Michael Plant, Joel McGuire, and Samuel Dupret[1]
Summary
How should we compare the value of extending lives to improving lives? Doing so requires us to make various philosophical assumptions, either implicitly or explicitly. But these choices are rarely acknowledged or discussed by decision-makers, all of them are controversial, and they have significant implications for how resources should be distributed.
We set out two crucial philosophical issues: (A) an account of the badness of death, how to determine the relative value of deaths at different ages, and (B) locating the neutral point, the place on the wellbeing scale at which life is neither good nor bad for someone. We then illustrate how different choices for (A) and (B) alter the cost-effectiveness of three charities which operate in low-income countries, provide different interventions, and are considered to be some of the most cost-effective ways to help others: Against Malaria Foundation (insecticide-treated nets), GiveDirectly (cash transfers), and StrongMinds (group therapy for depression). We assess all three in terms of wellbeing-adjusted life years (WELLBYs) and explain why we do not, and cannot, use standard health metrics (QALYs and DALYs) for this purpose. We show how much cost-effectiveness changes by shifting from one extreme of (reasonable) opinion to the other. At one end, AMF is 1.3x better than StrongMinds. At the other, StrongMinds is 12x better than AMF. We do not advocate for any particular view. Our aim is simply to show that these philosophical choices are decision-relevant and merit further discussion.
Our results are displayed in the chart below, which plots the cost-effectiveness of the three charities in WELLBYs/$1,000.[2]

StrongMinds and GiveDirectly are represented with flat, dashed lines because their cost-effectiveness does not change under the different assumptions. The changes in AMF’s cost-effectiveness are a result of two varying factors. One is using different accounts of the badness of death, that is, ways to assign value to saving lives at different ages; these three accounts go by unintuitive names in the philosophical literature, so we’ve put a slogan in brackets after each one to clarify their differences: deprivationism (prioritise the youngest), the time-relative interest account (prioritise older children over infants), and Epicureanism (death isn’t bad for anyone – prioritise living well, not living long). We also consider including two variants of the time-relative interest account (TRIA); on these, life has a maximum value at the ages of either 5 or 25. The other factor is where to locate the neutral point, the place at which someone has overall zero wellbeing, on a 0-10 life satisfaction scale; we assess that as being at each location between 0/10 and 5/10. As you can see, AMF’s cost-effectiveness changes a lot. It is only more cost-effective than StrongMinds if you adopt deprivationism and place the neutral point below 1.
1. Introduction
How should we compare the value of extending lives to improving lives? Let’s focus our minds with a real choice. On current estimates, for around $4,500, you can expect to save one child’s life by providing insecticide-treated nets (ITNs). Alternatively, that sum could provide a $1,000 cash transfer to four-and-a-half families living in extreme poverty ($1,000 is about a year’s household income).[3] The cost of both choices is the same, but the outcomes differ. Which one will do the most good?
This is a difficult and discomforting ethical question. How might we answer it? And how much would different answers change the priorities?
There are various methods we might draw on to make the comparison, such as health measures (DALYs and QALYs), subjective wellbeing measures (WELLBYs), or combining the judgements of experts, beneficiaries, and donors (e.g. GiveWell’s moral weights approach). However, whichever method we use, we must make some philosophical assumptions.
There are two philosophical issues that make a significant difference to the relative value of improving lives to extending lives. Specifically, these are: (A) an account of the badness of death, and (B) the location of the neutral point on a wellbeing scale. How we settle these two questions can change whether it's better to extend or improve lives.
Although there is philosophical literature on these topics,[4] they have received surprisingly little attention within the effective altruism community,[5] particularly given their potentially significant influence on decision-making. To address this issue, the charity evaluator GiveWell assigns ‘moral weights’ to deaths at different ages compared to doublings of consumption (see Figure 1). For instance, saving the life of a 5-to-9-year-old is deemed to have the same value as 134 years of doubled consumption. GiveWell derives these numbers by surveying its staff, its donors, and its beneficiaries and then weighting their answers (GiveWell, 2020). However, there is no public discussion of why - for what reasons, on what grounds - someone might choose one moral weight rather than another. Are these weights sensible? How could we tell? Nor is there discussion of how much difference this choice makes. Do ethical choices matter, or do you get essentially the same answer whatever ‘reasonable’ theoretical position you take?[6]
Figure 1: GiveWell’s disvalue of death at different ages in units of doubling consumption

Note: This graph comes from GiveWell (2020). Plant (2022a) discusses these weights in more depth.
This report is written for those who must make difficult choices between extending and improving lives and would like to have a better understanding of: (1) the theoretical choices they must make, (2) some of the reasons for making one choice rather than another; and (3) how much of a difference this could make. Our hope is that decision-makers will gain a better understanding of the issues and priorities that influence their decision rather than relying on opaque methods and recommendations made by others.
In section 2, we provide the theoretical background. We outline the two key issues, the options within them, and the advantages and disadvantages of those options.
In section 3, we put this theoretical machinery to work and show how the philosophical factors are decision-relevant by providing a novel cost-effectiveness comparison of three top charities.
In section 4, we set out our key uncertainties and directions for future research.
In section 5, we briefly conclude.
2. Philosophical issues in the valuation of extending lives
The standard metrics for combining quality and quantity of life are quality-adjusted life years (QALYs) and disability-adjusted life years (DALYs), two measures of health that were developed in the latter third of the 20th century (Sassi, 2006). On the QALY model, health states are modelled as values between 0 (death) and 1 (full health). For instance, two years lived at 0.5 would have a value of 1 QALY, as would one year of perfect health, and so on. This allows different health improvements to be quantified and compared in the same units. The DALY is essentially the same, but it is a measure of loss, rather than gain: 1 represents full disability and 0 represents no disability.[7] A principal motivation for the DALY was the Global Burden of Disease (GBD) study, which sought to quantify health trends and challenges worldwide (Salomon et al., 2012).
In the earlier (1990-2010) versions of the GBD, deaths were considered to be the worst for 10-year-olds. In the 2010-2015 version, the deaths of infants were considered worse than those of 10-year-olds, but stillbirths did not generate any disease burden (see Gamlud and Solberg, 2019, pp. 6-12 and references therein). This raises the question, ‘what is the worst age to die?’, and highlights issues that are referred to in the philosophical literature as the badness of death (Nagel, 1970; Feldman, 1992; Broome, 2004; Gamlud and Solberg, 2019). In section 2.1, we set out the three main accounts - deprivationism, the time-relative interest account, and Epicureanism - and show how the relative values of saving a life at different ages vary substantially between, and even within, them. In section 2.2, we turn to a further issue, that of the neutral point.
2.1 Accounts of the badness of death
Deprivationism (prioritise the youngest)
The more recent version of the GBD implies a deprivationist account of the badness of death.[8] On this, the badness of death consists in the difference between the wellbeing you actually had compared to how much you would have had if you’d lived longer. That’s why it’s better to save the youngest lives: they have more to lose than older ones. Two leading proponents are Broome (2004) and Bradley (2009).
Formulaically, the badness of death on deprivationism is:
wellbeing lost = wellbeing level x years of life lost
For example, if someone is expected to live 50 years at wellbeing level 1, then the badness of their death would be equivalent to 50 ‘units’ of wellbeing lost. We return to the issue of determining ‘wellbeing levels’, particularly in relation to a ‘zero’ level, in section 2.2.
The counter-intuitive aspect of this view is that it requires us to draw an awkwardly sharp line about the time at which death begins to be bad. If we draw the line at birth, then there would be no disvalue in ending a life immediately beforehand.[9] This problem is not removed by putting the line elsewhere.
The time-relative interest account (prioritise older children over infants)
An alternative, gradualist, approach is to say that death starts to be bad at a certain age but then becomes worse and reaches its peak badness at some later stage.
In philosophy, this position is associated with the time-relative interest account (TRIA) of the badness of death (McMahan, 2002). The idea behind TRIA is that the badness of death does not consist only of the wellbeing one would have had, but also in how psychologically connected the person is to their later self. As infants are only weakly psychologically connected to their later selves, their ‘interest’ in living may be less than that of an adult, even though the infant has more years to live.[10] This view takes inspiration from Derek Parfit’s work on personal identity and his conclusion that what prudentially matters in survival are certain kinds of psychological connectedness, rather than the physical continuity of our bodies (Parfit, 1986). TRIA could justify the stance taken in the earlier versions of the GBD on which saving 10-years-olds is more valuable than saving infants. It could also explain the intuitions many have that abortion is permissible - foetuses have comparatively limited interests compared to their mothers - and that earlier-stage abortions are less bad than later ones.
As we might expect, TRIA comes with its own theoretical challenges.
Here’s one problematic case.[11] A woman is pregnant. She can take a drug that will treat an illness but will cause substantial birth defects (a real-life example of this would be Thalidomide). According to TRIA, the mother would do little or nothing wrong in taking the drug because the foetus currently has quite weak interests in its own future. Intuitively, however, the mother should not take the drug.
If one accepts some sort of gradualist view, the further question is: how does it work, exactly?[12] As we saw in Figure 1 earlier, GiveWell - like the earlier version of the GBD - adopts a gradualist approach to saving lives, but this is not the only possible one. How much difference might it make to choose some version of TRIA relative to deprivationism?
We’ve illustrated some simple versions of TRIA in Figure 2 below, where psychological connectedness begins six months after conception and constantly increases until the ‘age of full connectivity’ occurs at 5, 15, or 25, after which it stays at its maximum level. In equation form, we can present the badness of death according to TRIA as:
wellbeing lost = wellbeing level x years of life lost x TRIA discount(age of death, age of connectivity)
Figure 2: The badness of death at different ages on deprivationism and versions of TRIA

As you can see, the value of saving a 5-year-old who would live 65 more years is worth 65 ‘happy years’ if the ‘age of connectivity’ (AC) is 5. However, it’s only worth 21 years (2/3rds smaller) if AC is 15, and worth 12 years (over 80% smaller) if AC is 25. Hence, there can be quite substantial differences in how to value a life, even within a gradualist approach. We do not aim to settle the question of which version of this view is best here, so much as notice their importance. For a discussion of what the view should be, see Norheim (2019), Mogensen (2019), and McMahan (2019).
