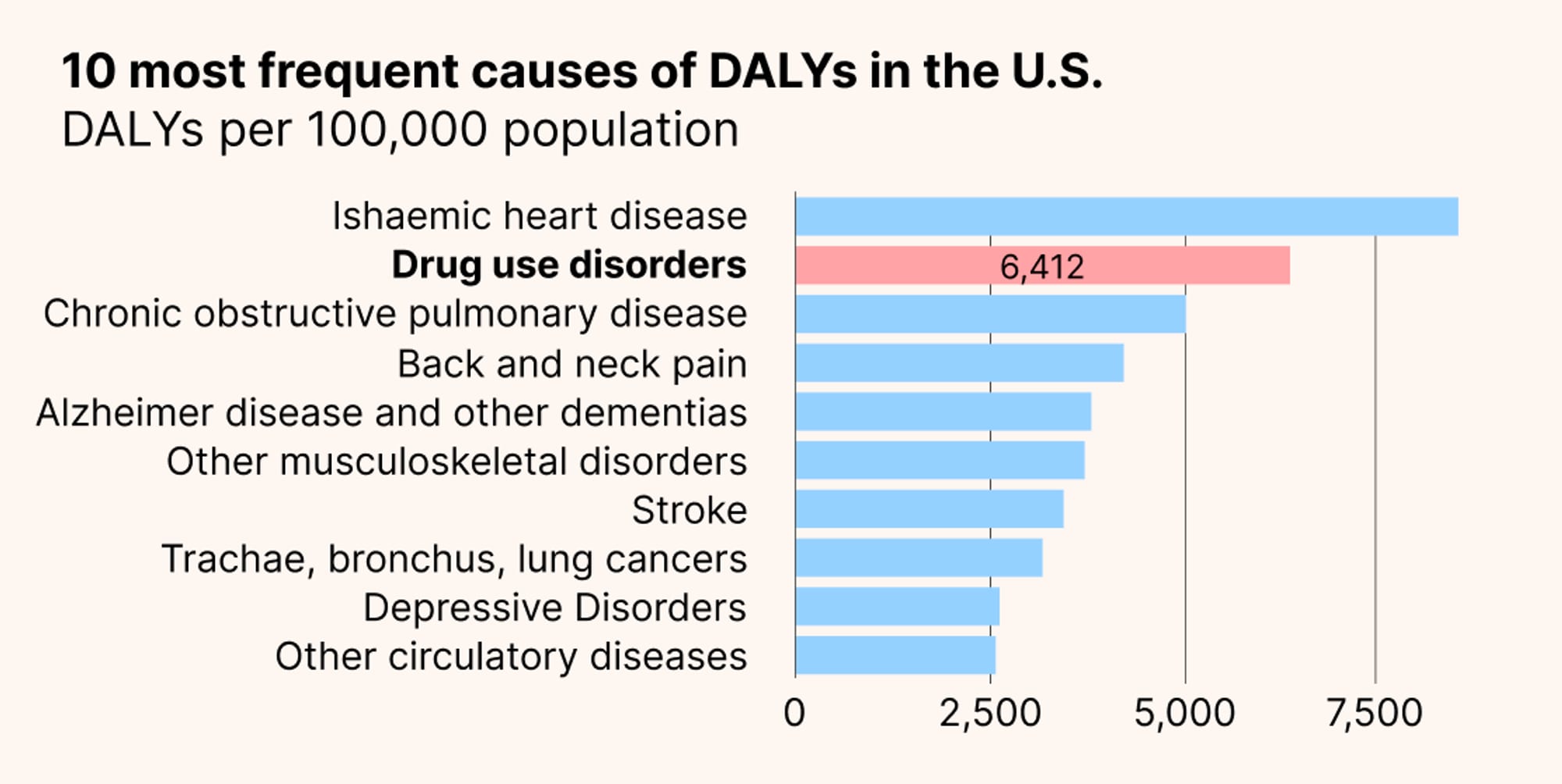
This comes right from the WHO DALY dashboard for the USA. But this does not include alcohol or cigarettes in ‘drug use’ and it also breaks up cancers and heart diseases into various subcategories. I’m pretty sure that addiction, if you include alcohol and cigarettes (and subtracting those from heart disease and cancer), would be at the top of DALYs in the US even after grouping together heart diseases and cancers. It would be great to have a method for this.
If you include smoking and drinking’s effects on dementia, liver disease, depression, anxiety, etc, the DALYs would keep rising and, I believe, far outstrip any other cause of disease.
And if you include crime, incarceration, the drug war, families falling apart, and all sorts of other externalities related to use of alcohol, opioids, and stimulants, the DALYs would keep on rising. Something like 40% of violent crimes in the US are committed by someone who has been drinking alcohol.
What about deaths and DALYs worldwide?
I haven’t yet attempted to look at this systematically worldwide, but would love some suggestions on where or how to do so (or help from someone who wants to collaborate on this!).
Opioid and stimulant deaths are generally much lower outside of the US and the US seems to be in the highish range on drinking. But globally, ~22% of people smoke and only ~12% do in the US. Since deaths from addiction appear to be so much higher than deaths from non-substance cancer and heart disease in the US, then addiction might also be the highest cause of death globally.
A couple misc tidbits from my notes:
- Alcohol causes about 750,000 cancer deaths per year worldwide.
- Worldwide 20% of deaths from coronary heart disease are estimated to come from cigarettes.
What about food?
If you considered modern processed foods addictive, and they seem to follow many of the same reward pathways and respond to some of the same medicines as addiction to substances (GLP-1s), then you would attribute a huge additional chunk of death and disease to addiction. This would be interesting to do the numbers on as well.
Next steps
I’d love comments with suggestions big and small, links, advice, etc. And would love collaborators even more, I can put this into a google doc for us.
For folks that are interested in tackling major public health crises, this may be the biggest of all! And what's so important about addiction as a public health challenge is that it's preventable. CASPR is a mostly volunteer driven project, with folks from EA forum and 80,000 jobs.
I genuinely believe that we have a chance to substantially speed up awareness and access to treatments that can prevent or cure addiction and, in doing so, save hundreds of thousands or millions of lives.

Thank you, this is extremely helpful! I will dive into this.