Introduction
Our research found that melatonin supplementation, cognitive behavioural therapy for insomnia (CBT-I), light regulation, mindfulness-based stress reduction (MBSR), and improved night-time air circulation could all be effective ways for you to increase the quality and quantity of your sleep.
This is a summary of research conducted into the most worthwhile practices for sleeping better. The post is the first in a series looking into the most effective ways people can improve their wellbeing, aiming to present this information as simply and practically as possible.
Thanks to the EA Infrastructure Fund for financing this project. If you find this information useful and/ or take up any of the suggestions, please let me know in the comments or a personal message!
Important note: None of the following constitutes professional medical advice. Some of the interventions suggested have risks of negative side effects that are discussed below. We encourage you to experiment with these practices but please be cautious in doing so and take any risks seriously.
Top takeaway
Our principal recommendations for improving sleep quality are (in order):
- Melatonin supplements: 0.3mg (300mcg) daily taken two hours before bed.
- CBT-I: a six-to-seven-week, self-guided course in cognitive behavioural therapy for insomnia, accessed through an app.
- Light therapy: greatly increasing exposure to bright light during the day, either through building a lumenator or purchasing a SAD lamp.
- Improved night-time air circulation: opening a window to reduce overnight CO2 accumulation.
- Mindfulness-based stress reduction: mindfulness training through an app with a focus on sleep.
Key Findings
Following a broad search of possible interventions, this review evaluated the effectiveness of 11 practices for improving sleep quality and quantity using an adapted weighted factor model.[1]
The five most promising interventions are listed below along with a brief explanation. More detailed assessments of all 11 practices are provided further down.
This research compared interventions across six criteria: strength of evidence, quality of evidence, ease of implementation, risk, externalities, and novelty. Full results from the model, along with reasoning for the metrics used and their respective weightings, can be found here.
Melatonin
Ranking: 1st
Intervention: 0.3mg daily supplementation (e.g. Options A, B and C)
Summary: Melatonin is a natural sleep hormone that can improve sleep quality and quantity when taken in small, daily doses. Melatonin supplementation appears highly practical, with a low risk of notable side effects as well as possible spillover benefits for other conditions.
CBT-I
Ranking: 2nd
Intervention: Completion of an app-based CBT-I course (e.g. Dozy; CBT-I Coach)
Summary: Cognitive Behavioural Therapy for Insomnia (CBT-I) involves a combination of reframing negative thoughts around sleep, improving sleep hygiene, and implementing sleep restriction. We found good evidence that completing a self-guided CBT-I course via an app can be an effective way to sleep better.
Light therapy
Ranking: 3rd
Intervention: Increasing indoor lighting brightness, preferably up to 10,000 lux or more (e.g. a ‘lumenator’ or a Seasonal Affective Disorder [SAD] lamp).
Summary: Multiple studies have found that significantly increased exposure to bright morning light improves sleep quality and quantity. We found negligible risks to this practice as well as possible benefits to mood and alertness, though this does require some time and money to set up.
Improved night-time air circulation
Ranking: 4th
Intervention: Leaving a window or internal door open while sleeping.
Summary: There is reasonable evidence to suggest that high levels of carbon dioxide can accumulate overnight in a closed room and that this reduces sleep quality. Leaving a window open overnight is a simple and effective solution with minimal downsides.
Mindfulness-Based Stress Reduction (MBSR)
Ranking: 5th
Intervention: Completing an app-based mindfulness-based stress reduction course (MBSR) (e.g. Calm; The Mindfulness App)
Summary: Mindfulness-based stress reduction courses are associated with improved total sleep time and reduced sleep disturbance. MBSR is not targeted at sleep as an intervention and likely offers significant additional benefits.
Why sleep matters
The selection effects of choosing to read this article mean that you are likely already convinced that improving your sleep is a valuable use of your time. In case that is a poor assumption, this is a very brief argument in favour of the importance of sleep.
Sleep is fundamental to wellbeing
35% of American adults are estimated to sleep less than seven hours on average. This is considered sleep deprivation, with more than seven hours of sleep a night the consensus recommendation.