Epicureanism (prioritise living well over living long)
The third account of the badness of death is Epicureanism, named after the ancient Greek philosopher Epicurus, who argued that death could not be bad for those who die on the grounds that nothing can be bad for us if we do not exist (Hicks, 2009). To be clear, Epicureans accept that dying can be painful and that a person’s death can be bad for others; they only deny that a person’s death can be bad for them. This view may seem implausible, given that we tend to think our own deaths would be bad for us, but Epicureans can raise three non-trivial puzzles for conventional views (Solberg, 2019):
- Experience: We often think that something cannot be good or bad for us unless we experience it. But, when we are dead, we cannot experience anything, so how can death be worse (or better) for us?
- Time: For something to be good(/bad) for us, there must be a time at which it is good(/bad) for us. But our future death is not bad for us whilst we are alive, and it is unclear how it is bad for us once we cease to exist.
- Symmetry: We don’t think that our non-existence before our lives harmed us, but there is no difference between not existing before and after our lives. Therefore, our after-life non-existence is not a harm either.
Philosophers disagree on whether and how these puzzles can be solved.[13] Although what we might call strong Epicureanism, the view that death is not bad at all, has few takers, there may be more sympathy for weak Epicureanism, where death can be bad, but relatively more weight is given to living well than living long.[14] In our later calculations, we only model strong Epicureanism.
The three views discussed in this section give very different accounts of the badness of death. The first two of these, deprivationism and TRIA, are illustrated in Figure 2 above. Epicureanism requires no illustration as there is no badness to death at any age. We will examine the implications of these views for charity evaluations in section 3.
2.2 The neutral point
In this section, we turn to another important philosophical choice, the location of the neutral point, the level of wellbeing that existence is neither good nor bad for someone. Why does this matter?
To compare life-improvements and life-extensions, we need to combine the quality and quantity of life into a single unit. We discussed how this can be done using QALYs and DALYs at the start of section 2: on the QALY, health states are usually between 1 (full health) and 0 (equivalent to death). The reason we need a measure of quality is because we’re not just interested in how long an intervention benefits someone, but also how much it benefits them. Any measure of the quality of life must include a neutral point. We need this to know how much better life is than some principled zero level. If we don’t know how much benefit people get from different outcomes, it’s impossible to allocate limited resources to do the most good. We discuss the idea that we should ignore quality of life when saving lives in a footnote.[15]
An initial issue with the neutral point is whether it even makes sense to say that lives can be bad. The QALY and DALY are both constructed by asking members of the public to make hypothetical trade-offs (e.g. how many years with illness X would be as good as Y years of full health?). One difference that is important, however, is that the QALY allows individuals to be in ‘states worse than death’ (SWD), whereas, on the DALY, death is the worst possible state (Gold et al., 2002; Weinstein et al., 2009).
What’s puzzling about the DALY approach is that we typically think it is possible to be in a state worse than death - a life of unrelenting misery and torture, for instance.[16] Part of the argument for legalising physician-assisted suicide is that death can, sometimes, be better for somebody. If living longer is always better, such an intervention could never be justified on cost-effectiveness grounds. By artificially inserting a ‘floor’ on how bad life can be, the DALY approach biases healthcare resources towards extending lives over improving lives.
Yet, what’s unsettling about the QALY approach is this implication: if people are in states worse than death, then it is bad to extend their lives, even if those people want to keep living and we could extend their lives for free. For this reason, Scheider (2021) considers the QALY objectionably ‘ableist’.
There are a couple of reasons why we might find it unsettling to say that saving lives is bad. Once we recognise those, it is easier to believe there are states worse than death.[17]
First, it seems like a double unfairness if we think that it’s a bad thing to provide life-extending support to unhappy lives: not only has the person been unlucky enough to end up in an unpleasant condition, but now, because of that, they won’t get life-extending medical care. It’s worth noting, however, that it would still count as valuable to provide life-improving care to those in ‘states worse than death’, so the QALY approach does not flatly rule out doing anything. Indeed, we often do have the intuition, at least for those who are suffering and at the end of life, that the priority is palliative care - making them comfortable rather than prolonging their lives at any cost.
Another explanation is that we don’t trust the accuracy of health measures. After all, these are typically created by asking members of the public to make hypothetical trade-offs, not by asking the people in specific health states how they feel about their own lives. For instance, Bernfort et al. (2018), looking at a cohort of elderly Swedes, find that although 1.8% are deemed to be in states worse than death (because they have health conditions assigned negative QALY weights), 45% of the people in that category said they were ‘happy’ or ‘fairly happy’ (55% said they were ‘not happy’). Perhaps the problem is not with the idea that there can, in theory, be states worse than death; rather, the issue is that the QALY health measure does not, in practice, do a good job of drawing the line in the right place.[18]
An obvious solution is to use subjective wellbeing surveys, individuals’ self-assessments of their happiness and/or life satisfaction, to work out how well or badly their lives are going. At the Happier Lives Institute, we have long argued for the use of subjective wellbeing measures, and for just this sort of reason (McGuire et al., 2022a; Plant, 2018). MacAskill (2022, Chapter 9) has recently argued for them too.[19]
However, this brings us to a further challenge. It’s unclear where to put the neutral point on different subjective wellbeing scales, and almost no research has been done on this topic (Donaldson et al., 2020; MacAskill, 2022). On life satisfaction scales, where 0 is typically marked as ‘not all satisfied’ and 10 as ‘completely satisfied’, there is no clear indication of what respondents should interpret as the neutral point.
Some wellbeing researchers are inclined to interpret 0 as the neutral point (Layard et al., 2020), but it’s unclear what the justification is for this. It runs into the same issue raised above for DALYs: it implies, implausibly, that people can only live good lives. Those who give themselves the lowest scores, 0 out of 10, would be assumed to have neutral lives.[20]
Other wellbeing researchers, such as Diener et al. (2018), appear to treat the midway point on the scale as the neutral point (i.e., 5 on a 0-10 scale). This might seem the more natural interpretation, but this also yields odd results. It suggests that a large share of the world’s population has negative wellbeing (average life satisfaction in Rwanda is around 3, for example). If we think the average Rwandan lives an overall good life, that might suggest: (1) the neutral point is below 5/10 on the life satisfaction scale; (2) life satisfaction is the wrong measure of wellbeing - perhaps we believe happiness is what matters, and Rwandans are happy, but not satisfied with life[21]; (3) wellbeing will increase in Rwanda, so saving the average life is positive in expectation, even if it isn’t right now; or (4) some combination of (1)-(3).
We might suppose, then, that the neutral point on the life satisfaction scale is somewhere between 0 and 5.[22] Yet, any particular choice here seems arbitrary - why 2 rather than 3, for instance? It also implies a ‘lop-sided’ scale where the negative end of the scale is shorter than the positive end. This clashes with the intuition that the worst possible lives are worse than the best possible lives are good. See Donaldson et al. (2020) for more details.
Empirical work on how individuals interpret the scale could be helpful but is extremely limited. A small (n = 75) survey in the UK found that respondents would choose death over life at a life satisfaction level of about 2/10 (Peasgood et al., unpublished, as referenced in Krekel & Frijters, 2021). A survey of people living in poverty in Ghana and Kenya estimated the neutral point as 0.56 (IDinsight, 2019, p. 92; n = 70). There are also preliminary results from a sample of 600 in the USA, Brazil, and China that finds a neutral point of 25/100 (Jamison & Shukla, private communication). At the Happier Lives Institute, we are currently working on our own survey to explore this topic further and hope to share our results soon.
In section 3, we do not take a position on where the neutral point is when making our calculations. Instead, we explore how different neutral points between 0 and 5 on a 0-10 scale affect the cost-effectiveness of life-improving and life-extending interventions.
How much difference could the location of the neutral point make if we use subjective wellbeing scales? We will say that 1 WELLBY (wellbeing-adjusted life year) is equivalent to a 1-point improvement on a 0-10 life satisfaction scale for 1 year. This is similar to how 1 year of life at full health is 1 QALY, except that wellbeing runs on a 0-10 scale, not a 0-1 scale. The location of the neutral point is irrelevant for improving quality of life: if Alice’s quality of life increases by 1 point for 2 years that is worth 2 WELLBYs. However, suppose that we can extend Bob’s life for 1 year and Bob rates his wellbeing at 6/10. If the neutral point were 5, this is worth 1 WELLBY. If the neutral point were 0, this is worth 6 WELLBYs. Clearly, this is a large difference.
This issue becomes sharper if our efforts to save lives focus on low-income countries where, as a consequence of lower prosperity, wellbeing levels are lower. Such individuals will be closer to the neutral point than those in high-income countries, and a non-trivial proportion may be below it. Although this thought is unpleasant it should not be surprising: if we aim to help those in poverty because we think poverty is very bad, then we must already accept that those in poverty have lower wellbeing.
When we’re assessing the value of extending a life in terms of wellbeing, we need to consider the change in net wellbeing. Take our formula for deprivationism:
wellbeing lost = wellbeing level x years of life lost
The existence of a neutral point implies that the wellbeing level refers to net wellbeing, that is, how much higher (or lower) wellbeing is than the neutral point (wherever it is).
