Comments
Hi Simon,
I think it's valuable to see all of this in one place, and I appreciate the digging required to piece this together.
A few comments:
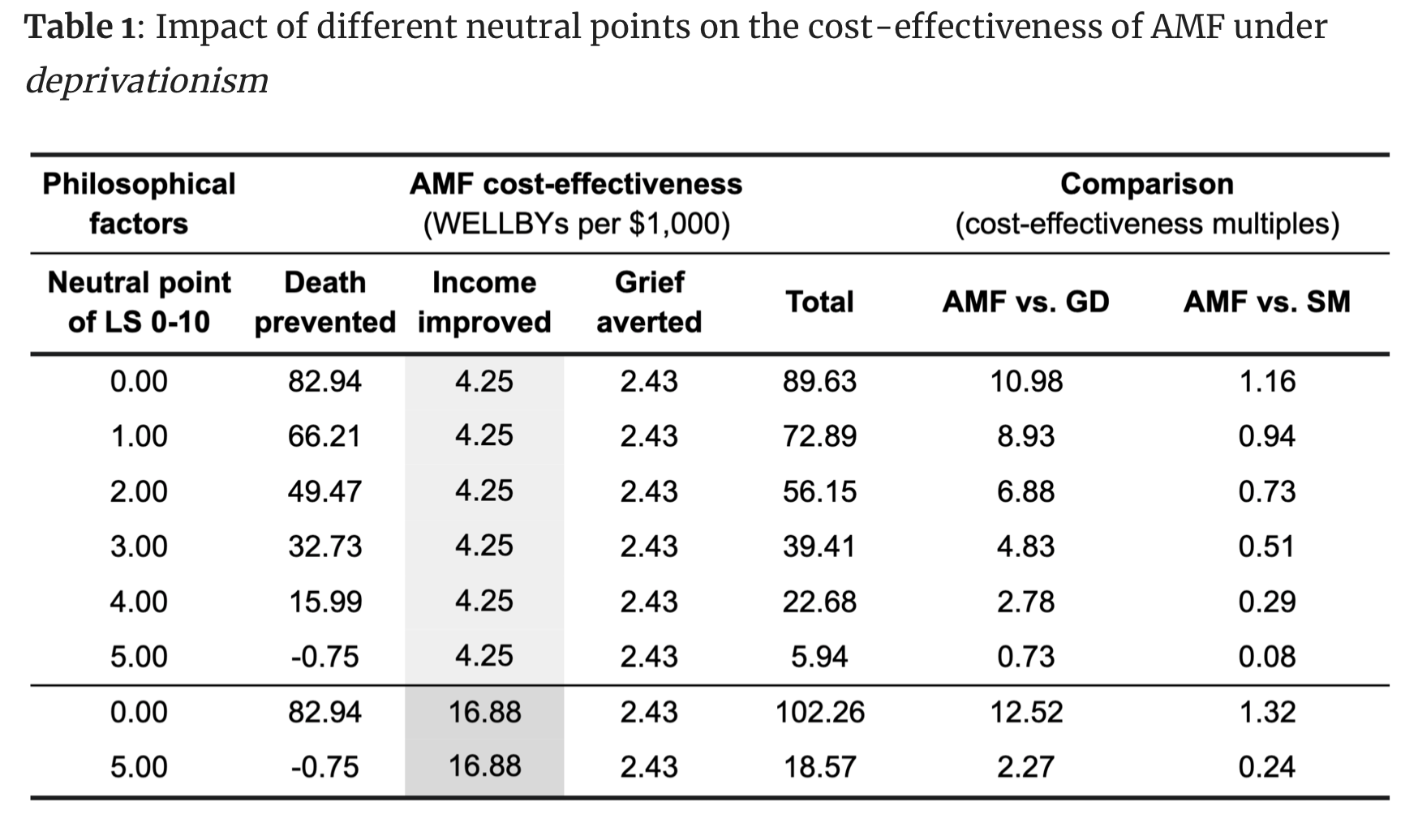
- The highest neutral point we think is plausible is 5/10 on a 0 to 10 wellbeing scale, but we mentioned that some philosophical views would stake a claim to the feasibility of 10/10.
- The highest value of a year of life we'd consider plausible is 10 WELLBYs a year (LS = 10/10 and neutral point = 0), and the lowest as -5 (LS = 0/10 and neutral point = 5).
- But if we're only accepting low-income country average LS values (~4/10 in our malaria report), then this would be -1 to 4.
- I think you can fill out the missing cells for HLI by taking the average age of death, which for Malaria I is ~2 for under 5's and ~46 for over 5s. Assuming a life expectancy of 70 (what we've assumed previously for malaria deaths), that'd imply a moral weight of under-5s = (70 - 2) * (-1 , 4) or (70 - 45) * (-1, 4).
- We haven't explicitly set out to estimate the wellbeing burden of depression, but this is an interesting question. I haven't thought too much about whether we can use our estimate of the benefit of treating depression with StrongMinds as an implicitly assigning a wellbeing weight to StrongMinds. I'm not sure this is as straightforward as it may appear.
- We are still developing our views on these moral weights, particularly around saving lives. To put it lightly, these are philosophically complex questions. Our present aim is to suggest what one should do, conditional on the moral view one holds. But perhaps surprisingly, this takes considerably more effort than assuming a viewpoint and seeing what follows.
- Granted, this has its limits. Our emphasis on subjective wellbeing is itself conditional on the primacy of theories of wellbeing that emphasise subjective states (e.g., hedonism, desire satisfaction).


It's awesome that you've put this together, as I think this is really valuable information. Honestly, what surprises me most here is how similar all four organizations' numbers are across most of the items involved.
As you pointed out, however, your use of the highest-possible value for HLI's value of extending a life by a year definitely undersells how different HLI is from the others. I think it would be better if you explicitly showed both endpoints of the range HLI considers, which includes negative values on the low end. Without that, I worry that readers who were otherwise not highly familiar with HLI's work would not come away with a correct impression of HLI's views.
I agree - and I started out trying to list all their approaches, but it very quickly becomes untractable in the table format. I have edited to show the full range, although I'm not sure if it's more or less helpful than before. Hopefully it does should how counter-intuitive their model can be
Thanks for the edit! I think that’s helpful
Is this because we argued that it's plausible that a life can have negative wellbeing?
This was also gratifying for us to see, but it's probably important to note that our approach incorporates weights from both GiveWell and HLI at different points, so the estimates are not completely independent.