Comments
I'd just like to say that I had OCD/GAD for ~ 10 years but now have no symptoms due to lifestyle changes and therapy. If anyone would like to chat with me about this I'm very happy to chat [email protected]
I'd just like to say that I had OCD/GAD for ~ 10 years but now have no symptoms due to lifestyle changes and therapy. If anyone would like to chat with me about this I'm very happy to chat [email protected]
if a third party ran the survey, the results would be similar? Did you take any measures to prevent a “an EA org is running this so I have to adjust my answers accordingly” bias?


The 2023 EA Mental Health & Productivity Survey was designed to build upon the results of the 2018 and 2021 EA Mental Health Surveys, which measured the prevalence and effects of mental health problems within the Effective Altruism (EA) community and obtains more information about the experiences of community members who struggle with mental health problems, respectively. Its goal is to provide more insight into community members’ mental health and productivity issues and experiences, and to get a better idea of what resources and services people might find helpful when dealing with or for preventing these. This survey was intended for anyone wishing to improve or maintain good mental health and / or productivity, and therefore was not restricted to only those members of the community who are struggling with mental health.
This results post starts out with the demographics of the survey participants, and then covers the following topics:
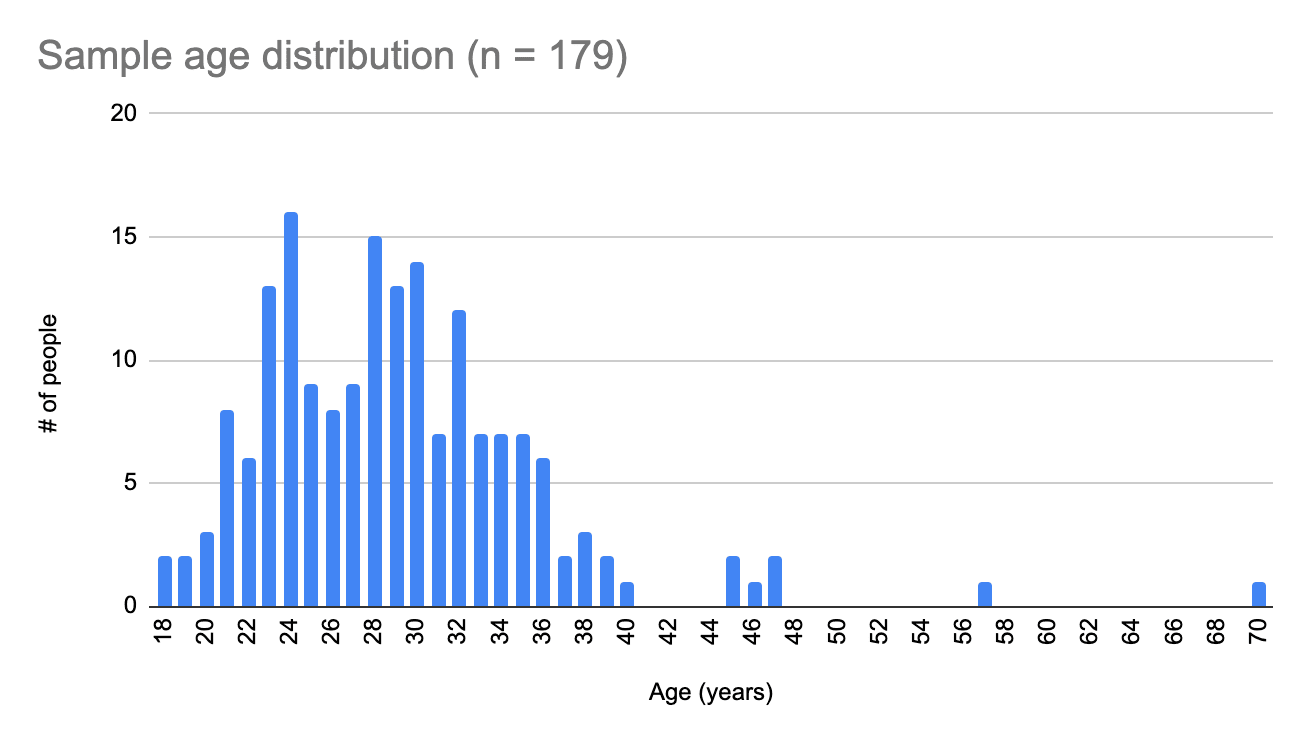
Ages of survey participants ranged between 18 and 70 (x̄=29.1, SD=6.8), with the majority of people in either their early to mid-twenties or late twenties and early thirties.