3. How do philosophical assumptions change the cost-effectiveness of top charities?
In section 2 we discussed how philosophy influences the value of extending a life. In this section, we crunch the numbers to illustrate how much difference this could make. To do this, we compare three charities which operate in low-income countries and are considered to be some of the most cost-effective ways to help others. Two are life-improving charities: GiveDirectly, which provides cash transfers, and StrongMinds, which treats depression using group psychotherapy. The third, the Against Malaria Foundation (AMF), provides long-lasting insecticide-treated nets for protection against malaria; the main benefit of this is taken to be life-saving.[23]
We assess the cost-effectiveness of each charity using a subjective wellbeing (WELLBY) framework. We’ve argued that effectiveness should be assessed in WELLBYs in general (McGuire et al., 2022a). In this case, it’s unclear how else we could capture the benefits of cash transfers, bednets, and psychotherapy in any other common unit. What would we use? Wealth? Health? Effects on wealth might be a good way to assess the impact of cash transfers, but not those of being alive or depression-free. Equally, effects on health might capture the value of bednets and therapy, but presumably, the value of alleviating poverty isn’t just that it improves health.
To make this comparison, we combine and extend several earlier pieces of work. We’ve already estimated the cost-effectiveness of GiveDirectly and StrongMinds in WELLBYs. First, we undertook meta-analytic cost-effectiveness assessments of cash transfers and psychotherapy (McGuire & Plant, 2021a, McGuire & Plant 2021b). We then used those results to estimate and compare the cost-effectiveness of GiveDirectly and StrongMinds, which we consider as ‘best in class’ organisations for implementing each intervention (see McGuire & Plant, 2021c for the original comparison and McGuire et al., 2022b for an updated version which incorporates household spillover effects). We found that GiveDirectly’s cash transfers produce 8 WELLBYs/$1,000 and StrongMinds’ psychotherapy produces 77 WELLBYs/$1,000, making the latter about 10 times more cost-effective than GiveDirectly.[24]
We’ve also done an initial estimate of the relative values of doubling consumption and saving the life of a 5-year-old using a WELLBY approach (Donaldson et al., 2020). The main two additions in this report are: (1) we estimate cost as well as effectiveness; (2) we show how the results change under several different assumptions about the badness of death and the location of the neutral point.[25] In other words, now we’ve got some key pieces of the jigsaw puzzle we’re working out, for the first time, how they fit together.
There are two key findings.
First, the philosophical factors can radically alter the cost-effectiveness of life-extending interventions. On the assumptions most favourable to extending lives, AMF is about 30% more cost-effective than StrongMinds.[26] On the assumptions least favourable to extending lives, StrongMinds is around 12 times more cost-effective than AMF.[27] We unpack the details of this below. We consider these results noteworthy, and hopefully a useful corrective to the idea that philosophy is not an important factor in these choices.[28]
Second, these comparisons could be sensitive to the estimates of AMF’s life-improving effects. The two we consider are: (1) averting the grief of bereaved family and friends; and (2) an income-increasing effect: a reduced incidence of malaria, particularly in childhood, may help people earn more in later life. (1) is unproblematic; we estimate this to be 2.5 WELLBYs/$1,000, a non-trivial but relatively small factor. (2) is more challenging. Taking GiveWell’s income-increasing effects at face value, and converting them into WELLBYs, implies that (2) is about 17 WELLBYs/$1,000. This seems implausibly large. It implies that AMF (if we only count its income effect is 3x more cost-effective than GiveDirectly’s cash transfers, which directly aim to reduce poverty. After further analysis, we think a more realistic figure of the income effects of bednets is 4 WELLBY/$1,000, about a quarter of the size.[29] We explain how we reached this figure in Appendix A.
We will now show how we estimated the cost-effectiveness of AMF in WELLBYs, how this changes under different philosophical assumptions, and how it compares to GiveDirectly and StrongMinds. In the following three subsections, we consider the three different accounts of the badness of death and, where relevant, vary the neutral point.
3.1 Deprivationism results
We start with the simplest account, deprivationism. On this view:
badness of death = net wellbeing level x years of life lost
We assume that the average age of the individual who dies from malaria is 20 years old[30], they would expect to live to 70, and so preventing their death leads to 50 extra years.[31] We estimate their average expected life satisfaction to be 4.95/10.[32] Hence, the WELLBYs gained by the person whose death is prevented is (4.95 - neutral point) * (70 - 20).
According to GiveWell, it costs $3,000 for AMF to prevent a death (on average).[33] Before we calculate the cost-effectiveness, we must also add the life-improving effects of providing malaria prevention. We estimate the grief-averting effect of preventing a death is 7 WELLBYs for each death prevented (see Appendix A.2), so 2.4 WELLBYs/$1,000. We estimate the income-increasing effects to be 4 WELLBYs/$1,000 (see Appendix A.1).
We can now calculate the cost-effectiveness of AMF under different assumptions about the location of the neutral point. If the neutral point is zero, the value of preventing a death would become 4.95 * 50 = 247 WELLBYs; this gives a cost-effectiveness of 83 WELLBYs/$1,000. This, combined with the life-improving and grief-averting benefit of 7 WELLBYs leads to a total of 90 WELLBYs,/$1,000 which is represented in the first row of Table 1 below.
This result compares favourably to the cost-effectiveness of GiveDirectly and StrongMinds, which are 8 WELLBYs/$1,000 and 77 WELLBYs/$1,000, respectively. The interpretation of this multiple is that AMF, assuming deprivationism and a neutral point of 0, is 10.98 times as cost-effective as GiveDirectly and 1.16 times as cost-effective as StrongMinds. We represent these as cost-effectiveness multiples in the last two columns of Table 1.
In Table 1, you can see that as the neutral point increases, the cost-effectiveness of AMF decreases considerably. At a neutral point of 5, AMF generates negative WELLBYs from its life-extending effects; the positive cost-effectiveness is driven entirely by AMF’s life-improving effects. At a neutral point of 5, GiveDirectly is about 30% more cost-effective and StrongMinds over 10x more cost-effective than AMF. The last two rows show what happens if we take GiveWell’s numbers at face value, since they estimate that malaria prevention increases income to a greater extent than we do.
Table 1: Impact of different neutral points on the cost-effectiveness of AMF under deprivationism
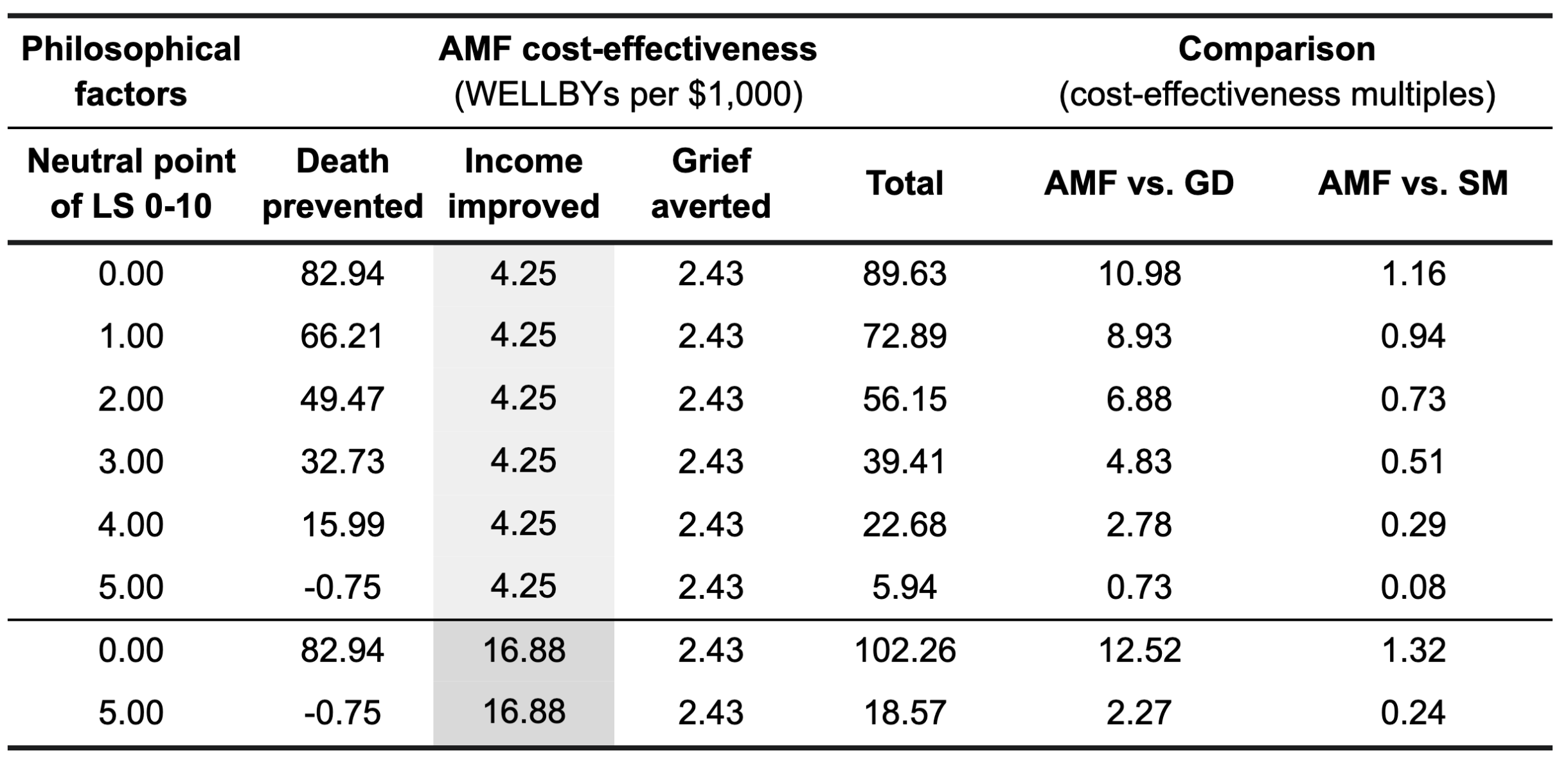
Note: A $1,000 donation to GiveDirectly (GD) produces 8 WELLBYs and a $1,000 donation to StrongMinds (SM) produces 77 WELLBYs. LS means a life-satisfaction scale.