Sleep deprivation is linked to a higher risk of many (perhaps most[2]) negative health conditions, including hypertension, coronary heart disease, diabetes, and obesity. It has also been directly linked to lower reported quality of life and wellbeing.
This makes sleep one of the most effective interventions for improving other aspects of wellbeing. Though health issues like those above can in themselves reduce the quality of sleep, there seems to be a range of tractable ways in which to improve sleep regardless.
Modern living is not set up for ideal sleep
Perhaps some of the practices suggested here feel to you like an excessive intervention into the natural process of sleep, something that should not require supplements or training programmes. But in the excellent words of the writer Gwern Branwen, ‘I would point out to such readers that they are already profoundly tampering with their natural sleep cycle, and indeed, all of Western civilization is tampering with it’.
People tend to go to bed more than an hour earlier each night when taken away from any artificial light through the evening. Mobile phone use in the evening is a direct act of sabotage on the quality of your sleep.
EAs are smart people and have shown significant previous interest in sleep
There are eight previous articles on improving sleep on the Forum[3], as well as multiple high-quality posts on EA-related websites[4]. Taking the premise that effective altruists are generally smart people, the prevalent interest in sleep among the EA community suggests it is a smart decision to take sleep seriously.
Common (sense) interventions
The focus of this research is to explore the effectiveness of practices that are likely to be new to the majority of readers. Given this, we have omitted the exploration of a few common suggestions for improving sleep that are nevertheless worthy of some mention:
- Use earplugs or a white noise machine if you frequently notice ambient noise when trying to fall asleep.
- Install blackout blinds or wear an eye mask if you are often woken up early by ambient light.
- Choose a realistic time to get up each day and stick to it as much as possible. Trying to catch up on sleep over the weekends is ineffective and can be counter-productive in disrupting your circadian rhythm.
- Minimise the use of your bed for anything that isn’t sleeping.
Discussion of Primary Recommendations
Melatonin
Intervention: 0.3mg daily supplementation
Score: 5.95/10 (1st)
Melatonin is a hormone that triggers sleepiness and works to regulate sleep cycles. A small dose of melatonin taken daily (0.3mg, or 300mcg) produced a 4.8% increase in total sleep time (time spent in bed) and a 12.8% increase in sleep efficiency (the % of time spent actually asleep out of the time spent in bed) in this study.
Most commercial melatonin supplements come in significantly larger doses - often 3, 5 or even 10mg. While these doses also appear reasonably effective, there is a greater risk of negative side effects from regularly taking melatonin in these larger quantities.
These side effects are mostly mild (headaches, dizziness, or drowsiness the next day) but can be more significant (nausea, diarrhoea, or worsened depression). It is also worth being cautious about taking melatonin if you already take regular medication.
There is some evidence to suggest that melatonin supplementation can reduce blood pressure. It has also been linked with an improvement in symptoms for people with certain chronic health conditions, including cancer and endometriosis. However, it seems plausible that these improvements are a result of improved sleep rather than any additional effects of melatonin.
Once you’ve found a supplier of melatonin at the right dosage, this is a highly practical intervention. A year’s supply of melatonin should not cost more than $30 or so. Taking a capsule each night in the hour before bed requires little time or motivation.
CBT-I (Cognitive Behavioural Therapy for Insomnia)
Intervention: Completing a self-guided CBT-I course
Score: 5.78/10 (2nd)
CBT-I is a version of cognitive behavioural therapy specifically tailored for insomnia. Principally, it involves strict sleep hygiene coupled with sleep restriction, concepts that are nicely explained here. Previous research has found that CBT-I provided via individual or group therapy sessions can be more effective than prescription medication at treating insomnia, while also having far fewer notable side effects.
Though CBT-I is targeted at insomnia, the key principles of sleep restriction and strict sleep hygiene seem an improvement on common sleep behaviours. This makes CBT-I valuable to most people as a set of tools for improving sleep.
Our recommendation is based on the use of a CBT-I app, enabling access to the benefits of CBT-I without the cost or difficulty of finding a specialist practitioner. We found good evidence to suggest that six to seven weeks spent following an app-based CBT-I course produces significant improvements to sleep quality and quantity.
