Summary
Bioethicists influence practices and policies in medicine, science, and public health. However, little is known about bioethicists' views in aggregate. We recently surveyed 824 U.S bioethicists on a wide range of ethical issues, including several issues of interest to the EA community (e.g., compensating organ donors, priority setting, paternalistic regulations, and trade-offs between human and animal welfare, among others). We aimed to contact everyone who presented at the American Society for Bioethics and Humanities Annual Conference in 2021 or 2022 and/or is affiliated with a US bioethics training program. Of the 1,713 people contacted, 824 (48%) completed the survey.
Why should EAs care?
- As Devin Kalish puts it in this nice post: "Bioethics is the field of ethics that focuses on issues like pandemics, human enhancement, AI, global health, animal rights, and environmental ethics. Bioethicists, in short, have basically the same exact interests as us."
- Many EAs don't hold the bioethics community in high regard. Much of this animus seems to stem from EAs' perception that bioethicists have bad takes. (See Devin's post for more on this.) Our survey casts light on bioethicists' views; people can update their opinions accordingly.
What did we find?
Chris Said of Apollo Surveys[1] separately analyzed our data and wrote a blog post summarizing our results:
Primary results
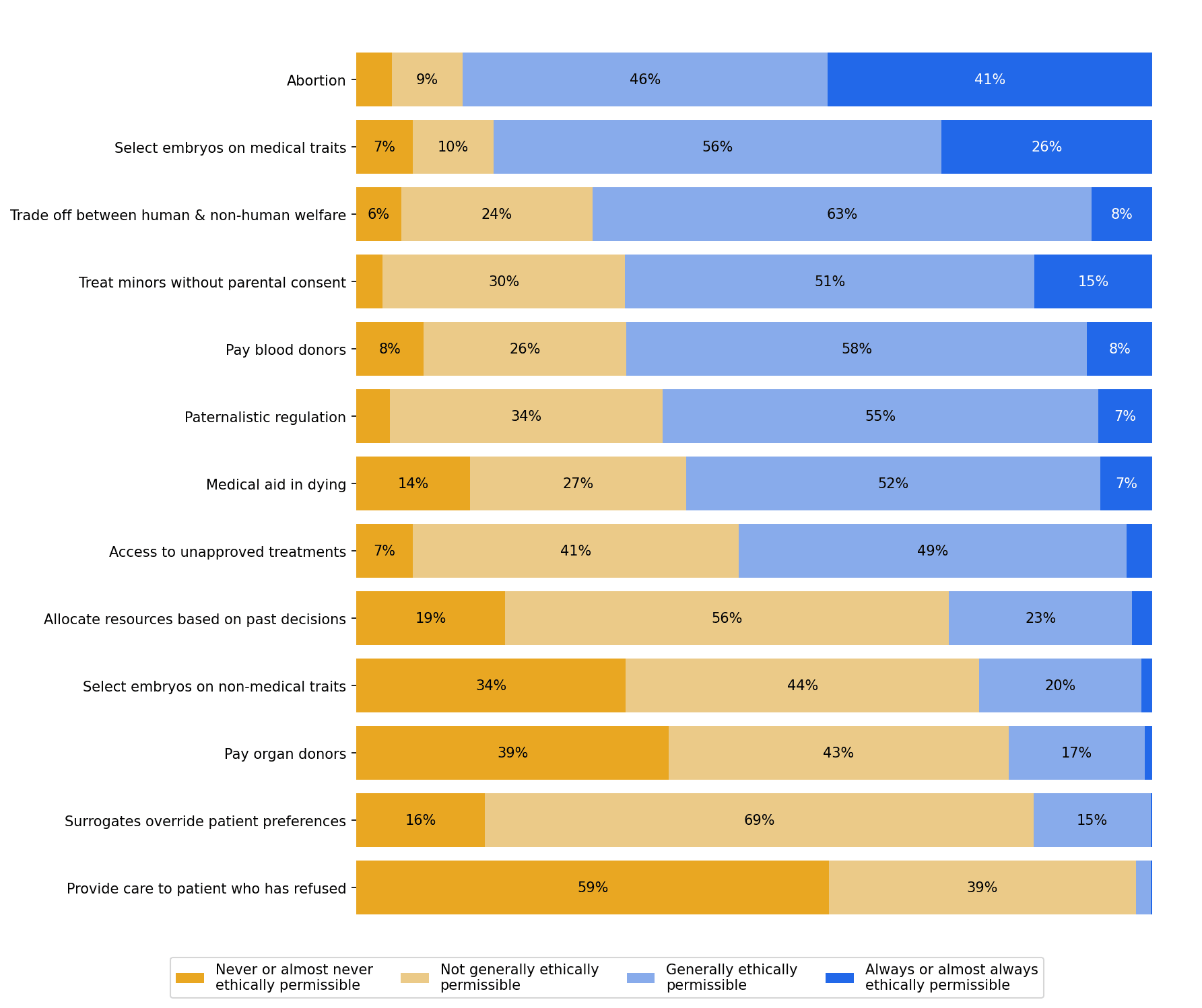
- A large majority (87%) of bioethicists believed that abortion was ethically permissible.