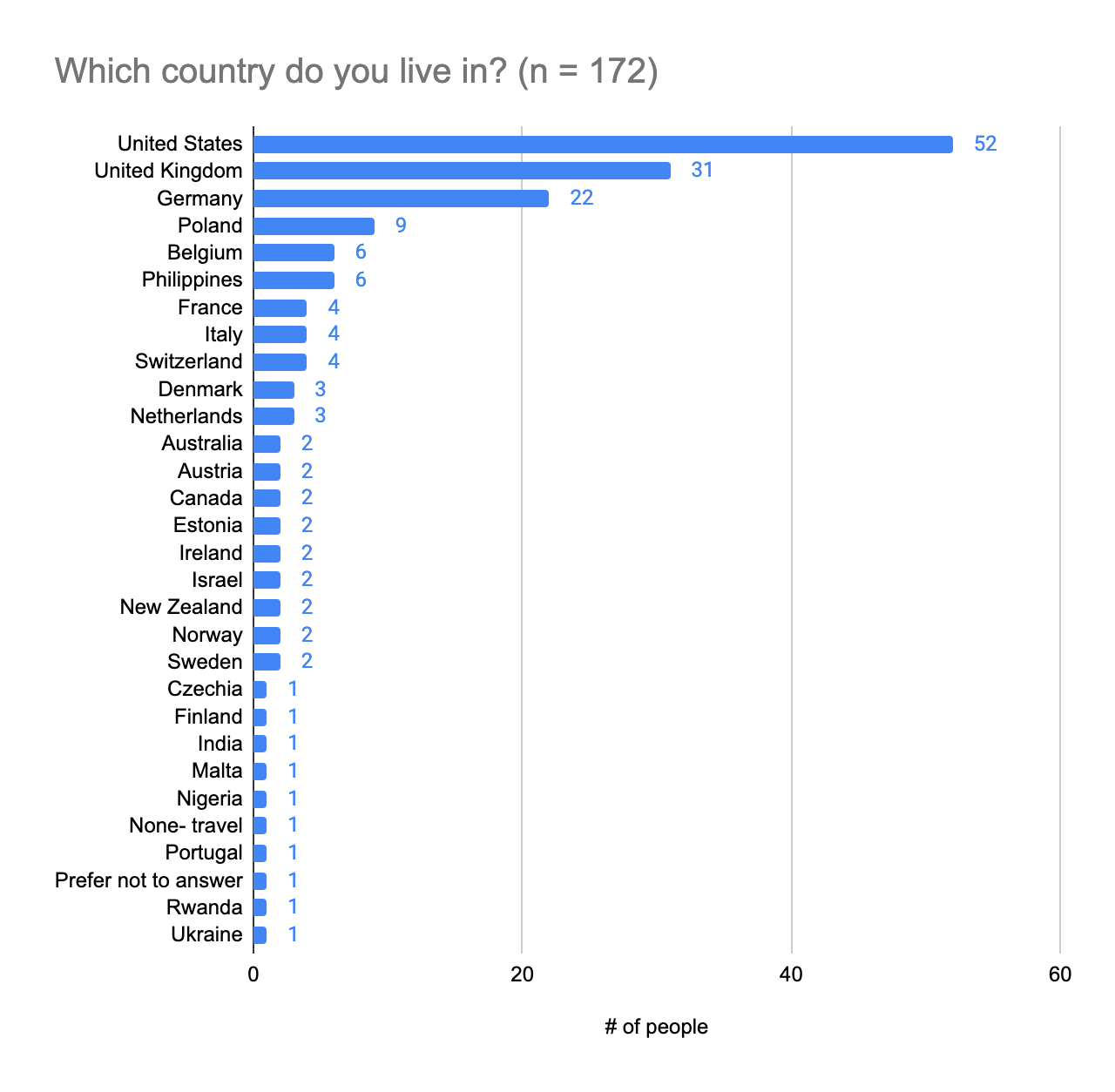
The majority of survey participants are based in the United States and United Kingdom.