The best CBT-I apps currently available appear to be either Dozy, an EA-aligned CBT-I app available via beta testing, or CBT-I Coach, a partnership between the US Department of Veteran Affairs and the Stanford School of Medicine. As an alternative to using an app, Overcoming Insomnia is a CBT-I workbook produced by leading sleep medicine researcher, Colin Espie.
Light therapy
Intervention: Completing a self-guided CBT-I course
Score: 5.63/10 (3rd)
There is a significant range of research suggesting the benefits of increasing daytime and minimising night-time exposure to bright light. Most people working indoor jobs are exposed to only a small amount of bright light throughout the day. Bright light treatment generally aims for exposure to 10,000 lux, the equivalent of the light exposure outside on a day with light cloud, for two hours or more.
One study found that the average time spent in light over 1,000 lux (10 times less than the recommended level of ‘bright’ light) was 23% in ‘modern’ conditions vs. 71% in ‘natural’ outdoor living conditions. It seems reasonable to conclude that most people are now experiencing far less bright light than was normal for most of human history.
Exposure to bright morning light can reset the circadian rhythm. This in turn can reduce the time taken to fall asleep and minimise sleep disturbances through the night. The effects on total sleep time and sleep efficiency were generally moderate but consistently positive in the studies reviewed, with some studies showing improvements of more than 15% for patients with significant sleep issues.
Achieving exposure to 10,000 lux requires a moderate investment of time and money, but once a solution is found it can provide permanent benefit.
The simplest method is to purchase a SAD lamp that emits 10,000 lux and place this on your desk, maximising exposure while working. However, the light levels received from a SAD lamp can decrease significantly if placed too far from the face, while the lamp’s light offers minimal benefit when doing non-desk based activities.
The alternative is to install sufficient lighting in a room that the whole space is lit to 10,000 lux or more. This tends to involve buying 10-25 very bright lightbulbs which in combination produce the required brightness. Ben Kuhn and Eliezer Yudkowsky have each written good, practical guides for doing this.
Improved night-time air circulation
Intervention: Leaving a window or internal door open while sleeping
Score: 5.31/10 (4th)
Opening a window overnight can reduce CO2 levels in a bedroom by 60%. There is reasonable evidence to suggest that abnormally high levels of carbon dioxide cause significant decreases in sleep quality and cognitive performance the next day. Direct studies on the impact of improved air circulation by opening a window or internal door overnight are limited but suggestive of improvements in sleep quality.
Given the simplicity of leaving a window or door open, this intervention seems highly worthwhile. While an open window could make for a cold room, this too could be beneficial for sleep quality. An overly cold room also seems simple enough to fix with warmer bedding.
On top of this, improved overnight air circulation could plausibly reduce the accumulation of household air pollution, providing additional benefits to health and wellbeing.
Mindfulness (MBSR)
Intervention: Completing a self-guided MBSR programme
Score: 5.10/10 (5th)
Mindfulness-based stress reduction combines practising mindfulness meditation, non-judgmental awareness, and exploration of the feelings and sensations associated with stressful events. A six-week MBSR course produced a 37% improvement in Pittsburgh Sleep Quality Index scores, an aggregated measure of sleep quality and quantity. While app-based therapy appears less effective than this, it is still likely of significant benefit. Specific research into the effects of app-based MBSR on sleep is limited, but this randomised control trial found a significant decrease in sleep disturbance for users of the meditation app Calm.
Given that this and other research has found significant benefits from mindfulness training for numerous aspects of wellbeing, MBSR appears a valuable intervention. In some cases, mindfulness training can make individuals more aware of negative behaviours and thought processes without providing relief, though this appears to be an uncommon outcome.
Apps tailored to improving sleep do not appear common. Two suggestions based on a limited review of available solutions are Calm and The Mindfulness App.
Secondary Recommendations
The following is a summary of the other interventions explored in-depth that did not score as high in our assessment.