3.2 TRIA results
We now turn to the time-relative interest account (TRIA) of the badness of death. Recall that TRIA captures the intuition that the badness of death depends, in part, on how psychologically connected someone is to their later self. This is why the deaths of very young children are less of a loss than older ones.
To produce this calculation, we need to stipulate the age that someone reaches ‘full connectedness’. In our model, we use a range of values between 5 and 25 years. This choice makes a lot of difference in this case because many of those who die from malaria are very young (see Figure 3 below).
Figure 3: Age at death from malaria using data from the Global Burden of Disease (2019)

Although 58% of people who die from malaria are under five years old, due to the large number of older people who die from malaria, the average age of death is 20 (see row 18). Therefore, we split the analysis into two, one for under-5s (who we model using the average age of those in that category, 1.5 years) and over-5s (who we model using the average age of that category, 46 years).[34] Given this, we assess the loss from the over-5 deaths in the same way as deprivationism; only the under-5 deaths are subject to a ‘TRIA adjustment’.
We don’t show all the possible combinations here, as there are too many to present. Instead, Table 2 displays combinations of the most and least generous assumptions about the neutral point and the age of connectivity, along with a middle option for both. As you can see, StrongMinds is more cost-effective than AMF in every case (between 1.1 to 12.5 times better) and GiveDirectly is less cost-effective than AMF except under the assumptions least favourable to extending lives. Again, we’ve added two final rows to indicate the difference it makes if we use GiveWell’s larger value for life-improving effects.
Table 2: Cost-effectiveness of AMF compared to life-improving charities under TRIA
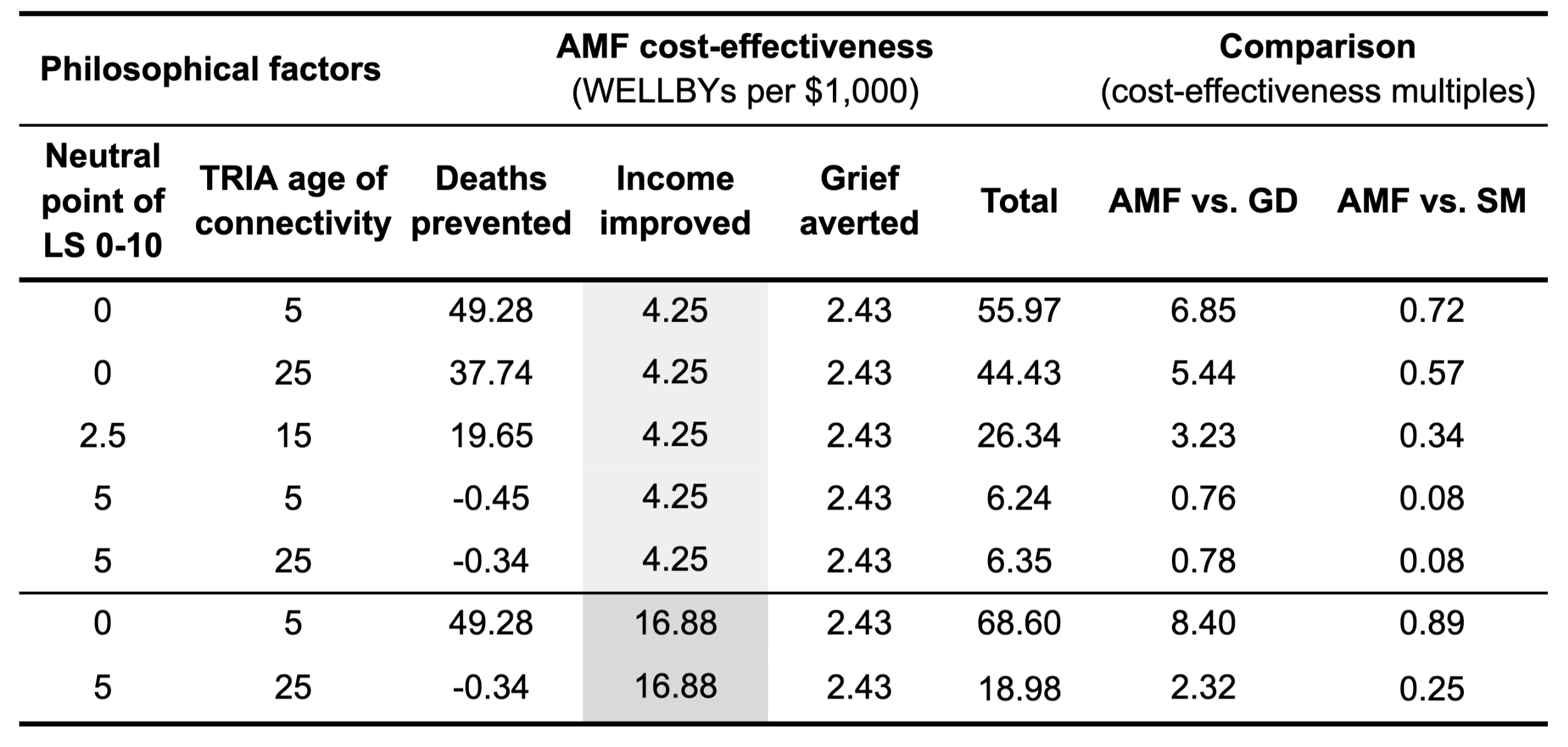
Note: A $1,000 donation to GiveDirectly (GD) produces 8 WELLBYs and a $1,000 donation to StrongMinds (SM) produces 77 WELLBYs. LS means a life-satisfaction scale.
3.3 Epicureanism results
For the person dying, the badness of death under Epicureanism is zero and, therefore, the choice of neutral point is irrelevant. For Epicureans, the effect of AMF’s malaria prevention comes from its grief-averting and life-improving impact of 6.7 WELLBYs (see Table 3 below). Unsurprisingly, AMF is less cost-effective than GiveDirectly and StrongMinds in this case. As before, we’ve indicated how much difference it makes if the life-improving effects of malaria prevention are as large as GiveWell’s estimate implies.
Table 3: Cost-effectiveness of AMF compared to life-improving charities under Epicureanism

Note: A $1,000 donation to GiveDirectly (GD) produces 8 WELLBYs and a $1,000 donation to StrongMinds (SM) produces 77 WELLBYs. LS means a life-satisfaction scale.
3.4 Summary of results
In Figure 4, we show how the cost-effectiveness of the three charities (in WELLBYs/$1,000) changes according to the combination of philosophical views.
Figure 4: Cost-effectiveness of charities under different philosophical assumptions

As we can see, AMF is more cost-effective than StrongMinds, but only by a small amount, and only on the assumptions most favourable to saving lives: if you accept deprivationism (the yellow line) and think the neutral point is less than 1. On assumptions of higher neutral points and/or different accounts of the badness of death, AMF’s cost-effectiveness drops away until it becomes about 12x less cost-effective than StrongMinds and has about the same cost-effectiveness as GiveDirectly. AMF never ends up much less cost-effective than GiveDirectly on our estimates due to the non-trivial life-improving effects of bednets from averting grief and increasing later income.
4. Key uncertainties and directions for future research
In the previous section, we showed how much difference it can make if we adopt different philosophical assumptions. This raises questions for further work.
Which account of the badness of death is most plausible? We have not argued for one account in particular, so much as briefly motivated them and raised some issues. Given these are long-standing debates (again, see Gamlund and Solberg 2019), it’s unclear how useful it would be for us to try to evaluate these views ourselves, rather than merely understand what the implications are of taking one or another position and communicating this to readers.
Where is the neutral point? We think the neutral point is under-theorised and under-investigated. There has only been initial empirical work (see section 2.2) and we plan to run a larger survey (n>1000) which could shed more light on how people interpret subjective scales.
How big are AMF’s life-improving effects? As flagged several times, these could be quite large, and our investigation into them has only been fairly shallow. However, we’re unsure how much to prioritise this, given they are a relatively smaller issue than the philosophical ones.
How should we deal with moral uncertainty? We’ve shown that the philosophical assumptions matter and we expect readers are unlikely to be 100% confident in a single approach. How should we account for this uncertainty? ‘Moral uncertainty’ is a new, important, and complicated topic at the frontiers of academic philosophy. We don’t have space to get into this in any depth here, but we will sketch the three approaches that seem to be on the table. We intend to return to this and write some guidance for donors and decision-makers.
- My Favourite Theory: Choose the action recommended by which moral view you have the most credence (i.e. confidence). If you had, say, the greatest credence in deprivationism and a neutral point of 0/10, then you should choose whatever is best given those assumptions: in this case, AMF.
- Maximise Expected Choiceworthiness: Construct a weighted average of each option based on your credences in the different views and how good the option is on each view; you then choose the option that maximises expected chioceworthiness. In this case, you would award 100% of your resources to whichever life-improving or life-extending option was best. We don’t run any numbers here: it should be clear from Figure 1 that the top life-improving option will be better unless one has the overwhelming weight of one’s credences in both deprivationism and a very low neutral point.
- Worldview Diversification (Karnofksy, 2016): Divide your resources across different theoretical ‘buckets’ in proportion to your confidence in each theory, then choose the best option for each ‘bucket’. For example, if you have 30% credence in deprivationism and 100% credence that the neutral point is below one, you should award 30% of your resources to AMF and the rest to StrongMinds.
(1) and (2) are discussed at length in the existing philosophical literature (Bykvist, 2017, MacAskill, Bykvist, Ord 2020), whereas (3) has received little attention (see Plant, 2022b and Lloyd, 2022 for explorations and tentative defences).
5. Conclusion
Two key philosophical issues seem to have barely featured in discussions about whether resources do more good if we prioritise extending or improving lives. They have, however, been there all along. And they can make a big difference to cost-effectiveness calculations and our conclusions about what the overall priority is. It’s reasonable to disagree about these theoretical issues, so it’s essential to bring these underlying assumptions to the surface. We do not have simple answers to the problems we raise - nor do we think there are any - but we hope we have clarified them and set the stage for further work.