- 82% thought it was permissible to select embryos based on somewhat painful medical conditions, whereas only 22% thought it was permissible to select on non-medical traits like eye color or height.
- 59% thought it was ethically permissible for clinicians to assist patients in ending their own lives.
- 15% of bioethicists thought it was ethically permissible to offer payment in exchange for organs (e.g. kidneys).
Question 1
- Please provide your opinion on whether the following actions are ethically permissible.
- Is abortion ethically permissible?
- Is it ethically permissible to select some embryos over others for gestation on the basis of somewhat painful medical conditions?
- Is it ethically permissible to make trade-offs between human welfare and non-human animal welfare?
- Is it ethically permissible for a clinician to treat a 14-year-old for opioid use disorder without their parents’ knowledge or consent?
- Is it ethically permissible to offer payment in exchange for blood products?
- Is it ethically permissible to subject people to regulation they disagree with, solely for the sake of their own good?
- Is it ethically permissible for clinicians to assist patients in ending their own lives if they request this?
- Is it ethically permissible for a government to allow an individual to access treatments that have not been approved by regulatory agencies, but only risk harming that individual and not others?
- Is it ethically permissible to consider an individual’s past decisions when determining their access to medical resources?
- Is it ethically permissible to select some embryos over others for gestation on the basis of non-medical traits (e.g., eye color, height)?
- Is it ethically permissible to offer payment in exchange for organs (e.g., kidneys)?
- Is it ethically permissible for decisional surrogates to make a medical decision that they believe is in a patient's best interest, even when that decision goes against the patient’s previously stated preferences?
- Is it ethically permissible for a clinician to provide life-saving care to an adult patient who has refused that care and has decision-making capacity?
Results
Question 2
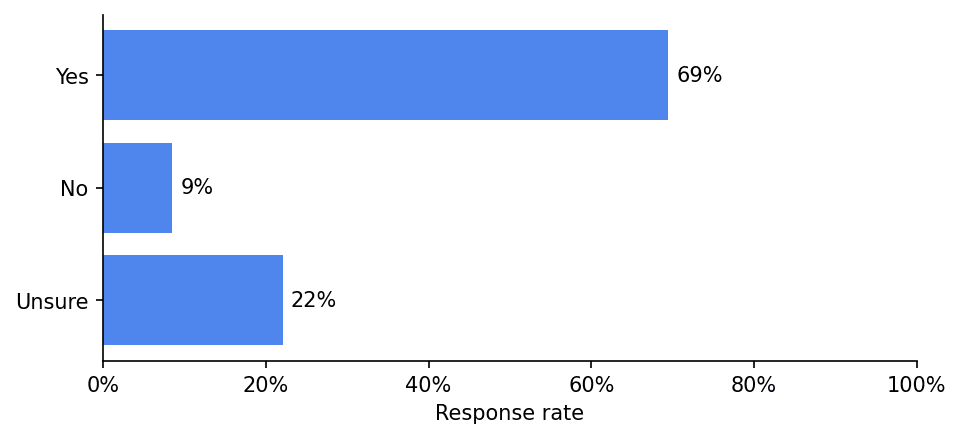
In general, should policymakers consider non-health benefits and harms (like whether expanding access to a service will reduce beneficiaries’ financial risk) when allocating medical resources?