Mattresses
Intervention: Changing to a medium-firm mattress
Score: 5.05/10 (6th)
Replacing current bedding with a new, medium-firm mattress appears to produce a 5-6% improvement in sleep quality and efficiency. While individual preferences may differ, the majority of studies that we analysed concluded that a medium-firm mattress was the optimal type for maximising sleep quality.
Mattresses, however, are a significant investment that may not be practical or worthwhile for many given the only moderate improvement in sleep quality. Additionally, studies tended to test subjects who were previously sleeping on mattresses several years old. Given this, we can reasonably expect a diminished effect for people with more recently purchased bedding.
We make no attempt to recommend specific mattresses given the large differences in price and larger amounts of marketing involved in their sale.
Caffeine
Intervention: Eliminating caffeine consumption from the late afternoon onwards
Score: 4.95/10 (7th)
Caffeine is a commonly known and consumed stimulant. That caffeine can make it more difficult to fall asleep is fairly obvious. However, regularly high consumption of caffeine can also have a significant impact on sleep quality.
The impact of caffeine on sleep can be avoided by limiting consumption to the first half of the day. Individuals’ speed of processing caffeine varies significantly but it is common for it to still have notable effects up to 10 hours after consumption.
At a minimum, avoiding caffeine consumption within the six hours prior to sleeping seems an easy and valuable intervention. Adjusting the results of this study to the caffeine content of a standard double-shot coffee, we estimate a 3% reduction in sleep time and sleep quality from drinking a coffee six hours in advance of sleep.
Though caffeine consumption has a significant effect and strong evidence base, we expect that avoiding caffeine later in the day is largely common knowledge. Given this, people who currently drink coffee in the evening are likely doing so for benefits that they weigh higher than a small increase in sleep quality (such as increased alertness for evening work), making this a less valuable recommendation.
Magnesium
Intervention: Taking a 300mg magnesium supplement daily
Score: 4.76/10 (8th)
Around half of Americans likely consume less than the recommended levels of magnesium, while some studies have suggested that recommended levels are significantly lower than the optimum daily magnesium intake.
While the quality of evidence is low, with no known method of causation, magnesium supplementation is associated with improved sleep efficiency and total sleep time.
Most multivitamins only contain a modest amount of magnesium[5] so we recommend taking a specific, 300-375mg magnesium supplement to test for any noticeable benefit to your sleep. However, magnesium supplementation can have significant side effects, particularly for people taking other medication, so it is important to note possible issues and stop taking supplementary magnesium should these occur.
Cold lighting
Intervention: Installing blue-enriched lighting to your workspace
Score: 4.53/10 (9th)
While lighting can come in a wide range of brightness, it also ranges widely in colour temperature. Blue-enriched (cold) lighting can improve daytime alertness and bring a modest benefit to sleep quality but is difficult to find commercially.
In our brief search, we found these household lights at 6,000K as the coolest option available. However, the blue-enriched lights used in the study referenced above were 17,000K, meaning that the benefits of commercially available cold lighting are likely to be significantly lower than those produced in research.
Given the greater evidence base and strength of effect for increasing the brightness of household lighting, we feel that this is a more worthwhile intervention than installing colder lighting.
Morning exercise
Intervention: Shifting exercise from evening to morning
Score: 4.43/10 (10th)
The positive effect of regular exercise on sleep quality is well-known. However, the timing of exercise during the day could play a significant mediating role in increasing or decreasing the beneficial effects of exercise on sleep.
For people accustomed to exercising in the evening, shifting their practice to the morning could increase sleep quality while reducing sleep disturbance and the time taken to fall asleep. However, these effects were relatively modest in the research we found and evidence on the topic is thin.
With the constraints of coordinating work, family, and social schedules, we expect that shifting exercise time will be relatively difficult for many people. Feasibly, it could even result in reduced sleep hours if you start waking up earlier to fit in exercise in the morning.