Appendix A: Estimating the life-improving effect of bednets
In this appendix, we explain how we estimate the SWB life-improving benefits of malaria from increased incomes for the recipients of bednets and averted grief for their loved ones.
A.1 Converting from economic benefits to WELLBYs
To estimate the effects of malaria prevention on subjective wellbeing (SWB), we would like to use direct evidence of the causal effect of malaria prevention on SWB but we found no reliable data for this.[35] The data used in some of the causal studies of malaria prevention’s effect also includes SWB variables (Shih & Lin, 2019; Rawlings, 2016; Mora-García, 2018; Venkataramani, 2012). However, we have not found an SWB analysis that uses these datasets.
Instead of using SWB evidence directly, we convert from malaria prevention’s estimated economic benefits to WELLBYs. GiveWell estimates that spending $1,000 on AMF’s malaria prevention programme increases economic benefits by 18 log-units (or about 13 doublings of income, row 247, “Modified” tab). McGuire et al. (2022c) explains how GiveWell arrived at these figures and argues why these effects on income are likely to be smaller and less certain than GiveWell’s estimates.
We translate the economic benefits into WELLBYs by estimating what a log-unit increase in economic benefits predicts in WELLBYs. To estimate this figure, we use the model in our cash transfers meta-analysis where we moderate the SWB effect of cash transfers by the relative size of the transfer compared to previous income (Model 2 in Table 2 of McGuire et al., 2022d). We calculated the total benefits in SD-years using the ‘area of the triangle’ formula as illustrated and described in Figure 1 of McGuire and Plant (2021a). Since a 1-unit increase in log-economic benefits is approximately a 70% increase in household income, plugging a 70% increase in income (1 log-unit) into Model 2 from Table 2 (McGuire et al., 2022d) leads to a 0.6 SD-year increase in SWB (row 23, “Inputs” tab). To convert from SD-years to WELLBYs we multiply the SD-years by the average SD of life satisfaction (2.17, see row 8, “Inputs” tab), which results in 0.6 x 2.17 = 1.3 WELLBYs. If we take these numbers at face value, $1,000 donated to AMF’s malaria prevention programme creates 18 x 1.3 = 23 WELLBYs due to income-increasing effects. Note that this includes household spillovers because GiveWell includes household spillovers in their figure. In GiveWell’s analysis, non-recipients receive a benefit that is 25% of the benefit received by the recipient. This is equivalent to GiveWell’s 2x household multiplier for households of four (row 120, “Modified” tab).
However, there’s a key difference between the way that cash transfers and malaria prevention increase incomes. When it comes to increases in income, part of the SWB benefit may be due to a comparison effect - comparing yourself with others and finding yourself better or worse off (Clark et al., 2018; Easterlin, 2021). Comparison effects apply to cash transfers, but they probably do not apply to malaria prevention. With mass distribution of bednets, the benefits accrue to everyone in an area, while cash transfers are only sent to the poorest. We estimate that these comparison/relative income effects comprise 26% of the total income effect.[36] Including this adjustment discounts the life-improving effect of malaria prevention from 23 down to 17 WELLBYs.
The final step is to incorporate various further discounts to AMF’s income effects that we proposed in our recent essay critiquing GiveWell’s CEAs (McGuire et al., 2022c). We won’t restate all those details here, but the short version is that we identified several issues with GiveWell’s calculations. We estimate that, cumulatively, this leads to a 75% reduction in the income effect relative to what GiveWell estimates (row 35, sheet “Inputs”), or a (1 - 0.75) x 17 = 4 WELLBY effect. To frame this effect, we compare it to the other charities we’ve analysed in Figure A1 below.
Figure A1: Life-improving effect of charities in WELLBYs

A.2 Grief spillovers
We do a shallow calculation for grief in the same way we did in Donaldson et al. (2020). The best estimate we found is from Oswald and Powdthavee (2008): a panel study in the UK which finds the effect on life satisfaction due to the death of a child in the last year as being -0.72 (adjusted for a 0-10 scale). According to Clark et al. (2018), the duration of grief is ~5 years. Based on data from the UNDP, we calculate that the average household size across the beneficiary countries (excluding the recipient of the nets) is 4.03 people (row 16). Hence, an overall effect of grief per death prevented is (0.72 x 5 x 0.5) x 4.03 = 7.26 WELLBYs. However, we think this is an upper bound because it doesn’t account for the counterfactual grief averted. If you avert the death of someone, they will still die at some point in the future, and the people who love them will still grieve.
- ^
Michael Plant originated the idea, undertook the philosophical research and wrote the final draft. Joel McGuire performed the quantitative analysis and wrote the initial draft of the report. Samuel Dupret assisted with the quantitative analysis and provided feedback on earlier drafts.
- ^
1 WELLBY is equivalent to a 1-point increase on a 0-10 life satisfaction scale for one year. For example, going from 5/10 to 6/10 for one year.
- ^
This is the case for household income of the poorest 10% in Guinea, Chad, Uganda, Togo, Nigeria, and the Democratic Republic of Congo (see row 258 of “Modified” tab for calculations).
- ^
See Gamlud and Solberg (2019) for a recent, excellent compendium on the philosophical issues applied to health policy that we draw on several times in this report, Luper (2019) for a general overview and this PhilPapers archive for a list of hundreds of paper on the topic.
- ^
For mentions in an effective altruist context, see Plant (2016; 2019, Chapter 3), who sketches arguments that philosophical issues could make a very substantial difference to choosing between life-extending and life-improving interventions. Cotra (2016), writing for GiveWell, responds and objects to Plant (2016). Donaldson et al. (2020) estimate the relative values of doubling consumption and saving the life of a 5-year-old using a wellbeing-adjusted life year (WELLBY) approach. They emphasise that switching from one view of the badness of death (deprivationism) to another (the time-relative interest account) would reduce the value of saving 5-year-olds by a factor of five, a substantial difference. Donaldson et al. (2020) does not estimate the cost-effectiveness of any charities or say much about the different philosophical theories and how the cost-effectiveness estimates of charities change under these assumptions. These are things we do in this report.
- ^
Note some discussion of GiveWell’s moral weights on this recent EA forum post.
- ^
For our purposes, the differences are not important. See Sassi, 2006 for a discussion.
- ^
This is sometimes called the life comparative account. Arguably, this would be a more appropriate name, but we stick with the conventions of the literature. The rival view to (what we’ve called) deprivationism is the time-relative interest account, but both agree that death is bad because it deprives you of the goods of life. Hence, to call the former the life comparative account would make it easier to distinguish it from the latter.
- ^
This is more puzzling when we consider that birth is a matter of geography – when an entity moves from inside to outside the mother. Is it worse to end the life of a 35-week child outside the womb or a 36-week child inside the womb? Although we use different words to describe these - infanticide and abortion, respectively - we might wonder if there is an important moral distinction between them.
- ^
As Holtug (2010) explains it, “foetuses and infants usually have rather simple psychologies and thus few of the preferences, memories and character traits they will acquire later in life”.
- ^
For some others, see the edition collected by Gamlud and Solberg (2019), especially the chapter by Hilary Greaves.
- ^
Specifically: How exactly should we model the gradually-increasing value of a life? When does someone develop an ‘interest’ in continuing to exist? How does this interest grow? Does it increase constantly, or does it vary with stages of development? When does it reach its peak?
- ^
- ^
As the army sergeants used to say in the drill training of one of the authors: “I’m here for a good time, not a long time”.
- ^
Some are tempted to argue that we should give the same value to saving lives, regardless of the wellbeing those lives would have. See Open Philanthropy (2021, 5.2) and Plant (2022) for a reply, which we recapitulate here.
Although it’s appealing to say that extending a life has the same value, whoever’s life it is, the problem is making this consistent with other beliefs we are likely to have. If we think it’s better to save someone in their 20s than in their 70s, then we already think it’s correct to account for the quantity of life. Presumably, we also agree it’s better to cause a bigger increase in quality of life than a small one. So, how can it be consistent to value quality when improving lives, and quantity when extending lives, but not quality when extending lives?
The QALY and DALY frameworks combine quantity and quality into a single figure because the aim is to cause the largest benefit with the available resources. What’s more, if we ignore quality of life when valuing the extension of life, that will lead to other problems. If something extends someone’s life and improves their quality of life, e.g. a surgery to remove a painful tumour, what is the value of that? Do we ignore the improvement to quality of life? How would we compare the value of that to a similar surgery, that only improved quality of life?
Another important point to make is that, in saying it’s better to save one life than another, we are not saying one person has greater intrinsic worth than another. Rather, the claim is that the people have the same intrinsic worth, but one gets a greater benefit than the other, and that’s what matters. It’s better to alleviate two days of pain for Alice than one day for Bob because Alice and Bob have the same moral worth, but Alice benefits more.
- ^
In a survey of 667 Irish respondents, 67% disagreed with the statement “If I were severely ill with no hope of recovery, I would want to be kept alive at all costs” (McCarthy et al., 2010). Out of 1,081 doctors surveyed, 88% said they do not wish to be resuscitated if their heart stops (Periyakoil et al., 2013).
- ^
Another is to draw a distinction between what we ought to do and what’s good. Perhaps we ought to save people’s lives if we can do so costlessly, even if doing so would be bad for them. A further question would be how to balance this duty against our duty to do good.
- ^
If we genuinely believe someone has negative wellbeing, then it may seem appropriate, in line with the standard medical principle of triage, to prioritise extending the lives of those with positive wellbeing instead. After all, they will benefit more.
- ^
In response to the question of how to assess whether people’s lives are overall positive or negative, he concludes, “the answer is to rely primarily on people’s self-reports”.
- ^
It seems the main advantage of placing the neutral point at 0/10 is that it avoids giving too little to extending lives, but we also want to avoid giving too much value to extending lives.