Results
Question 3
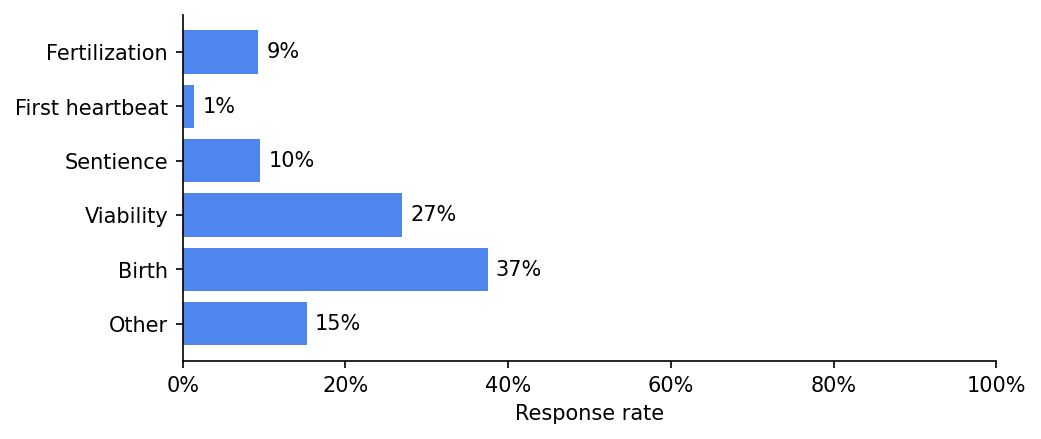
A being becomes a person at...
Results
Question 4
Does the fact that a person's life is expected to be worth living once we bring them into existence give us a moral reason to bring them into existence?
Results