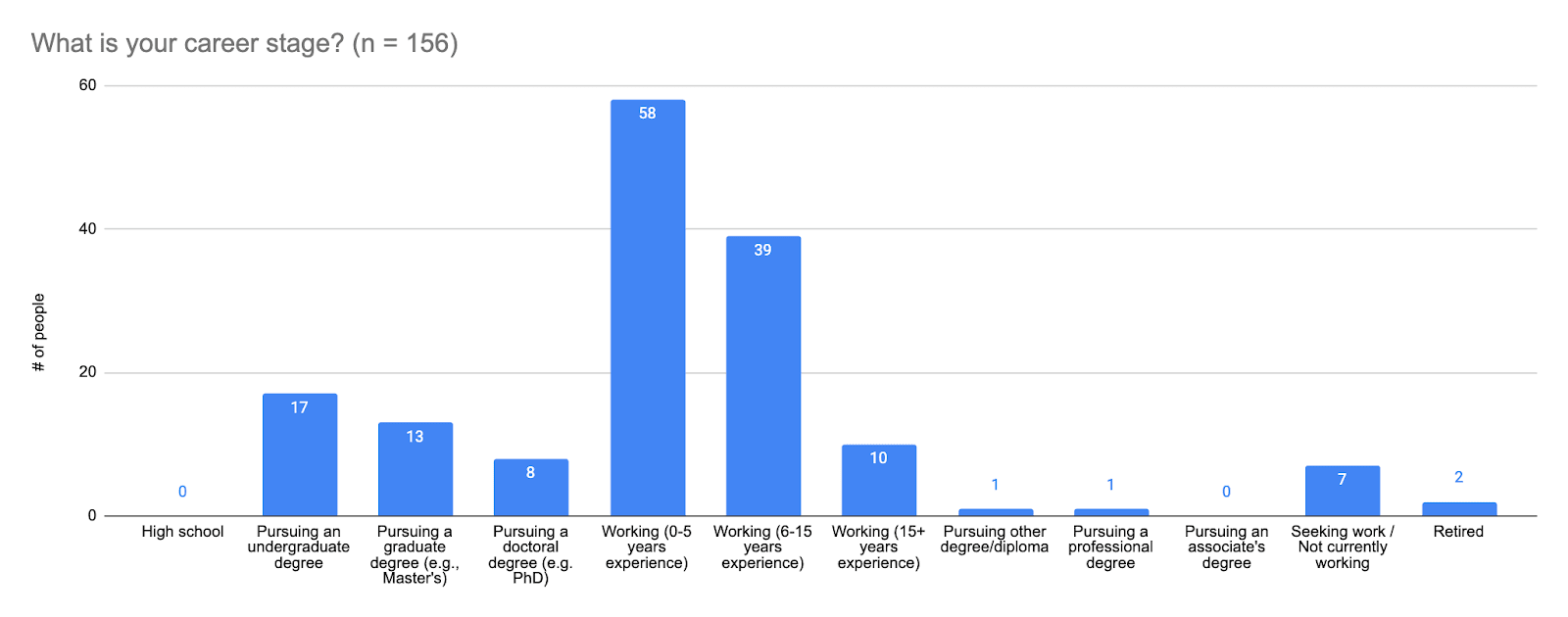
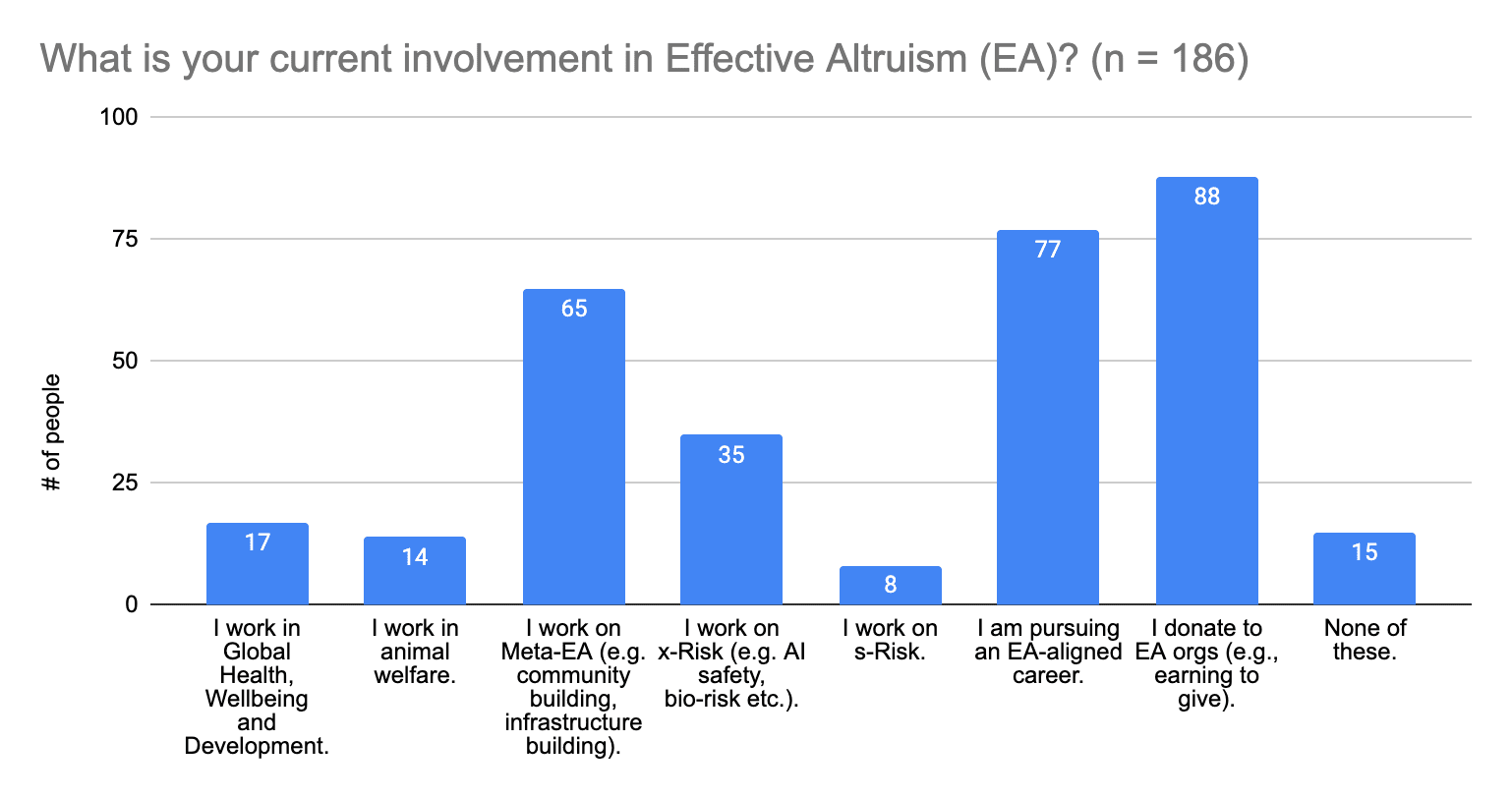
Answer choices from left to right are:
Most survey participants are working and have 0-15 years' work experience.