- ^
Indeed, 90% of Rwandans attest that they are ‘happy’ or ‘very happy’ (OWID, 2022). Unfortunately, the data on happiness is much sparser than life satisfaction data.
- ^
- ^
Malaria is a disease due to Plasmodium parasites transmitted by infected female Anopheles mosquitoes. In 2020, there were an estimated 627,000 deaths due to malaria (WHO, 2021).
- ^
Our previous results (McGuire et al., 2022b) are in standard deviation changes over time (SD-years) of subjective wellbeing gained. Since these effects are standardised by dividing the raw effect by its SD, we convert it into life satisfaction points by unstandardising it with the global SD (2.2, see row 8) for life satisfaction (Our World in Data). Crucially, we assume a one-to-one exchange rate between a 1 SD change in affective mental health and subjective wellbeing measures. We’re concerned this may not be justified, but our investigations so far have not supported a different exchange rate.
- ^
Previously, we compared deprivationism to one version of TRIA and assumed the neutral point was around 2.5/10.
- ^
Assuming deprivationism and a neutral point of 0/10
- ^
Assuming Epicureanism or a neutral point of 5/10.
- ^
- ^
This reduction is the result of incorporating all the discounts we propose to AMF’s income effects in our recent essay critiquing GiveWell’s CEAs (McGuire et al., 2022c; row 35, “Inputs” tab).
- ^
See row 18 of our copy of GiveWell’s data regarding the age of death for malaria victims.
- ^
To estimate the expected lifespan of malaria victims if they didn’t die, we use data from the World Bank (2020). While the average lifespan for the countries AMF operates in is 59 years (row 252; World Bank, 2020), UN projections expect this to increase by 11 years in the next 40 years. Therefore, we expect the average lifespan to increase to 70.
- ^
In the countries that AMF operates in, the average life satisfaction is 4.5/10 (row 251). We speculate that those typically surveyed are in the upper half of income and those served by AMF are in the bottom. There’s a ~0.5 life satisfaction difference in African countries between the upper and lower half (OWID, 2020). These assumptions imply that the life satisfaction of AMF’s recipients is closer to 4. However, life satisfaction has been increasing in these countries in the past two decades. Using data from OWID (2020), we selected the life satisfaction data from the countries served by AMF from 2004 to 2020. We modelled life satisfaction as a linear increase over time which suggests a significant increase of 0.04 points each year (p < 0.001). To estimate the expected wellbeing for the rest of the beneficiaries' lives, we used the wellbeing we expect them to experience at the midpoint between their current age and life expectancy.
- ^
We use data from GiveWell’s cost-effectiveness analysis of AMF’s malaria prevention programme (see our modified copy of their spreadsheet). GiveWell estimates that AMF prevents 0.34 deaths per $1,000, (see rows 245-246; based on Pryce et al., 2018). Note that we haven’t checked this number. Our results for GiveDirectly and StrongMinds are in ‘per $1,000’, so we normalise the benefits of AMF to a per $1,000 basis.
- ^
To calculate the TRIA discount, we take the average age of the under-5s (1.5 years old) and weight it by the proportion of under-5 deaths (58%). Note that when we ran this analysis in R by simulating this age distribution our results did not change significantly.
- ^
We looked at two sources of direct evidence on SWB effects as sanity checks but did not update much on them.
Two natural experiments in Ghana and Colombia (Pasha et al., 2019; Carrillo, 2020) found that increased rainfall around the time of a child’s birth led to them having a higher likelihood of mental health issues later in life (20+ years later). Both papers argue from correlational evidence that this appears to be through an increase in mosquito-borne diseases (such as malaria). But neither of the studies pin down a causal link that runs through malaria prevalence. But according to Oheneba-Dornyo et al. (2022), for every 1 mm increase in rainfall, there's an additional case of malaria two months afterwards. If rainfall increases by 79 mm (the SD of rainfall in Ghana) the predicted increase in the population with malaria cases will only be 0.1%. Also, rainfall seems too weakly related to malaria to be a primary driver of this effect, so we are very uncertain about this evidence. That seems insufficient to explain the rainfall shocks as a malaria story.
The second source of evidence we considered involves cerebral malaria. In ~1% of malaria cases, the malaria attacks the brain (Idro, 2010), which can result in mental debilitation. There’s correlational evidence on small sample sizes that ~1 year after being infected with malaria, children with cerebral malaria have a greater likelihood of showing signs of a behavioural disorder (odd ratio: 8.5, Christensen & Eslick, 2015) or a mental disorder when compared to a control group of healthy kids (Ssenkusu et al., 2016; Bangirana et al., 2011; Boivin et al., 2018). But due to cerebral malaria’s rarity, we think that preventing this would only constitute a small benefit. Neither of these separate strands of evidence update us much about the plausibility of the SWB effect of malaria exposure in childhood.
- ^
The approach we took to estimate the importance of relative income effects was to see how much the magnitude of the absolute income coefficient decreases when you introduce a relative income coefficient (comparing yourself to your peers) to the equation. We interpret this ratio of coefficients (absolute income coefficient after / absolute income coefficient before the introduction of the relative term) as the share of absolute income effects from the total income effects. This is 74% for Reyes-Garcia et al. (2015), a study whose sample seems similar to that of the beneficiaries of AMF. The average income in the AMF countries in 2021 is $1,171 (row 256, “Modified" tab), and the average income is $1,062 for Reyes-Garcia et al. (2015). Relative income effects will likely grow with total income.
The Economist, last week: "[EA] doesn’t seriously question whether attempting to quantify an experience might miss something essential about its nature. How many WALYs for a broken heart?" (Nov 2022, Source)
HLI, this week: "...Hence, an overall effect of grief per death prevented is (0.72 x 5 x 0.5) x 4.03 = 7.26 WELLBYs"
Great article – well done!!!
Well, if we think feelings matter, we should try to quantify them in a sensible way. That's what we try to do.
But I share the sentiment that you really do miss something if you try to quantify feelings by measuring something other than feelings, such as income.
I don't think this is accurate. In explaining the wrong of pre-natal injury (which causes harm to the future adult), McMahan writes that "we must evaluate the act in terms of its effect on all those time-relative interests it affects, present or future." (The Ethics of Killing, p. 283.) That is, while the pre-natal being has little or no time-relative interest in avoiding the pre-natal injury, the future adult's time-relative interests would be gravely affected (we may suppose), which explains why the pre-natal injury is a morally weighty affair. (In case of pre-natal death, by contrast, there are no future time-relative interests to be negatively affected; the death prevents those interests from arising in the first place.)
You outline a moral dichotomy between the following:
It seems to me that longtermism explicitly rejects this dichotomy, because longtermists believe the prevention of the occurrence of the interests of innumerable future people would be a catastrophic moral loss. A believer in this dichotomy would argue that a human extinction event is morally neutral with respect to the interests of innumerable future people who would have lived, because the extinction event simply "prevents those interests from arising in the first place". Do you agree that this dichotomy is inconsistent with longtermism?
Not exactly -- though it is a good question!
The dichotomy merely suggests that failing to create a person does not harm or wrong that individual in the way that negatively affecting their interests (e.g. by killing them as a young adult) does. Contraception isn't murder, and neither is abstinence.
But avoiding wrongs isn't all that matters. We can additionally claim that there's always some (albeit weaker) reason to positively benefit possible future people by bringing them into a positive existence. So there's some moral reason to have kids, for example, even though it doesn't wrong anyone to remain childless by choice.
And when you multiply those individually weak reasons by zillions, you can end up with overwhelmingly strong reasons to prevent human extinction, just as longtermists claim. (This reason is so strong it would plausibly be wrong to neglect or violate it, even though it does not wrong any particular individual. Just as the non-identity problem shows that one outcome can be worse than another without necessarily being worse for any particular individual.)
I'm currently taking a class with Jeff McMahan in which he discusses prenatal injury, and I'm pretty sure he would agree with how you put it here, Richard. This doesn't affect your point, but he now likes to discuss a complication to this: what he calls "the divergent lives problem." The idea is that an early injury can lead to a very different life path, and that once you're far enough down this path—and have the particular interests that you do, and the particular individuals in your life who are important to you—Jeff thinks it can be irrational to regret the injury. So, if someone's being injured as a fetus leads them to later meet the particular life partner they love and to have particular the children they have, and if their life is good, Jeff thinks they probably shouldn't regret the injury—even if avoiding the injury would have led to their having a life with more wellbeing. That's because avoiding the injury would have led to them having particular people and interests in their life which they don't in fact care about from their standpoint now. However, Jeff does add that if an early injury makes the later life not worth living, or maybe even barely worth living, then the future person who developed from the injured fetus does have reason to regret that injury. He would say that children of mothers who took Thalidomide have reason to regret that.
Hello Richard. I'm familiar with the back-and-forths between McMahan and others over the nature and plausibility of TRIA, e.g. those in Gamlund and Solberg (2019) which I assume is still the state of the art (if there's something better, I would love to know). However, I didn't want to get into the details here as it would require the introduction of lots of conceptual machinery for very little payoff. (I've even been to a whole term of seminars by Jeff McMahan on this topic when I was at Oxford)
But seeing as you've raised it ...
As Greaves (2019) presses, there is an issue of which person-stages count:
Whichever choice the TRIA-advocate makes, they will inherit structurally the same issues for those as one finds for the equivalent theories in population ethics (for those, see Greaves (2017)).
The version of TRIA you are referring to is, I think, actualist person-stage version: if so, then the view is not action-guiding (the issue of normative invariance). If you save the child, it will have those future stages, so it'll be good that it lived; if you don't save the child, it won't, so it won't be bad that it didn't. Okay, should you save the child? Well, the view doesn't tell you either way!
The actualist version can't be the one at hand, as it doesn't say that it's good (for the child) if you save it (vs the case where you don't).