Houseplants
(Note: see this comment for why the estimate given below is likely a significant overestimate of the potential effect of houseplants on bedroom CO2)
Intervention: Buying multiple succulent houseplants for your bedroom
Score: 3.94/10 (11th)
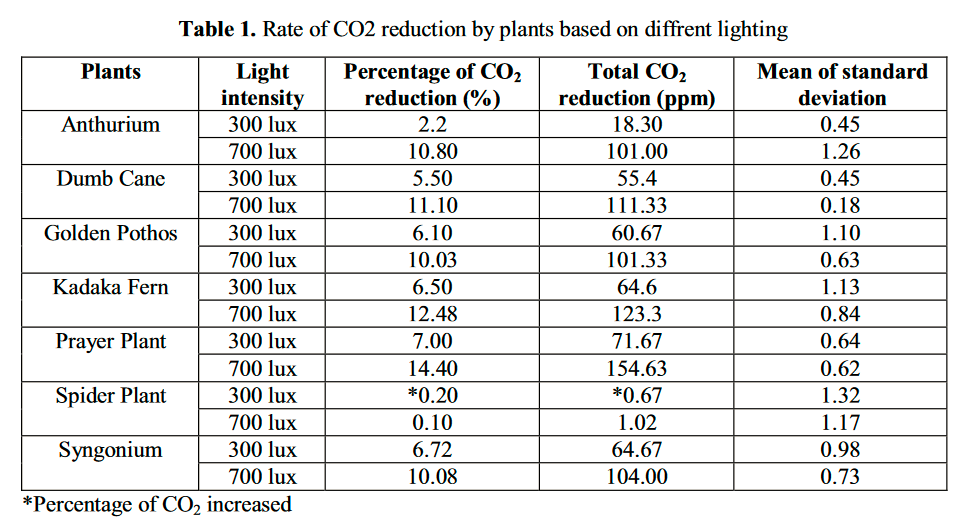
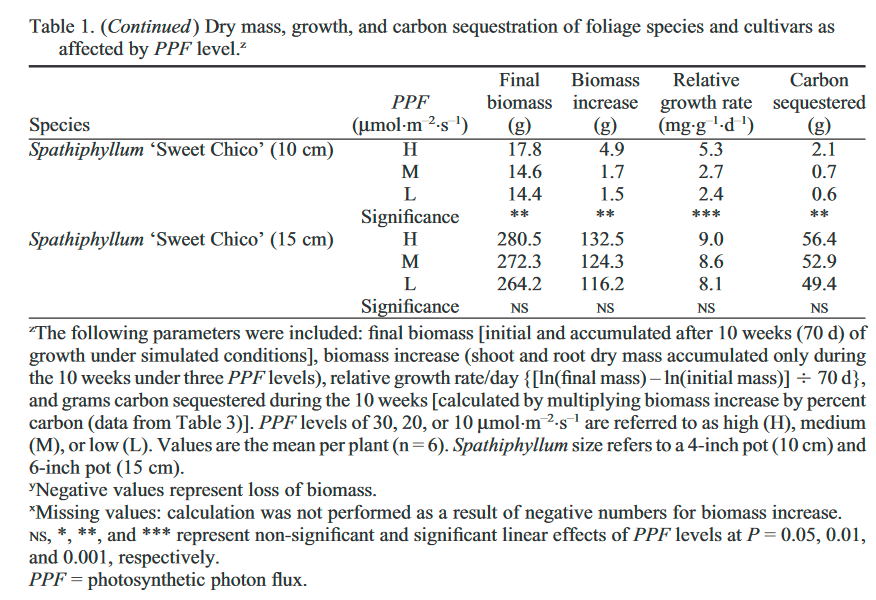
As an alternative to opening a window, there is some evidence that some houseplants can produce a notable reduction in CO2 levels in a room. In particular, certain plants that store CO2 at night to then use for photosynthesis during the day (a process known as crassulacean acid metabolism [CAM]) appear particularly effective at reducing night-time CO2 levels.
While there has been little research into this area, one study found several common houseplants reduced CO2 concentration in a room by 15-20%. It seems reasonable to assume that placing several houseplants in a room would significantly increase this effect, though likely with diminishing returns.
A study conducted by NASA into the effectiveness of houseplants at removing a range of air pollutants (to then use them on the ISS) found that Variegated Snake Plants and English Ivy were particularly promising.
