Comments
Thanks for writing! Checking this out
Thanks for writing! Checking this out
Air filters are often proposed as a simple, scalable way to reduce the spread of respiratory infections. The underlying logic is simple - respiratory pathogens can be transmitted through the air in aerosol form, and air filters are capable of removing these particles before they are inhaled and go on to cause infection. This has led to sustained interest in air filtration as a non-pharmaceutical intervention to prevent the spread of respiratory disease.
I’ve spent a significant portion of my time at 1Day Sooner researching interventions for indoor air quality. Throughout that time, I’ve become increasingly bearish about the utility of air filters for preventing respiratory infection. I argue that, because respiratory infections are driven by short-range exposure to highly concentrated emissions and because empirical findings also fail to find a link between filters and infectious disease, air filters are unlikely to work well in a wide variety of settings and situations.
There are few published studies that examine how filters affect actual infection rates. To date, there have only been two major randomised studies assessing the effect of air filtration on actual infection incidence. Both were conducted in care homes over several months, and both reported statistically insignificant results.
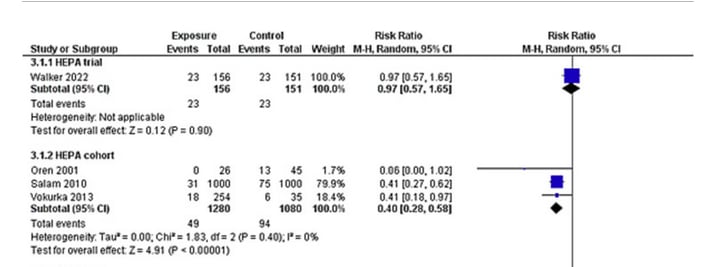
Prior to the release of these two studies, the state of the field was well summarised by a 2023 systematic review and meta-analysis. This paper summarised all of the studies that attempted to directly estimate the efficacy of air cleaning technology for infection risk, and it found a positive effect for HEPA filters.
Below is the relevant data[1] for studies that measure infection incidence. It’s notable how thin it is - data is restricted to one interventional trial (which does not find a significant effect) and three cohort studies, only the largest of which finds a significant positive effect (Salam et al, a study into aspergillosis in Singaporean hospital wards).
This meta-analysis, then, should be read with some heavy caveats. The entire finding on HEPA filters for infection rests upon one very specific scenario of a hospital-acquired fungal infection in severely immunocompromised cancer patients. It is difficult to generalize that finding to answer questions about easily transmissible viral respiratory disease passed around in everyday life.
The review also identified a high risk of publication bias, and warns that the results should be treated with caution. A final caveat to bear in mind is that other infection control measures which share the thesis of “deploy something that effectively inactivates pathogens in well-mixed air” (such as ultraviolet light) also had no effect.
Based on my reading of this systematic review, there’s a small amount of weak evidence for the effectiveness of HEPA filters, but it’s very far from definitive, nor is it particularly instructive. To me, this captures the state of affairs before large-scale studies quite well. I haven’t come across many studies that provide much important contextual or circumstantial evidence for the effectiveness of filters, which may not fit in a narrowly defined systematic review (despite months of work with a heavy focus on filters, and years of experience in indoor air quality research).
Moreover, even when studies show improved ventilation or filtration in turn improves different health outcomes (such as decreasing school absence rates), this often happens in ways that do not suggest reductions in infectious disease as the cause. One of the most influential ventilation studies in schools in California, for example, found that the longer filters had been in use, the more absences decreased. This pattern points to chronic exposure to pollutants as the cause of absences. If the cause was infectious disease, we’d expect to see a more rapid effect.
Perhaps the most convincing argument that improving steady-state air quality helps to reduce infection risk appears in Brundage et al. They studied Army trainees housed in two types of army barracks and found a significantly higher infection risk in older, leakier barracks than in newer, more tightly sealed and efficient buildings. It was a large and well-run study that involved tens of thousands of trainees over 47 months, but its central questions were far enough removed from air filters that it’s hard to take it as particularly good evidence for their effectiveness.
However, thanks to the subsequent publication of two large-scale, real-world interventional studies in 2024, we now have two studies providing good evidence specific to filters.
The first, a crossover trial conducted in three Australian care homes, found no statistically significant difference in infection incidence. However, a subgroup analysis, restricted to participants who completed the study (104 out of 135) reports a substantial effect (OR 0.53, 95% CI 0.28–1.00, p = 0.048).
The authors took 3 carehomes, each with 50-100 beds, and installed a unit with either a HEPA-14 or dummy filter in each bedroom (but not in communal areas). The participants were randomly assigned a filter or dummy (this assignment was double-blinded[2]). After 3 months, the filters were changed for dummies and vice versa (with a 1-week washout period in between to minimise carryover effects). It’s a simple study, executed well - I’m satisfied that there aren’t major holes in the methodology. That means we can subject the data to a critical eye without too much worry.