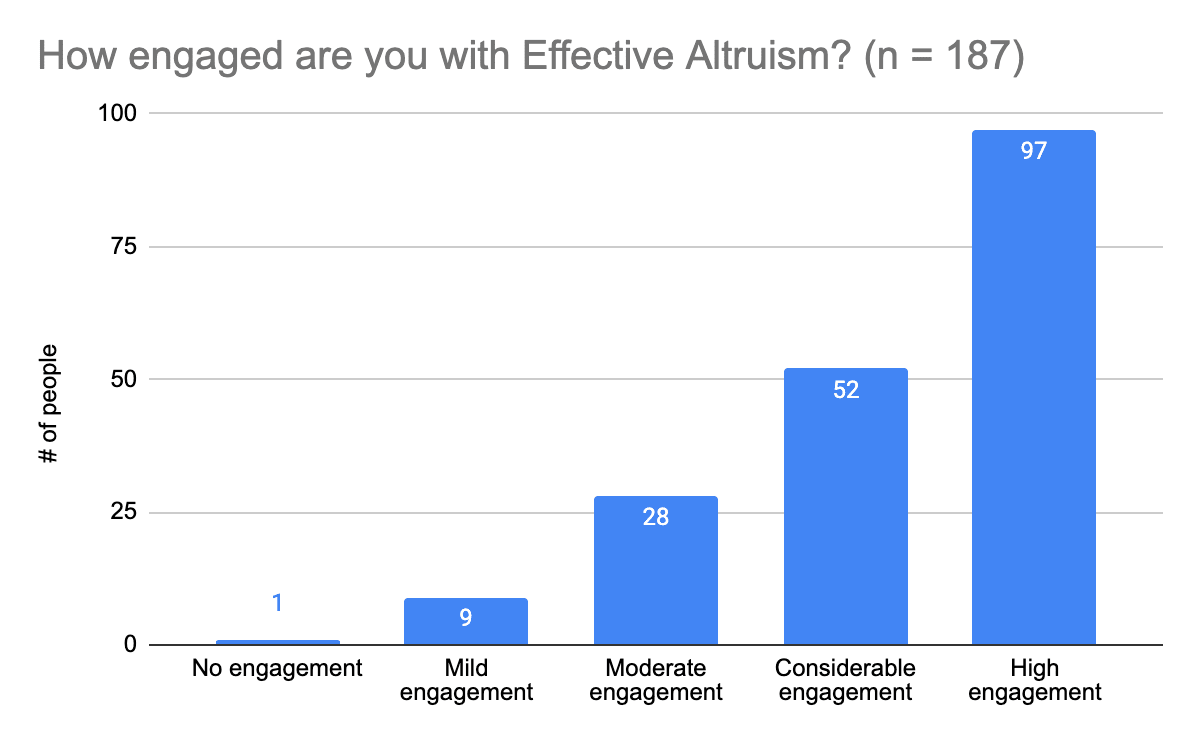
Answer choices were defined as follows:
Most survey participants are fairly engaged with Effective Altruism (considerable to high engagement).
People who answered this question could provide multiple answers, so survey participants who are involved in multiple sectors provided multiple answers.
This section was geared toward getting a more granular view of what community members struggle with in terms of their mental health. Building off of lessons learned from the 2021 EA Mental Health Survey, the questions are structured to provide more extensive lists of options for people to choose from, and to make the distinction between mental health disorders and mental health topics (which can include symptoms of disorders).