I am, I think, implicitly assuming a present-stage-interest version of TRIA, as that's the one that generates the value-of-death-at-different-ages curve that is relevantly different from the deprivationist one.
Just to clarify, is the only benefit you're considering from AMF a longer life for a few people, or are you also taking into account all the people who don't get sick from malaria?
Yes, we try to account for the benefit that'd accrue to everyone who doesn't get sick. We mention this at the beginning of Section 3 and discuss the calculations in more detail in the appendix. Overall we think these "life improving" (as opposed to "life extending") effects are relatively small. And if malaria prevention is cost-effective (which we argue depends on your philosophy), then I think it'll be the life-extending benefits that drive that.
Currently, we're primarily relying on evidence about how malaria prevention increases incomes -- and then converting that into estimates of how it'd affect people's subjective wellbeing. We're currently missing good data on how malaria prevention affects people's feelings.
It looks like you're only accounting for increased incomes and avoided grief when estimating the effects of AMF other than on the people who would have died. Have you looked at all about trying to account for all the factors GiveWell lists under supplemental adjustments in their CEA? Just to take an example, GiveWell increases AMF's benefits 9% to account for the reduction in malaria morbidity (time spent ill). If you take out the benefits from averted deaths, the morbidity effect is still 9% of the original benefit, not 9% of the new lower benefit. I would think that (and the other supplemental adjustment effects) might moderately shift your conclusions if you aren't currently accounting for them.
We already include GiveWell's adjustments, including their supplemental intervention adjustments in the lives saved and income-generated figures we use (and then adjust in the case of the income effects).
I guess I'm not quite sure what to make of your answer here. To take a concrete example, when computing AMF's cost-effectiveness in an Epicurian framework, how many WELLBYs/$1k are you attributing to reduced morbidity?
This is implicitly 0.42 WELLBYs per $1k if we go with the HLI adjusted figures, or it's 1.67 WELLBYs per $1k if you take GiveWell's income figures at face value.
Again, GiveWell doesn't explicitly model the morbidity effects other than by inflating the value of malaria prevention's life-saving and income-increasing effect by 9%. We didn't tinker with the supplemental charity-level adjustments, supplemental intervention-level adjustments or their leverage/funging adjustments because that is, I expect, a whole can of worms. Because we kept these adjustments that GiveWell uses to tweak the value of income and life -- the morbidity effects that GiveWell implicitly incorporates, we implicitly include it as well.
Basically, if you think that the morbidity effects should merit a different adjustment than 9%, we don't account for that. If you're satisfied with 9%, then it's already accounted for, just in a weird opaque way as part of GiveWell's suite of subjective adjustments.
Thanks for the response! If I'm understanding you right, then I'm not convinced I like your approach to this specific aspect of the model. But I do think any approach to handling the morbidity benefits is going to be very coarse without a lot of further research.
To try and illustrate my concern, let me just give a quick example for the DRC, working in GiveWell's units of value rather than WELLBYs (because that's what I'm more familiar with). If we take GiveWell's estimate that the morbidity reduction is equal to a 9% of AMF's pre-adjustment benefits, that means that per $100000, morbidity reduction generates 0.09*8570 = 771 units of value.
Based on how I think you're doing it, when you go to calculate the non-life-extension benefits of AMF, you compute the benefits of morbidity reduction as 9% of (development benefits + avoided bereavement). If we just work with GiveWell's numbers (which don't include the bereavement effects), that would be 0.09*2582 = 232 units of value/$100000. Then when you go to calculate the life-extension benefits, you add in a 9% adjustment for morbidity reduction, which is 0.09*5987 = 539 units of value/$100000. But that bookkeeping doesn't make any sense, as all the morbidity benefits should be accounted for in the non-life-extension category. Doing it the way I think you are, where you're adding a factor of 0.09 to all benefits, ends up making AMF look worse in the Epicurean case, as well as in all cases with a higher neutral point for happiness.
This is actually even more important because you're applying such a big downward adjustment to GiveWell's numbers. If we divide GiveWell's estimate of the development benefits by 4, then the development benefits are about 709 units of value/$100000 and the total morbidity reduction benefits under GiveWell's assumptions are 9% of the new total, or 597 units of value/$100000. If you do the bookkeeping how I think you're doing, only 58 units of value/$100000 of morbidity reduction would get attributed to the non-life-extension benefit category. Correctly attributing all 597 units of value/$100000 from morbidity reduction nearly doubles the estimated non-life-extension benefits of AMF.
I recognize that to some extent we're working with made-up numbers here. But I think the general point that the supplemental adjustments need to be handled with care when doing this kind of component analysis is an important one. However, I do apologize in advance if I'm misunderstanding how you're approaching this right now.
Thanks Joel!
This is great work, and I think it's super valuable to everyone thinking about the best ways to go about improving global health and wellbeing. I wanted to share a couple comments on it as well as a couple specific questions.
First, I think it's really good you're looking at these questions in so much detail despite the fact that they can feel unpleasant or difficult. I personally think that there's something pretty screwed up about the world when a random upper-middle class person in the United States can choose whether someone in Sub-Saharan Africa lives or dies depending on the choice of how much and where to donate. But given that's the world we live in, I think it's really important to do our best to try and figure out answers to these kinds of moral questions you're looking at. (Note: I also think it's worth trying to bring about systemic changes to remove the need for aid, but systemic change isn't something that we can snap our fingers and bring about. It's a complex process that carries its own costs and benefits, and the potential for systemic change doesn't remove the need to think carefully about options for improving wellbeing immediately).
In light of my more general feelings, I'm pretty strongly in favor of efforts that try and ask aid recipients what they want and value, rather than trying to make these tradeoffs based on our own moral reasoning. For that reason, I've been very pleased that GiveWell has incorporated surveys in its computation of moral weights, and I'll be very excited to see the results from HLI's survey on the neutral point. I would love to see more survey work that tries to tease out views on deprivationism vs. TRIA vs. Epicurianism among individuals actually impacted by aid. However, these might be complicated enough questions that focus groups and other more in-depth approaches would work better than surveys.
With those comments out of the way, I also wanted to ask a couple specific questions:
Hi MHR,
I also wish that these choices need not be made.
I find myself still trying to form a view on how much we can and should outsource our moral reasoning by surveying people in general and beneficiaries in particular. I think this is a tricky question, as there are many technical questions we don't and probably shouldn't survey the affected people to decide on the best course of action (i.e., setting interest rates). That being said, I would welcome more work understanding people's views on these tough philosophical questions. I think this could be a promising line of research[1].
Answering your specific comments.
But the IDinsight report on this topic (2019) made me think this type of work may be more difficult to do in very low-income settings than I might have hoped.
Thanks so much for your answer. I generally think what you're saying here makes sense, but I wanted to dig into one specific point. You say:
What worries me here is that you don't need to be a totalist to have these concerns. Even under a TRIA framework, wouldn't you still care about the population-level wellbeing impacts of any intervention (at least on the portion of the population that exists in both the world where the intervention happens and does not happen)? It feels like a little bit of a selective demand for rigor to say that this makes the total utilitarian calculus intractable, but not that it makes any of the other calculi intractable.
Still, I do recognize that total utilitarianism sometimes leads to galaxy-brained worries about higher-order effects.
Right, I should have clarified that the gnarly thing with totalism is considering the effect on all future 14k+ generations and the likelihood they exist, not just the higher-order effects on the presently existing population.
However, I'm not the philosopher, so Michael may disagree with my sketch of the situation.
Thanks HLI. I really like the post.
Pointing out an issue with the links to sheets that are referenced. Remove everything after "/edit" to make them work (as per below), and the latter one regardless is not publicly accessible:
https://docs.google.com/spreadsheets/d/1NMAU-a1X4vqjodjI6kf8KnUyCJaK9uyNvXWj5VetDZw
https://docs.google.com/spreadsheets/d/1RrBuiPVgL-t8hlr6EqkqABiaqdHMGkpvfeiqiiX49LU
---
Regarding the content, as explained in Joel's comment above the immediate expected replacement effects are not included, and if they were to be you need to ask why stop after the first generation. Is there a legitimate argument however to count the first generation and stop there? Because:
Thanks.
Thanks very much for flagging the issues with the spreadsheet links. I believe I've fixed them all now but do let me know if you encounter any further issues.
Yep that makes sense to me
Thanks for the analysis!
It is worth noting the portfolio approach corresponding to worldview diversification applies to the allocation of resources of the community as a whole, as far as I understand. So, even if one has "30% credence in deprivationism and 100% credence that the neutral point is below one", assuming AMF (or other life-saving interventions which score highly under deprivationist views) currently receives more than 30 % of resources, one could reasonably direct (at the current margin) all donations to StrongMinds (or other life-improving interventions which score highly under epicurean views).
I also wonder whether GiveWell's moral weights being majorly determined by its donors (60 %) has the intention of capturing other effects besides those directly related to the death of the person. For example, Wilde 2019 analyses the effect of bednets on fertility, concluding:
If the results are suggestive that decreasing ITNs leads to higher long-run fertility, AMF would tend to decrease longterm fertility. This would tend to decrease the future population size, but it is unclear whether this is good or bad.
I guess population size considerations did not play much of a role on the moral weight answers of GiveWell's donors. However, such considerations could play a major role in determining the longterm cost-effectiveness of life-saving interventions, so they should arguably be investigated.
It does? Says who? And why does it? Given that attempts there have been, as far as I can tell, almost nil attempts to think through the worldview diversification approach - despite it being appealed to in decision-making for many years - it strikes me as an open question about how it should be understood. I see moral uncertainty as asking a first-personal question - what should I do, given my beliefs about morality?
Ah, I too used to spend many hours wondering what GiveWell really thought about things. But now I am a man, I have put away such childish things.
Hi Michael,
Thanks for the reply!
The decision of which interventions to support depends on their marginal cost-effectiveness, which in turn depends on the amount of resources invested in the interventions globally, not just by me.