We leave the decision of whether to create a small indoor forest in your bedroom in your hands but note that this is unlikely to be more effective at reducing CO2 concentration than simply opening a window.
Summary
This research forms an attempt to find the most effective ways an individual can improve their sleep, with a focus on suggestions that readers are less likely to have previous knowledge of. The methods used are rough and a work in progress, forming the basis of a larger project researching the most effective ways people can improve their wellbeing.
Our principal recommendations for improving sleep quality are (in order):
- Melatonin supplements: 0.3mg (300mcg) daily taken two hours before bed.
- CBT-I: a six-to-seven-week, self-guided course in cognitive behavioural therapy for insomnia, accessed through an app.
- Light therapy: greatly increasing exposure to bright light during the day, either through building a lumenator or purchasing a SAD lamp.
- Improved night-time air circulation: opening a window to reduce overnight CO2 accumulation.
- Mindfulness-based stress reduction: mindfulness training through an app with a focus on sleep.
Thank you to everyone who has previously written about improving sleep here on the Forum[3:1] and on other EA-aligned sites.[4:1] We hope that this research has been useful and that you’ll consider experimenting with our recommendations!
Note: We are currently running a 5-minute survey evaluating our work which we'd greatly appreciate you filling out!
The model used for this research is a rough one, loosely based on the weighted factor models used by the Charity Entrepreneurship team. A model like this allows for the inclusion of a wider range of subjective and objective measures, combining practical aspects of an intervention with evidence of its effectiveness. Results should not be taken as definitive, acting instead as a guide for updating knowledge in a positive or negative direction. As the wider project grows, this model will likely be further developed. The results posted here will be updated accordingly. ↩︎
We were going to establish the accuracy of this claim but decided it would be more worthwhile to get some extra sleep instead [it was]. ↩︎
Thank you to everyone who has previously written about sleep on the Forum. The following is a (hopefully!) comprehensive directory of previous articles on the topic published on the Forum (in order of karma): Burnout – what it is and how to treat it: Sleep [Elizabeth]; Insomnia with an EA lens: Bigger than malaria? [samstowers]; Insomnia: A promising cure [Halstead]; On Sleep Procrastination: Going to Bed at a Reasonable Hour [emily.fan]; Things I recommend you buy and use: Health/ Sleep [BenSchifman] Should we consider the sleep loss epidemic an urgent global issue? [orenmn]; Instructions on potential insomnia cure [Halstead]. ↩︎ ↩︎
Other great EA-adjacent articles: How to improve your sleep [Lynette Bye]; Behavioural treatments for insomnia [Luke Muehlhauser]; Melatonin: Much more than you wanted to know [Scott Alexander] ↩︎ ↩︎ ↩︎
Magnesium content in the first 5 multivitamins I found through a quick Google search: Vitabiotics Wellman Max [60mg]; Holland & Barrett Ultra Man Multivitamin 30 Caplets [125mg]; Boots A-Z 180 Tablets [60mg]; Centrum Advance 50+ [100mg]; Vitabiotics Wellwoman Max [100mg]. ↩︎


While I am as much a fan of wellbeing research as the next fellow - indeed, probably a much bigger fan - I have to say I found the methodology and conclusions of this research rather confusing.
If I were approaching this topic, I would have (1) done a review of the existing literature to find out what people thought was effective and what the possible interventions were, then (2) tried to assess the options in terms of (a) a comparable metric of effectiveness and (b) cost, so readers could think about what would do the most for them at the least effort.
As it is, this research seems to have missed out many of the standard pieces of advice like avoiding alcohol, napping after 3pm, having a large meal before bed, or having a sleep routine. The author doesn't mention having looked at the existing literature, but does note that other EAs have mentioned sleep. I don't mean to single out the OP, but I do want to deride the myopic and self-referential tendency among effective altruists in general to overlook work done outside effective altruism. Lots of good has happened 'out there' and we ignore it at our peril.
