Comments
This post covers key insights for pandemic risk reduction from our Risk Analysis paper, which was awarded ‘Best Paper of 2025’
Global pandemics, such as the Black Death, the Spanish Flu, and most recently, COVID-19, have brought hardship and loss: from global famine to loss of life, from deepening inequality to overwhelming health systems, and more.
An important lesson arises: the more prepared we are against a pandemic, the better we can protect the lives of millions.
Historically, pandemics usually arose through animal-to-human interaction. In the present day, a new origin source for pandemic potential pathogens (PPP) has emerged from human interaction with PPP in laboratory settings (for example, in vaccine development). This represents a new type of risk with different characteristics (e.g., geographic distribution) and potential for harm.
Alongside laboratory origin sources, increased global travel (especially via air networks) facilitates the rapid spread of pathogens, further increasing potential for harm. Even if a particular country is unlikely to give rise to a new emerging infectious disease or be the source of a lab leak, it might be strongly connected to other countries that do face such risks.
But infectious diseases don’t affect only our physical and mental health. Given that pandemics do not unfold in isolation, the consequences cascade through health systems, economies, and food supply chains.
It is then essential to discover which countries influence global pandemic risk and how to use this information to prioritize risk mitigation efforts, especially since reducing harm from pandemics has become a global priority.
To answer this question, my colleagues and I set out to develop a model that simulates how diseases spread between countries through air travel, starting from either Emerging Infectious Diseases (EID) — diseases that jump from animals to humans — or level 3 and 4 high-security laboratory leaks — facilities that study dangerous or potentially lethal pathogens.
Using global travel data alongside measures of where a pandemic is most likely to begin, the model explores how expected case burdens are distributed across countries during the first 30 days of a pandemic.
The findings suggest that, by day 30, three countries consistently face the highest risk regardless of where a pandemic starts: the United States, China, and India, as they are significant travel hubs with large populations. This suggests a small number of locations where preparedness and mitigation efforts could have the highest leverage.
To read the full paper, find it here: Assessing Global Pandemic Risks from Emerging Infectious Diseases and High Containment Laboratory Leaks: A Country-Level Spatial Network SIR Model Analysis.
For a brief summary of the model and findings, continue reading below.
Methodology
Our spatial network susceptible infectious removed (SIR) model treats each of the world's 195 countries as a node in a network connected by air travel. We used real data on daily international flights to show how diseases spread between countries. The model runs simulations starting a pandemic in each country individually and then tracks how the disease spreads over 30 days using equations that divide populations into three groups: susceptible (can get sick), infected (currently sick), and removed (recovered or deceased).
To determine where pandemics are most likely to start, we developed two separate scoring systems. For natural diseases emerging from animals, we used existing vulnerability indices that account for factors like healthcare capacity, population density, and economic stability — with Central African countries scoring highest. For laboratory accidents, we created a measure combining the number and size of high-containment labs in each country with that country's biosafety management scores. We then weighted the model's outputs by these origin probabilities to calculate which countries face the highest expected infections, accounting for both where pandemics might start and how global travel networks transform that initial risk into widespread outbreaks.
Results
For EIDs, risk starts concentrated in Central Africa, particularly Nigeria, the Democratic Republic of Congo, Equatorial Guinea, and the Central African Republic, during the first 10 days. Yet, interestingly enough, by day 30, the United States emerges with the highest number of cumulative infections**, followed by India and China, even though neither was the origin point. This shift demonstrates how global travel networks transform risk: diseases may start in remote locations, but they inevitably concentrate in major transportation hubs with large populations within a month.
With laboratory leak scenarios, from day 10 onward, the United States and India dominate the risk distribution. India has five BSL-3 or BSL-4 laboratories and comparatively lower biosafety management. Coupled with its position as a major global travel hub and large population, it contributes approximately 30% of total lab leak pandemic risk by day 30. China ranks third in both scenarios by day 30.
Regardless of whether a pandemic originates from nature or a lab accident, the same three countries (USA, India, and China) consistently face the highest number of infections within the first month, making them critical intervention points for early detection systems and prevention efforts.
