WHO estimates between 81,000-138,000 die every year from venomous snakebites. What on earth!? When I first heard this I refused to believe it. How had I managed to call myself an EA for so many years and not known snakebites were this big a deal? Not only do snakebites kill an unfathomable number of people, another four hundred thousand are permanently disabled every year.
In this post I will:
- Provide an overview of the situation.
- Look at the cost-effectiveness of conventional interventions to prevent and treat envenoming.
- Argue that a new medical invention could make a massive difference and shill for the company that invented it.
Why do snakebites kill and maim so many?
Imagine you're a farmer working in the amazon. One day, as you are working your field, you suddenly feel a searing pain from your leg. You see a snake dislodging its fangs from your calf and quickly slither away. Was it venomous or not? Even if it were a venomous snake that bit you, there's a 50% chance it was a dry-bite, and that the swelling will go away after a while. The trip to the nearest medical facility will take an entire day and cost you a fortune. You decide to wait and see. After a while the symptoms get worse and you decide to consult your family. They tell you to go to the town's spiritual healer, who can treat you for a much smaller cost. When morning comes around, you finally make the decision to go to the hospital. It's now too late. By the time you arrive the venom will have done its damage. Even if you receive the correct antivenom treatment and survive, you will suffer permanent disability and be in for a long and expensive hospital stay. After a few weeks spent recovering in the hospital you will find yourself handicapped, out of work, and in debt.
Snakebite envenoming is an enormous burden on tropical regions in the third and second world. Like other neglected tropical diseases, the burden of snakebites is much larger than the just deaths they cause. Having a productive member of one's family or community suddenly die or become permanently disabled wrecks havoc on all those who were dependent on them. Children, for example, are often removed from schools to make up for the lost income and additional person who must now be taken care of.
After reading up on various studies, WHO reports, and meeting with the CEO of a venom diagnostics startup, I believe there are two primary reasons why snakebites do so much harm.
Snakebites are expensive to treat
Treating envenoming requires administering antivenom which is expensive to produce. Each type of venomous snake species requires its own antivenom. Administering the wrong antivenom is costly and harms the patient.
The hospitalization and antivenom treatment is far too expensive for many to afford. In Bangladesh, nearly 75% of snakebite victims spent their savings on treatment and over 60% had to borrow to meet the costs.
The world currently produces roughly half the antivenom needed to treat every patient. WHO argues (without using these exact terms) that there is a lemons-market for antivenom, where production of low-grade and ineffective antivenom is crowding out high-quality producers. This has reduced the profitability of antivenom production and prevents producers from scaling up production. For example, FAV Afrique, a dependable and widely distributed antivenom in sub-saharan Africa, was discontinued in 2016. I haven't been able to verify that recent discontinuations of antivenom production can be attributed to a lemon market, and an alternative explanation could be that WHO is neglecting that a worse treatment for less money may be the better outcome for some.
Lemons-market or not, we need to produce much more antivenom at a much lower cost.
Snakebites are difficult to diagnose
Diagnosing snakebites in the third world involves waiting for the patient to show symptoms and having a well-educated doctor attempt to determine the species of snakebite based on the patient's symptoms, bite-marks and geography. This process has many points of failure and misdiagnosis is common. The waiting time for the patient to develop symptoms alone delays the treatment by vital hours and lowers the chance of a complete recovery.