In favour of filters, it’s noteworthy that the measured positive effect is consistent over all groups/times/locations studied. No matter what data you’re looking at, there’s a similar effect size with a similar degree of statistical significance. Given this, I’d argue that dismissing the results out of hand probably undervalues them, but that’s also a challenging claim to quantitatively support. Adam Kucharski makes this point well in this post, arguing that the study was simply underpowered.
We can also dig a bit deeper into the author’s subgroup analysis. On the one hand, “people who completed the study in full” seems like a good way to generate a group of participants for whom you have comparatively more data, because, on average, they were studied for a longer period. A positive effect in this subgroup might, then, increase your confidence that this is a study that strongly suggests a real effect, but is simply not large enough to detect that difference.
On the other hand, you could just as easily make the argument that, with a study on the cusp of significance, there’s bound to be some subgroup somewhere which reaches it. Fishing for these subgroups after the fact is generally known as p-hacking - and, sure enough, there’s no mention of this analysis anywhere in the protocol agreed upon before the study.
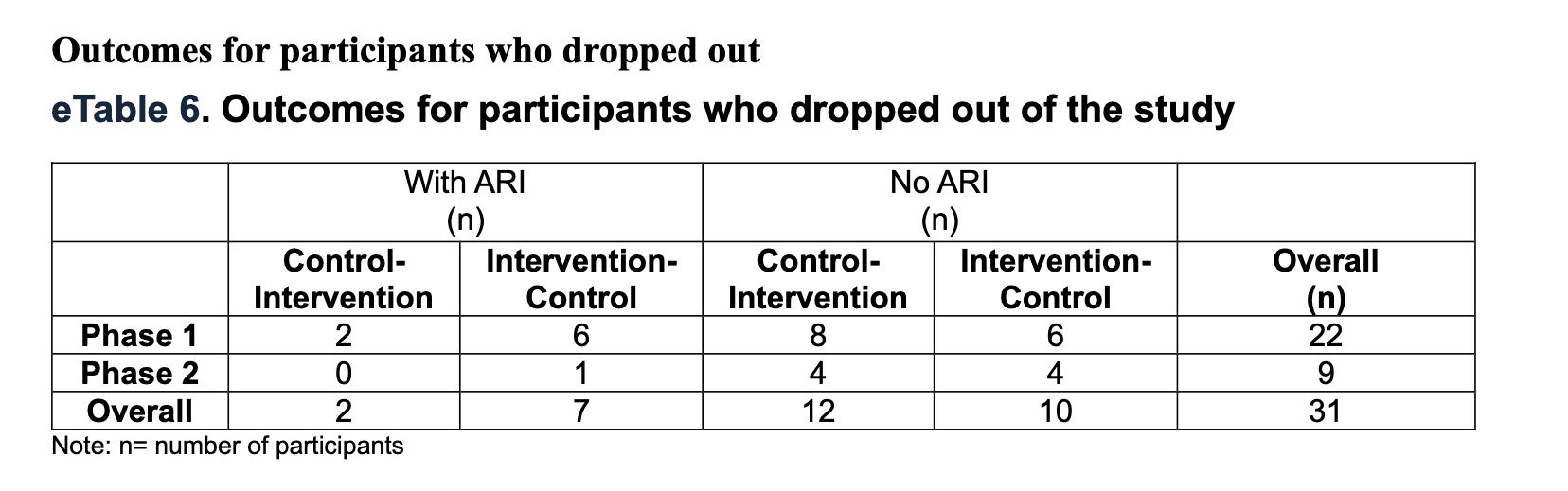
Furthermore, there are very good reasons why “people who have completed the study in full” is not a standard analytical tool. Analysis of this subgroup is considered a major sin in some circles. This is because people generally don’t drop out of studies randomly. This is particularly true in carehomes, where the usual “moved away/changed doctors/got too busy” kind of churn doesn’t occur nearly as much. In fact, overwhelmingly, people dropped out of this study because they died.
With that in mind, the table above (taken from the supplemental information files) becomes very important. It details how many people dropped out of the study, broken down by phase and by intervention status. Focusing on the left columns, we can see that during the first phase of the study, eight people who developed a respiratory infection dropped out of the study (due to death). Six of those who died were in the intervention arm.
This means that, over the entire study, a disproportionately large number of dropouts occurred in those who a) contracted respiratory infection and b) were in the intervention group. Excluding these participants therefore artificially enhances the apparent intervention effectiveness.