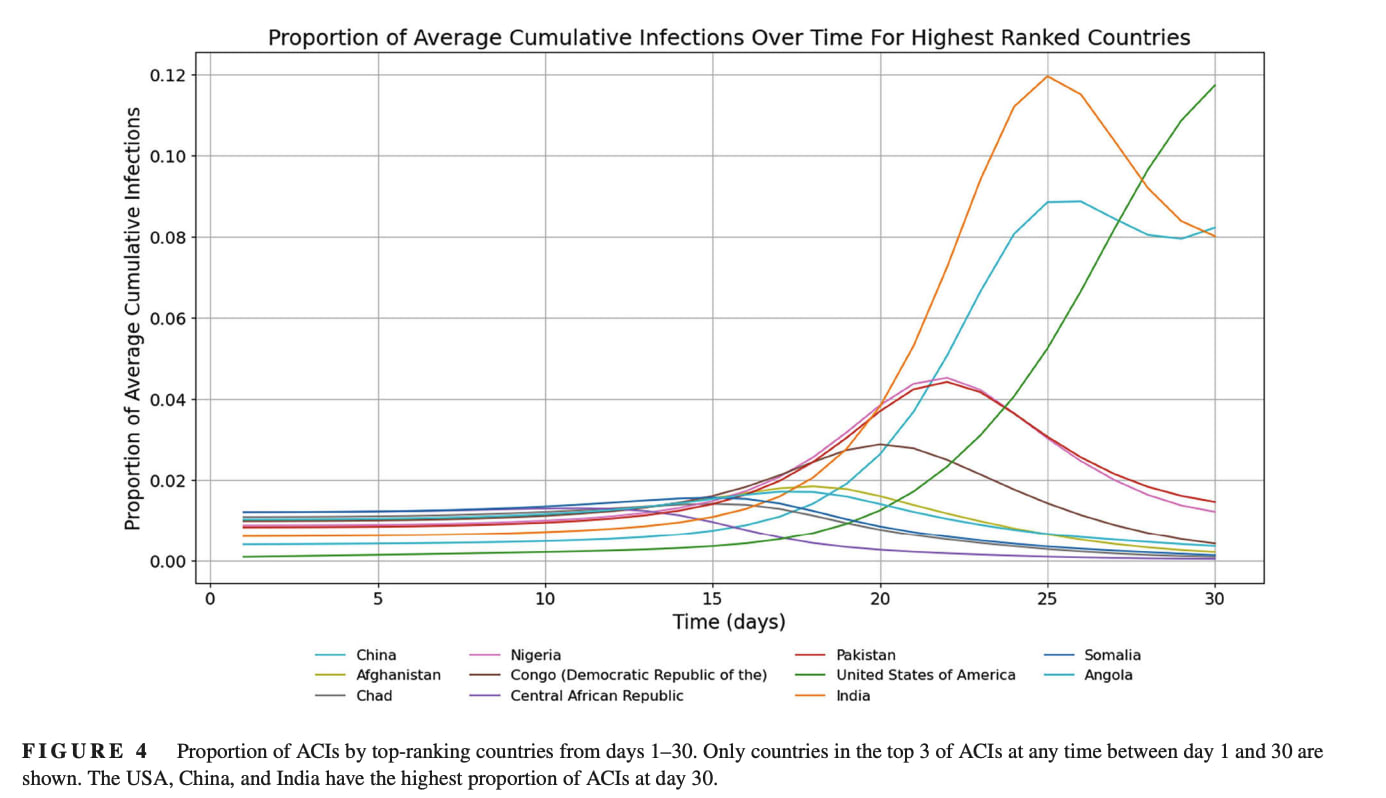
Figure 1: Proportion of Average Cumulative Infections (ACI)* by top-ranking countries from days 1 to 30 in an EID scenario.
*ACI is obtained by simulating pandemic evolution for each country as the origin source; we then average across simulations, weighting values according to the probability of each country being the origin source.