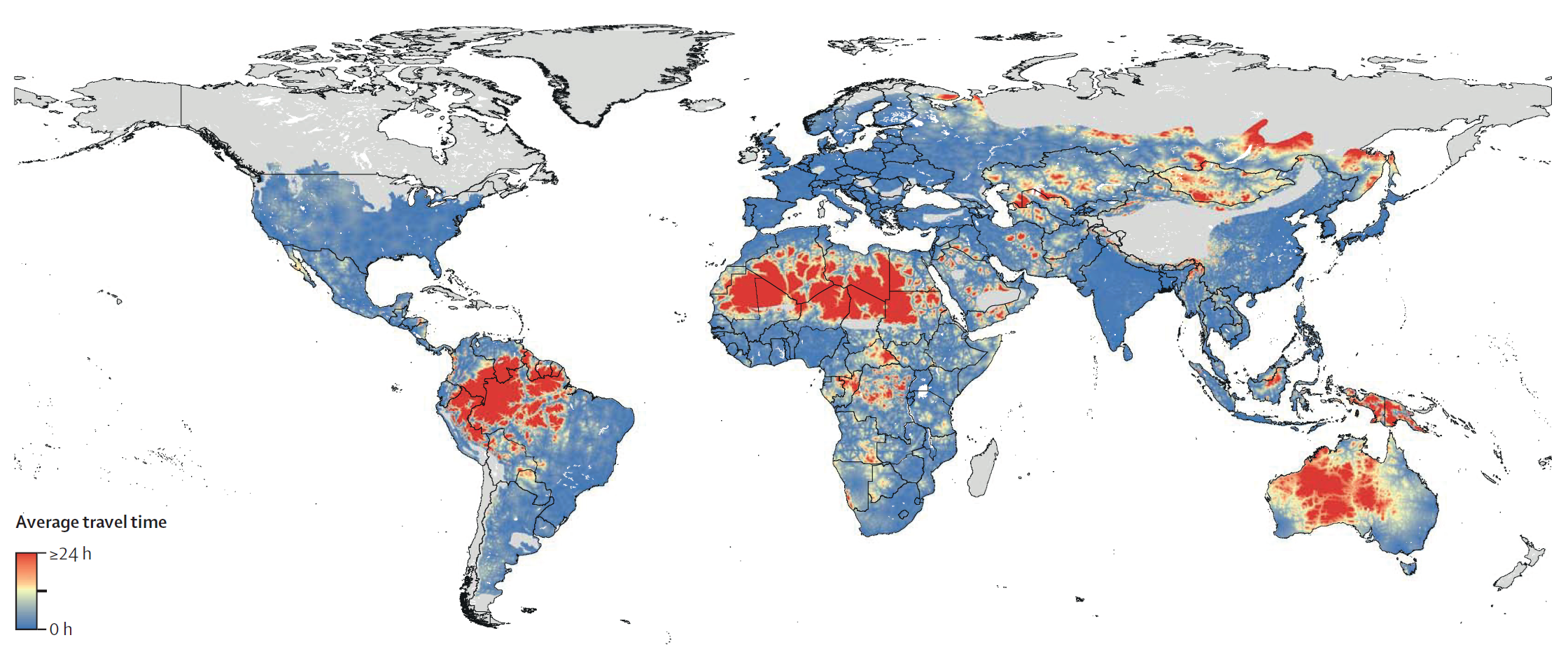
Due to the difficulty of diagnosing and cost of misdiagnosis, antivenom is often only available at larger clinics where doctors are trained to diagnose and administer it. For patients this means having to travel great distances to get treatment, by which the odds of survival have decreased.
I found this paper to be a great overview of the diagnostics landscape around the world.
Effectiveness of conventional interventions
Effectively treating snakebite simply requires healthcare capabilities much beyond what many third world countries can provide. Improving these healthcare capabilities often requires multiple steps to be taken at simultaneously which is exceptionally difficult to do.
Doctors of local clinics must become better able to diagnose snakebites to justify administering antivenom. Local clinics can't justify improving their diagnosing of snakebites if they don't have the antivenom to treat their patients. Solving one bottleneck often gives rise to another.
For reasons I don't quite understand, RCT's and other studies on snakebites are exceptionally difficult to conduct, meaning there is large uncertainty surrounding basically everything related to snakebites. This difficulty in conducting studies is emphasized by multiple reports and everyone I spoke with on the matter.
Despite this uncertainty, there are studies on the cost-effectiveness of available treatments that suggest conventional treatments may reach effectiveness in the same order of magnitude as givewell's recommended charities.