Question 5
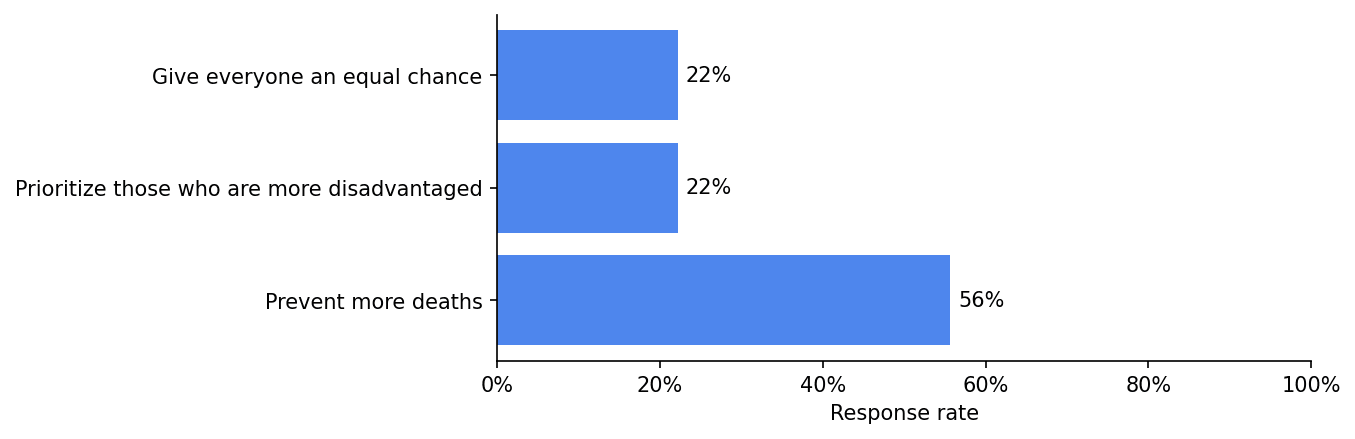
If there are not enough lifesaving resources for everyone at risk of death, we should:
Results
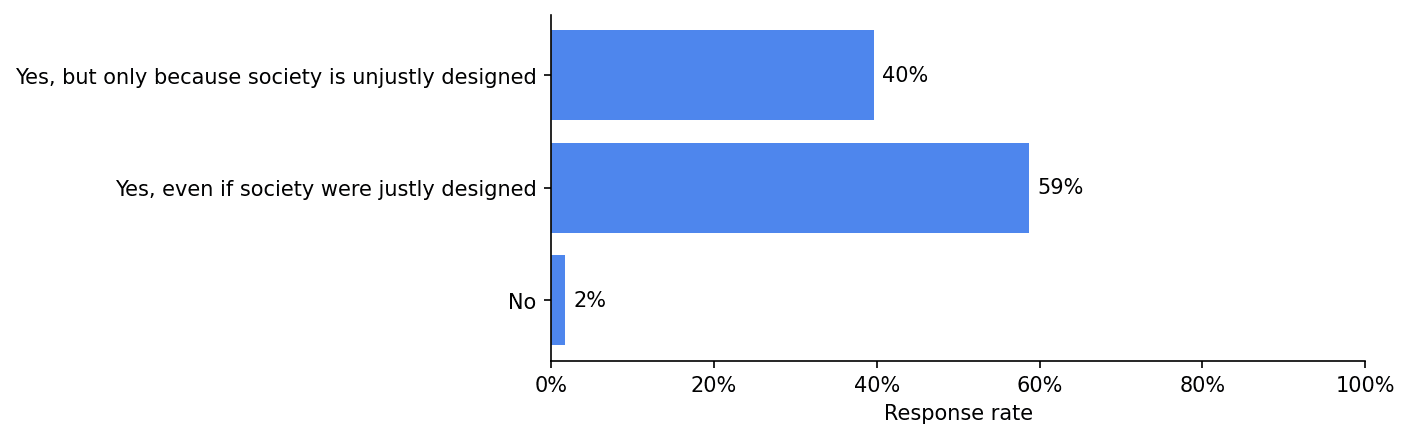
Question 6
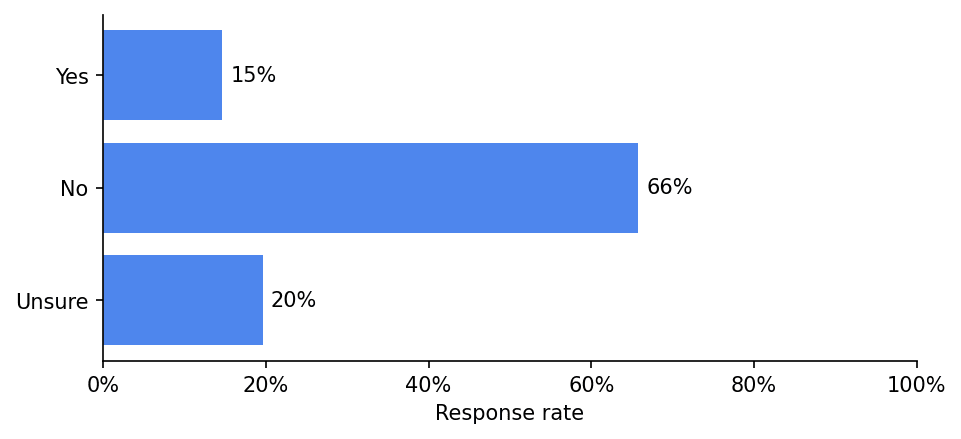
Is being unable to see disadvantaging?