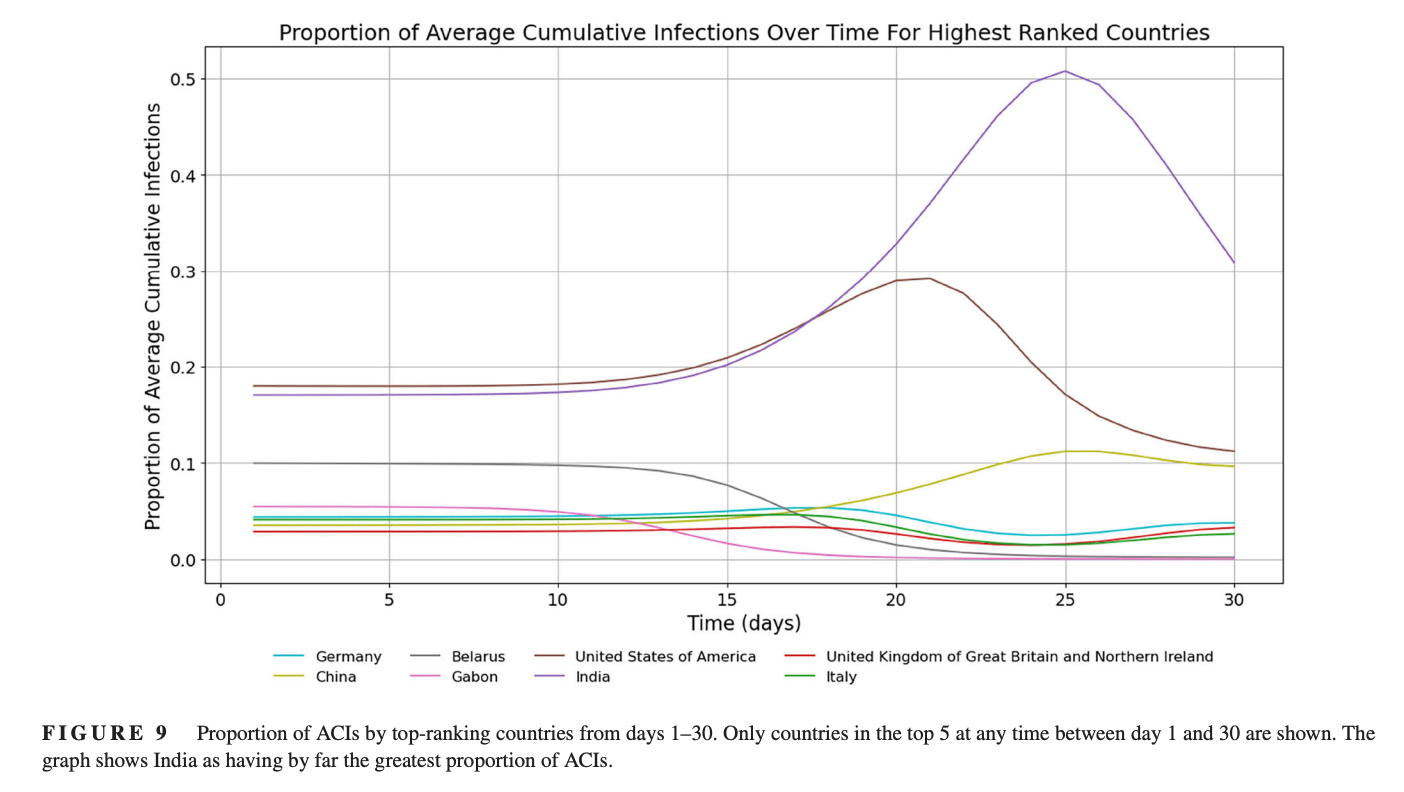
Figure 2: Proportion of Average Cumulative Infections (ACI) by top-ranking countries from days 1 to 30 in a lab leak scenario.
**We ran simulations starting from every country, then weighted results by the probability of each being the actual origin. This created a weighted average that identifies which countries consistently face the highest infections across all possible pandemic scenarios.
Limitations
The presented SIR model should be thought of as a preliminary investigation intended to guide future work. There are several important limitations, such as the country level of model abstraction, gaps in the datasets used, and assumptions regarding the EID and lab leak potential measures. Other choices of risk metric are likely to change prioritization significantly. The risk metric chosen — average proportion of global cases at day 30 across origin risk-weighted simulations — is strongly influenced by population, as we focus on global cases. There is a lack of global oversight for high-containment laboratories — while the WHO provides guidelines, no international body regulates how countries implement BSL-3 or BSL-4 practices, leading to widely varying standards.
This governance gap is concerning, as our research shows how a laboratory accident in one country could become a global problem within 30 days through travel networks. Interventions such as standardized biosafety risk assessment protocols and independent verification offer potential avenues for reducing actual risk, which are consistent with our results. These would have the added benefit of creating higher-quality data that could improve the accuracy of future pandemic risk modeling.
Going forward
Our research points to an important finding:
The trajectory and final destination of a disease may matter more than its origin, especially when planning interventions.
In the case of EIDs, origin countries in Central Africa have minimal international connectivity, yet infections funnel through major travel hubs within weeks. Deploying early warning systems at airports in the USA, India, and China (where pandemic risk tends to concentrate) may be more effective than focusing solely on predicted origin locations.
The findings identify India as a potentially high-leverage point for reducing pandemic risk due to its combination of five high-containment laboratories, the biosafety indicators used in this analysis, and its central position in global travel networks.
Targeted interventions, such as strengthening biosafety infrastructure or implementing airport screening at hubs, could represent cost-effective approaches to pandemic prevention, though formal cost-effectiveness analysis would be needed to confirm this.
Finally, we argue for establishing coordinated international frameworks with standardized protocols and independent verification to both reduce actual risk and improve future pandemic modeling accuracy.