Cost-effectiveness of antivenom treatments
The most straight-forward treatment is simply to pay for antivenom and its distribution.
This was the best study I found on estimating the cost-effectiveness of antivenom treatments. The authors create a decision-tree of snakebite outcomes and run monte-carlo simulations to estimate the cost-effectiveness of treatments.
They found the cost to be $1997.91 per death averted in the most effective sub-saharan country, to $6204.95 in the least. That is $82.63-256.61 per DALY. For reference, Givewell's recommended deworming programmes are in the range of $30-80 per DALY.
The study has its limitations, with many uncertain estimates of important variables. But until better studies and RCT's for antivenom treatments are made, this study is likely the best estimate of cost-effectiveness available.
Snakebite awareness radio outreach
In many communities 60-80% of snakebite victims choose traditional medicine or spiritual healers instead of hospital treatment. People likely do this due to a mix of cultural pressures and lack of information. Radio-based outreach campaigns for other topics can be highly effective. It may be that information related to prevention and treatment of snakebites can achieve similarly effective results.
WHO emphasizes the importance of community engagement in their 2030 to reduce deaths. I would be excited to see someone do further work in analysing why radio-based outreach is so effective for certain domains and whether we should expect snakebites to be one of those domains.
A new innovation in venom diagnostics could be a game changer
After recovering from my initial shock, I discovered that one of the world's leading labs working with envenoming is located in Denmark where I live. I met with one of its researchers, who recently founded the company Venomaid. They have developed a cheap lateral-flow test that reliably detects envenoming even before symptoms appear.
This test enables anyone to reliably diagnose the species of snakebite. Such a test would enable rural medical personnel to accurately diagnose and administer the correct antivenom.
This seemed too good to be true. If diagnostics is this big a bottleneck and the test is as cheap and reliable as venomaid claims, why hasn't WHO, for example, adopted it into their 2030 plan which heavily emphasized improving clinics diagnostics capabilities? WHO's plan was launched in 2019, and has been in the works well before that. Venomaid's lab produced the world's first working lateral-flow test to detect envenoming in 2018. WHO's strategy doesn't include anything like this as a crucial component, because they didn't know it could be done.
There's many reasons to have reservations over whether it will be cost-effective. Even if the test is inexpensive, what is the cost of distribution? How much training do clinics need to administer the test? To what extent will the test alleviate the diagnostic bottleneck that is supposedly preventing roll-out of antivenom to local clinics?
I initially held many of these reservations (and still have many!), but felt I was receiving satisfying answers to most of them. For example, the entire world has just received a crash-course in producing, distributing, and using lateral-flow tests due to covid, significantly lowering many costs associated with Venomaid's test.
Venomaid's own cost-effectiveness estimate (which they claim is conservatively calculated, but seems optimistic to me) is ~20 USD/DALY for Brazil, the first country in which they plan to roll out their product.
Despite the uncertainties I believe their lateral-flow test looks both incredibly promising and neglected in its current stage. I am willing to bet money at good odds that lateral-flow tests to diagnose snakebites will be commonplace within a few decades.
They are hoping to raise $2M for their next seed round following their pilot project in Brazil, but it seems to me that if concerns over profitability and funding were less of a concern they would be able to scale much faster. If a philanthropist were to offer a large buy-order conditional on a study estimating its cost-effectiveness or something similar, they would be able to scale up and start saving lives much faster.
I hope this post will inspire some organisation to look further into this and figure out if it really is as promising as it looks to me.




{kind=link}
For reference malaria killed 600.000 in 2020 according to WHO, so it is pretty surprising to me that I've never heard of snakebites given that they kill about 1/6th of what malaria does (not to mention the handicapping).
Super interesting writeup, I'm glad that my horizon is now a little wider.
Wider list if anyone's curious what's after mosquitos and snakes:
https://en.wikipedia.org/wiki/List_of_deadliest_animals_to_humans