I agree the worldview diversification approach is quite ad hoc, and I much prefer the softmax approach suggested here by Jan Kulveit and Gavin Leech.
I think it is useful to understand the reasoning behind certain assumptions (e.g. giving large weight to donors' moral weights), because they may inform our own analyses. However, one should still question whether the reasoning makes sense.
We're having trouble actually finding the Peasgood et al paper. Have you/has anyone actually seen it?
It's unpublished, but I actually have access to a version of it. I would have to ask Peasgood to share with anyone.
I’m glad that it is a real thing :-). If you could get permission to share it that would be very helpful. There are several pieces of work relying on it including a handbook chapter and a UK government paper. And this is relevant for our pivotal questions on well-being measures
Skimming through this, this is great! My only bone to pick is that, skimming through this, I don't have an easy understanding of the intuition behind the key results. For example, it would be good to know (from reading the summary?) what the intuition behind the following results are:
Not sure what others think, but personally I like to understand intuitions like the above!
Hi Jack, thanks for the feedback! I think your suggested intuitions are about right for the first two points.
Regarding your third point, I'm inclined to phrase it slightly differently. People aren't generally pretty sad on a life-satisfaction view, it's more that the people AMF saves will live hard lives. That's why we're trying to help them. If we expected them to be considerably more satisfied with their lives, then I think the cost-effectiveness comparison would look very different.
Um, because these are literally the results these views are structured to give! To me, your question is akin to asking "why does consequentialism care more about consequences than deontology?" Sorry, maybe I've misunderstood.
To be clear, there is no intuition here! These are the outputs of an empirical analysis. There's absolutely no reason it has to be true that the purported best life-extending intervention is better, under a range of different philosophical assumptions, than the purported best life-improving one. In a nearby possible world, AMF* could have been very many times more cost-effective on the assumptions most generous to saving lives.
Is it not true that if AMF generally saved older people then giving to AMF would have been equally as good under TRIA as deprivationism?
If so I think it’s worth making this explicit. It’s an interesting and important point that for interventions that prolong the lives of older people, it isn’t nearly as consequential what moral theory you choose. It’s far more consequential for interventions that save young people.
I generally think intuitions like this are very useful as it allows your analysis to be applied to more scenarios than just the one at hand.
Based on this post I felt motivated to try to give a more visual and interactive explanation of the underlying philosophies and their bearing on WELLBYs. This is now available here (with an EA forum version here).
Very interesting report thanks folks! I am very sympathetic to the WELLBY approach. I wonder if anyone shares the intuition that the real improvement of subjective wellbeing doesn't follow linearly when people report on a 10 point scale. When I think about how I rate something something like how tasty a meal was, there is a bigger real difference between a 6/10 and 7/10 than between a 5/10 and a 6/10 even though the difference in my ratings was 1/10 in both cases. I wonder if something similar applies to ratings of SWB.
This could have important implications for which groups to target with certain interventions, if for example through further research we found something like: the first WELLBY point increase from the neutral point is 'worth more' than a WELLBY point increase at a higher starting point.
I'm fairly new to this area and have just engaged with it through HLI's posts so I'm not sure if this has been talked about before. Keep up the awesome work.
Hi! Thanks for engaging. Yes, the issue you raise does get discussed quite a bit, and is much worried about (by effective altruists but not in general). I've got a working paper here where I review the theory and evidence and tentatively conclude people probably do interpret the difference between each unit as having the same value (i.e. the scales are interpreted linearly).
My colleague, Casper Kaiser, who is also an HLI trustee, has a more recent paper which shows an approximately linear relationship between reports and later behaviour.
Internally at HLI we're working on doing our own survey on this stuff too!
Awesome, will check it those out.
I don't know if StrongMinds explicitly has a goal of reducing suicides, or what its predicted effect on suicide risk might be, but searching for "suicide" on the StrongMinds site (https://strongminds.org/?s=suicide) brings up a lot of results. Whether or not suicide prevention is part of their mission, treating depression would seem to potentially reduce the risk of suicide for some people . If so, some of the value of StrongMinds might come from the extension of lives. This would mean the value of StrongMinds could vary depending on which view of the harm of death we take.
Hello Rhyss. We actually hadn't considered incorporating a suicide-reducing effect of talk therapy onto our model. I think suicide rates in eg Uganda, one place where SM works, are pretty low - I gather they are pretty low in low-income countries in general.
Quick calculation. I came across these Danish numbers, which found that "After 10 years, the suicide rate for those who had therapy was 229 per 100,000 compared to 314 per 100,000 in the group that did not get the treatment." Very very naively, then, that's one life saved via averted suicide per 1,000 treated, or about $150k to save a life via therapy (vs $3-5k for AMF), so probably wouldn't make much difference. But that is just looking at suicide. We could look at the all-cause mortality effects on treating depression (mental and physical health are often comorbid, etc.).
Is there any website or spreadsheet where we can see how different ethical views affect the ranking of charities we should donate to? Specifically, where we can plug in our own parameters into the model, like we can do with the GiveWell CEA, except for more complicated positions (like the ones expressed in this post)?
If not, would such a project potentially be in the cards for HLI?
Unfortunately, no. I don't know of a website or spreadsheet that does this. I made a toy version of this just for the AMF to GiveDirectly and StrongMinds comparison, but it only includes the topics discussed in this report.
This is on HLI's wishlist of things to do, but we have a very small team, so I'm not sure when we'll get around to it. I'm personally very into this idea.
Serious question: Tanae, what else would you like to see? We've already displayed the results of the different ethical views, even if we don't provide a means of editing them
I've really enjoyed reading this topic and reading the comments here as well. I'm really excited to join the community and although I find myself vastly under-educated in the terminologies and brilliantly contrasting epistemological memes I do hope to add some Earth to the arena.
One of the most dangerous fallacies in the practical applications of social ethics and structured altruism an issue that tends to occur in the quantification of third-party experiential qualia which weeatquince, MichaelPlant, and Richard Y Chappell beautifully highlighted, and the specific point I'd like to substantiate is the sunk-cost fallacy that becomes almost a default of a happenstance when any quantification of a third-party's hypothetical experiential valued outcomes to the charted and plotted undertakings of a presupposing individual or party.
That presupposition being - that they, the individual or party that is doing the quantifying of the third-party individual's values, do actually care about that individual which their oversight and conjecture by all means is going to impact (assuming there is a actual real-world application which the hypothesis is being formulated for, whether the individual is precise or hypothetical themselves.)
Notice the extreme difference in the amount of actual consideration to all aspects and dynamics we attend to when the consideration is of a loved one in mind. With a loved one in mind whom we care about we do not leave room for any variable to arise and cause harm to them, and we are committed to the safety and well-being of them as was we can very well consider a universally human virtue, as we do take responsibility for those we love and care for.
If we look at the characters in the old tale of Cain and Abel, the projected shame denied facing by Cain is elementally psychological in the depicted scenario through the expression "Am I my brother's keeper?" - which is the very sunk-cost fallacy that is the whole of my point.
We are "our brother's keepers" when we sincerely care. We take ownership of the risks and the dangers personally and we put ourselves responsible and accountable for all possible dangers and damages that may occur to or upon another - when we love another.
That is the only valid quantifier which can be attributed scientifically procuring, as it is the only stance which allows for the continuance of accounting of all data.
A third-party stance conjecturing hypothesis does not account for all data by the very nature of it's outside-party perspective, ergo, forms of itself a sunk-cost fallacy in the terms of its limits by the dimensions it can quantify values from.
And we can see this is a default to the process in every application of it we find in history, so much so that it's been the very reason we created terms like "socially immoral" and "community guidelines" to begin with, because there is a inherent understanding that when it comes to the application of ethics coming from a policy where the authors of the policy are alien to it's subjects -there is a X-factor of unknown immoral infliction (or just as likely, a known immoral infliction) that is due to the policy makers being alien to the subjects over which they are policing.
To me this does not leave us at an impasse, the impasse we've so-far carried over this clearly defined and outlined structural flaw is the shadow of the denial we've ironically deflected ownership of, and there is a vast amount of uncharted grounds which we could invent and create off of it if we ever did commit to the admittance if these factors and the sincere actuation, and sincere application of those illuminated avenues and realities arisen from what implications we're left with.
Here's one example of use-case I can think of just off the top of my head: upon the first sign of a politician lacking care for what harm and damages their actions had caused- they should no longer be entrusted with governance of that area and criteria which they were not seen holding themselves accountable to.
That should be common sense, it should be law, and in fact I might argue that it's even a threat to national security to not have that as a deterrent to protect the innocent.
Maybe I'm wrong, and maybe I'm shortsighted even somewhere, but that was just off the top of my head and I do hope someone more knowledgeable and better educated than I am can either take this to practical application or teach me how, because I care enough to want to see it through.
No one should be entrusted with care over things they do not care about, and the verification of care is as simple as measuring the actions taken in responsibility over the care of it, not just words. Anyone can say any words. The proof is in the actual real world pudding.
The difference between a person who actually cares for the individuals of a matter and a person who doesn't care for them is as enormous the difference between a native Alaskan Eskimo being asked to map out a valley's frozen lake and a blind flat-Earther from New Mexico who's never seen snow before in his life and thinks you're talking about "hypothetical" things that only exist in his imagination but are completely non-existent to him.
And that's what it is like every time when we think our 2-dimensional conceptualizing can somehow grasp a 5-dimensional reality impact, which accounts for ongoing-time with our inarguable accountability unquestionably married to the answering-for and managing of all risks and interrelating aspects including all interpersonal impacts caused by, from, to, and with -what influences over the ultra-personal values of the lives of others we plot to tread on.
It's always hypothetical to the CEO until it's money in the bank -and then it becomes "proof of concept" for them, while it's called structural violence to us.
If you found this post helpful, please consider completing HLI's 2022 Impact Survey.
Most questions are multiple-choice and all questions are optional. It should take you around 15 minutes depending on how much you want to say.