Results
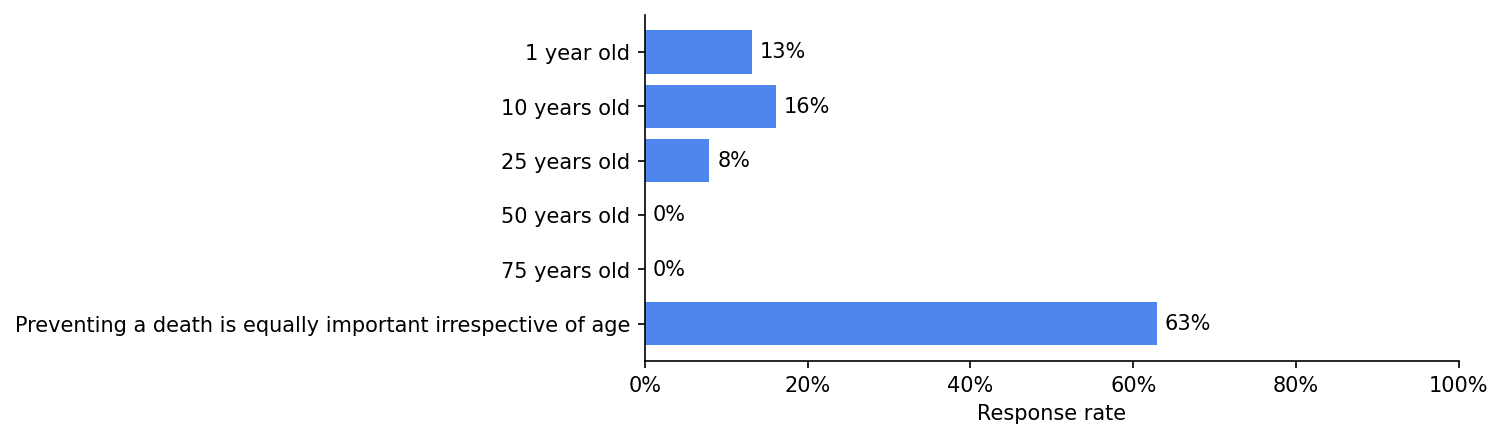
Question 7
It is most important to prevent someone from dying at which of the following ages:
Results
Some concluding thoughts
- There are more analyses/data in the paper (e.g., comparisons of bioethicists' views to those of the US public; data on bioethicists' backgrounds; analyses of the relationship between bioethicists' normative commitments and their views on specific issues). You can access the paper here. Feel free to reach out if you have trouble accessing it.
- We also surveyed bioethicists about issues related to research ethics (e.g., challenge trials; information hazards). These results will be published separately.
- If you're interested in administering this survey to EAs, please reach out.
- The American Journal of Bioethics will solicit peer commentaries on this paper in the near future. Please consider writing a commentary if you have thoughts. Edit: the link to do so can be accessed here.
- Sophie Gibert (the second author) and I have a podcast, Bio(un)ethical, where we often discuss issues at the intersection of bioethics and EA. If these issues are of interest to you, consider checking it out.
- ^
Apollo Surveys and EA Funds supported this work.

Thanks a lot for collecting this survey! I think it's valuable to solicit 'external' (to the EA community) views on important questions that affect our decision-making, especially from plausible expert groups.
I'm quite shocked at the vehemence and dismissiveness of many of the comments on this post responding to these results. Here are some quotes from other commenters:
1.
2.
3.
4.
Here are some possible explanations for the supposedly crazy results:
I share the intuition that many of the results in the survey seem surprising, and very discrepant from my own views. But regardless of whether you understand the reasons, surely after seeing that a group of people holds substantially different views to your own, your all-things-considered belief should shift at least somewhat towards those views, even if your "independent impression" does not? Especially when that group has years of relevant thought or expertise; these facts make it more likely that there are valid reasons underpinning their beliefs. Where there are discrepancies, there's a chance that they are right and you/we are wrong.
I'm worried that some of the quotes above represent something like cognitive dissonance or a boomerang effect. Or at least they seem more like "soldier mindset" than I'd expect here, although I note some exceptions where several commenters (including some of those I quoted above) ask others for input on helping to understand and steelman the bioethicists' views.
[Edit: the following paragraph felt true at the time of writing but I regret writing it as it seems pointlessly offensive/inflammatory itself in hindsight. I apologise to the people I quoted above.] Honestly, seeing the prevalence of these kinds of reactions in the comments makes me feel less confident in the epistemic health of this community and more worried about groupthink type effects. (Maybe some of these commenters have reasons for their vehemence and dismissiveness that I'm missing?)
Sorry, that was ambiguous on my part. There's a differentiation between research ethics issues (how trials are run, etc.) and clinical ethics (medical aid in dying, accessing unapproved treatments, how to treat a patient with X complicated issue, etc.). My work focuses on the former, not the latter, so I can't speak much to that. I meant "conservative" in the sense of hesitance to adjust existing norms or systems in research ethics oversight and, for example, a very strong default orientation towards any measures that reduce risk (or seem to reduce risk) for research participants.