What I found least satisfying about this research was how this (partial list of) interventions were assessed. As far as I can see, the 'weighted-factor model' involved assigning unexplained subjective numbers to various seemingly-arbitrarily chosen properties, then assigning a seemingly-arbitrary weight to each factor to aggregate them. * I am reminded of "Garbage-In-Garbage-Out" concept in computer science where nonsense inputs products nonsense outputs. As a reader, I have no idea how to interpret the rankings or numbers - what does it mean that melatonin gets "5.95/10" or that CBT-I gets "5.78"? - or how much to update off them. The results are basically uninterpretable.
I would strongly recommend that the OP heavily revise their methods and the presentation of their research for any further work. The main thing would be to present the results of the interventions in a standardised metric, e.g. total sleep time, or standard deviations of something, so readers can make a comparison themselves, then make comments on cost and, if necessary research quality. I am happy to provide advice if that's helpeful.
*I recognise the weighted-factor model is something Charity Entrepreneurship use. I have raised it with them several times that, for the reasons given, I find this approach hard to follow or justify and thus questionably useful.
Thank you for the feedback!
There's a few points you make that I feel are important to clarify but I want to first acknowledge that the format and presentation of the research is a work in progress and could definitely be improved. In particular, I can agree that the "5.95/10" numbers aren't particularly useful given the lack of any context/ scale.
To respond quickly to a few specific points:
1) This research was overwhelmingly based on the existing literature. I chose not to include a reference list or in-text citations to maximise the readability of the text but perhaps this was an error.
2) The interventions' strength of effect, which accounts for about 40% of the score, is an average of improvements in sleep efficiency and total sleep time found in the literature I reviewed. In hindsight, I think it could have been better to highlight these findings on their own in the text and may add them in.
3) The focus of this research was to explore interventions that the reader is less likely to have heard of previously. I assumed that ideas like avoiding alcohol and late naps are things that nearly all readers would already know. On that basis, I felt that highlighting them in an article like this is unlikely to produce any change in behaviour, though I can see now the potential usefulness of presenting the size of effect.
4) I think an article like this recommending low-cost, personal interventions can reasonably have a different approach and level of rigour to one recommending charitable interventions and/or shifting large sums of money. A weighted factor model may not be the best way to frame this research but I think additional considerations like the potential risks and additional benefits of a recommendation are important and necessary to highlight.
These points make me realise that a more explicit description of the methods used and the literature reviewed would be valuable for future posts, rather than linking to them in out-of-text docs or leaving them out for a marginal improvement to the conciseness of the text.
This is the first post intended in a series and I expect to revise and improve the methods involved with each post and certainly the feedback I get on posts helps to direct that process. As a first attempt, some of the process was not as rigorous as it could or perhaps should be. In part, this is a relatively time-limited project for now (~3 months) so I am sacrificing some potential added depth in each post for the ability to cover more topics.
On a final note, I have immense respect and appreciation for the work of HLI and so really appreciate the feedback from someone who does wellbeing research at a much higher level!
Hello Ben!
Good to know this was based on existing literature. In most cases, it helps to show the reader you know that literature, to outline what it is, and then go on say what your new contribution is. Like I say, you missed a few of the obvious things, which is unfortunate. A piece of "what works for X" should, I say, include the things that work for X, then perhaps go on to flag which of these are likely to be a surprise, rather than assuming on the reader's behalf what they will already know. If you are going to have a piece on "what works for X that might but that might surprise you" you should at least clearly flag that, and then point to something such as "standard guidance on X".
Re strength of interventions being "40%" that still seems a confused way of presenting the information. 40% of what? Of a maximum score? A maximum score of what? Of cost-effectiveness? Well, why not just present the effectiveness numbers and divide them by the costs then?
I agree that this sort of thing can have a lower level of rigour but I stand by my concern that the method you use is so puzzling it's questionably useful at all. You gathered quite a bit of relevant info, but I think you presented it in a less-than-ideal way. Here, simpler would have been better: I'd have preferred a post that just said "here's a list of evidence-based ways to improve sleep" and then listed them and provided a brief discussion on each. That seems the way to go unless you have the data and time to do a quantitative (cost-)effectiveness analysis.
Glad you think we (at HLI) do good work. Like I see, feel free to reach out if you want to chat about research methods etc.! You can get me at [email protected]