While the study doesn’t detail the causes of death, we obviously cannot discount the possibility that these deaths were caused by respiratory infections, or those who dropped out were systematically different in some way, making this subgroup analysis much less than persuasive to me.
The second study, conducted in British care homes was much larger than CAFACS (recording a total of 832 infection incidents, compared to 73 in CAFACS) and was conducted over a longer time period (2021 to 2024, thus including the COVID period of intense monitoring for respiratory infection), and included filters in communal areas as well as resident’s private rooms. All this means it should provide more robust evidence than CAFACS, and the results are indeed straightforward: there was no effect across any measured outcome.
Even more concerningly, unlike CAFACS, there was no indication of a consistent underlying effect masked by low power for any measured endpoint (respiratory infection incidence, rates of primary care consultation, antibiotic prescribing, hospitalisations, or staff absence).
This section is brief, as any extra analysis would simply be nitpicking for the sake of it. There are no criticisms substantial enough to dissuade me that this study represents clear-cut evidence that, in this case, filters had no effect on respiratory disease transmission.
So, in theory, why might filters fail to disrupt transmission? Experimental studies consistently show that portable HEPA filters substantially reduce airborne particle concentrations to a degree often equivalent to adding several air changes per hour. Filters definitely remove pathogens and infective aerosols from the air. This is not a fact in dispute.
However, this mechanistic evidence does not straightforwardly translate into infection reduction. The key issue is the mechanisms of pathogen transmission. In general, respiratory infections occur through close-range interactions, where individuals are exposed to high concentrations of particles over short periods of time (low double-digit numbers of seconds).
Even if particle sizes are small enough to be aerosolised for long periods, the actual exposure to these particles is still dominated by short, close-range interactions. This point often leads to confusion - even though it’s likely to be the case that most infections are caused by smaller particles (able to remain suspended for hours), that doesn’t mean that in practice actual infections don’t still rely on short-duration, close-range exposure dynamics.
By contrast, filtration primarily reduces the background concentration of airborne particles, and does so over a timescale of minutes. This means that they’re not very good at disrupting short-range transmission, which limits the extent to which they reduce the actual risk of transmission in real-world settings[3].
However, that doesn’t mean filters can’t be useful. Damon Binder demonstrates (albeit in the context of GUV) that even if long-range transmission causes a minority of overall transmission, interventions which disrupt long-range transmission can have a significant impact on overall disease rates.
I think the best argument for how filters might work involves the disruption of superspreading. Some proportion of large transmission events appear to be driven by a small number of highly infectious individuals. For instance, a COVID-19 human challenge study found that 86% of all of viable virus shed across the entire study came from just 2 of the 36 volunteers[4].
Much greater shedding from a smaller number of individuals may indeed create a high enough background concentration of pathogens that long-range transmission through steady-state air becomes more likely. There is reasonably good evidence that superspreaders are an important driver of infections for a number of different pathogens. In this context, filters are likely to be very effective.
However, this remains only a theoretical assumption, without much real-world evidence one way or the other. Apart from this, the theoretical case that filters impact respiratory disease transmission is much weaker than it might look at first glance, which helps explain the negative results seen in the real world.
The evidential landscape for air filters in infectious disease can be summarised as follows. In theory, air filters should reduce background pathogen transmission, but because respiratory diseases usually spread over short distances and in narrow timeframes, the positive effect of filters is likely modest. Filters may also help prevent superspreading events. But, while superspreading is known to play a major role in transmission, it is notoriously difficult to study in real-world settings, which makes the impact of filters hard to quantify.
Real-world evidence is essentially confined to two studies, both of which were conducted in care homes. One study found a weakly positive effect, which didn’t officially rise to statistical significance (but which should not be completely disregarded for clipping a somewhat arbitrary confidence threshold). However, the other study; larger, but, if anything, even more methodologically robust, simply found no effect at all.
Furthermore, all of these results exist in an environment of publication bias. Given that, since publication of the 2023 systematic review, at least one other high-profile study in UK schools, apparently completing in 2022, seems to have failed to report results, I’m not optimistic this problem has improved much.
None of this means filters deserve the scrapheap. More research in real-world conditions is clearly needed, and, it seems, some completed studies have yet to be reported. But it is worth being clear-eyed about what that research is likely to show. The best-case scenario appears to be that, against infections, filters are of modest use in a narrow set of situations; and it is far from unlikely they do nothing at all.
Another good way to summarise my thoughts is that if filters are highly effective in preventing respiratory infection, it’s quite weird that (even after all the pandemic-driven interest), we still do not have definitive evidence that that is the case, and even weirder that the only real-world evidence available points increasingly strongly to the opposite.
I think the attention given to air filtration is completely reasonable. They’re relatively cheap, easy to install (especially standalone units), and promise to reduce the incidence of respiratory infection. I think it’s therefore completely rational that they were widely hyped during the pandemic. With no real evidence one way or the other and a perfectly plausible hypothesis, deploying a zero-risk, low-cost intervention was a very prudent move.
However, it shouldn’t be ignored that during this period of hype, the evidence base for air filters’ ability to fight infectious disease was already very weak. Now, six years on, much serious research has ended in two multiple large-scale studies reporting no significant effect.
My overall view is therefore that the balance of probabilities have tipped towards it being unlikely that filters actually have real-world use against respiratory infection.
I’m open to hearing opposing points of view or disagreements. I’d be particularly interested in real-world studies of filters on infections that I might have missed, and it’s surely a limitation that all of the current RCT evidence takes place in carehomes, and filters may be found to be more effective in other environments.
I’m also open to opposing theoretical arguments, or evidence suggesting that filters are very useful for superspreaders. But I’d also point out that, if there is an emerging consensus that this is the most likely way in which filters will be useful, the wider discussion of both effectiveness and deployment is yet to be explicit about that..
I’m pleased that further studies with filters are currently underway, and look forward to those results - and I sincerely hope that they are positive, and that this post becomes thoroughly debunked. I hope to be wrong about filters. I think cheap, easy-to-deploy interventions that help reduce respiratory infection incidence (and probably come with some side benefits for PM2.5, dust, and hayfever) would be an excellent thing for the world to have. At present, though, I’m very skeptical that they live up to the hype.
My thanks to David Carel and Gavriel Kleinwaks for their thoughtful suggestions on this piece, Tess Lanzarotta for her numerous style improvements, and a special thanks to Josh Morrison for his consistently insightful feedback through my endless drafts of this piece.
In case you need it, a quick primer on reading meta-analysis graphs: individual studies are represented by a dot and horizontal line (the dot showing the headline results and the line showing the confidence interval), and the pooled results are represented by a black diamond. The middle line is the line of no effect. Studies falling to the left of this line show a positive effect, studies falling to the right a negative. If the line touches or crosses the line of no effect, the study is not statistically significant (the same rules apply to the overall black diamond). I’ve had to cut the scale off this graph, but you can visit the original paper to see that.
You may be wondering why double-blinding is needed here - the placebo effect might be powerful when it comes to headaches, but it’s not going to do much to influence a BioFire PCR test. I’m wondering that too! Perhaps you suppose there are some arguments one can make about likelihood for staff to administer tests, or patients to report symptoms that lead to testing, but (especially given anyone’s being tested regularly anyway), this seems like pretty thin gruel. The increasing tendency of journals, ethics committees, or reviewers to just (pardon the pun) blindly demand randomisation of any study, regardless of the circumstance, is, I rather suspect, a real irritant for lots of real-world studies. But I digress.
This argument therefore potentially applies to upper room GUV systems, too - I do not consider those in this post as they’re able to reach much higher eACH numbers than filters (which are generally agreed to cause unacceptably bad noise and draught problems beyond 5eACH, while GUV systems trivially reach double-digit eACH).
In which 36 your author is privileged to count himself a member


This matches my understanding, but I think the conclusion is too strong. That is, I would agree that in most conditions this won't materially affect transmission, but there are still reasons to think that in settings where people are properly masking, there should be a reasonably clear (or even large) effect on residual transmission. So I'll strongly agree that it's good further studies are underway, but I'm skeptical that they address the point I think i most likely to be relevant.
Does this matter in practice? Well, not when people are ignoring infection risks and can't be bothered to mask, so perhaps not - unless we see an actually worst case pandemic, in which case I expect for behaviors to change and for this to have some non-trivial impact. How much is very uncertain, but I could imagine that conditional on masking, it would decrease transmission rate by more than 10%, which matters greatly if we're talking about moving from, say, r=1.05 to r=0.95.
How likely is the case where it makes such a difference? It's unlikely, but it's exactly the class of case where making a difference matters; the infection rate is possible to reduce greatly, but not easy to actually reduce enough to stop spread using other interventions. (Also, as we saw during COVID, policy responses seem to get relaxed around r=1, and groups that want to push below that level will need something marginal to reduce transmission in their community.)
Given the above logic, clearly there are other methods we should prioritize more strongly, but I think it's premature to claim the intervention isn't going to work at all, even if we find trivially small or null impacts from newer studies. This mistake would be similar to, and related to, the mistake made during COVID, when many public health officials jumped from the observed and easy to notice fact that most transmission is via large droplets to the incorrect claim that there isn't aerosol transmission. And if we slow large droplet based transmission, i.e. if people can keep their damn masks on, the residual infections plausibly get much more important.