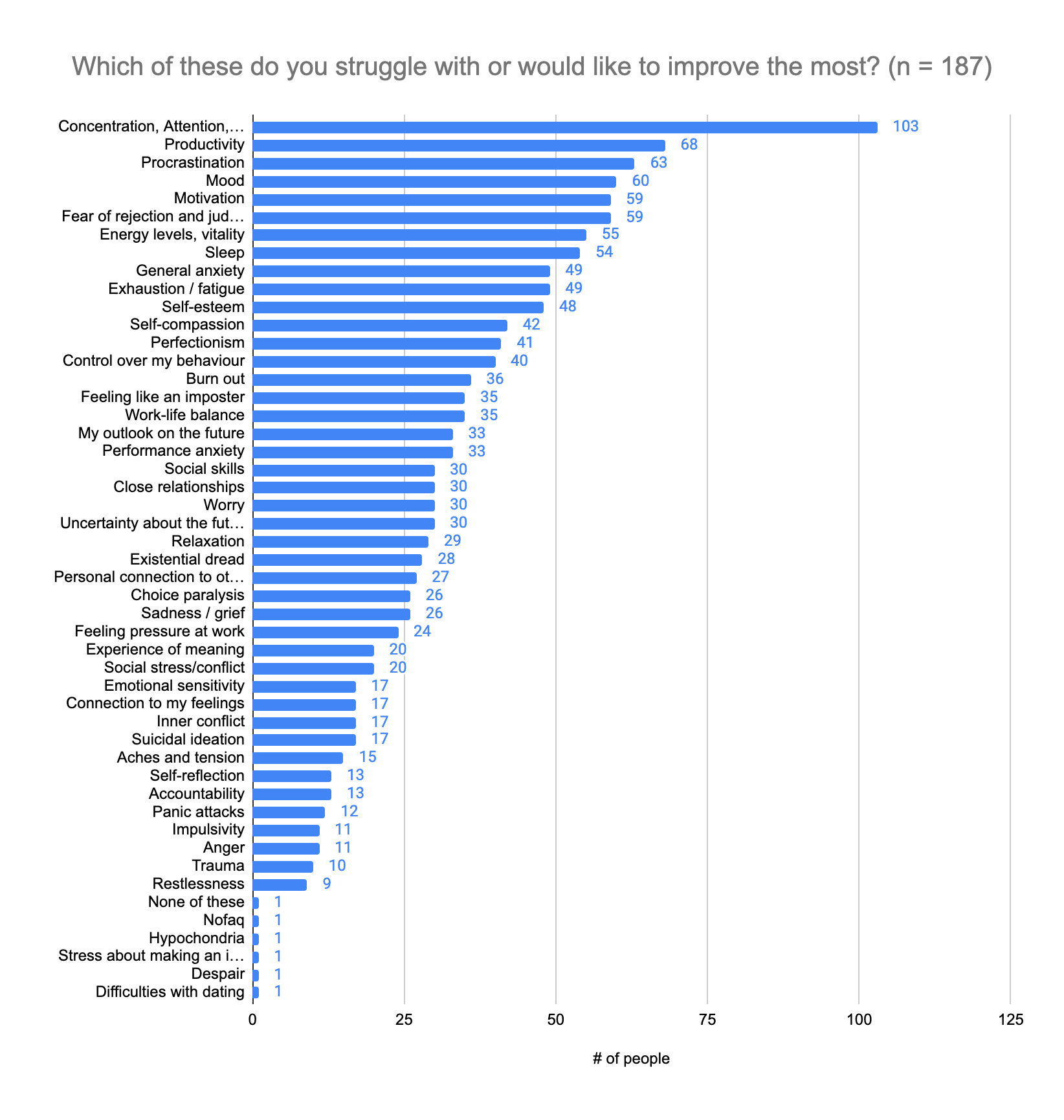
People struggle the most with concentration, attention, and focus (n =103; 55%), followed by productivity (n = 68; 36%) and procrastination (n = 63; 34%). The topics with ellipses are:
Please note: People who answered this question could provide multiple answers.
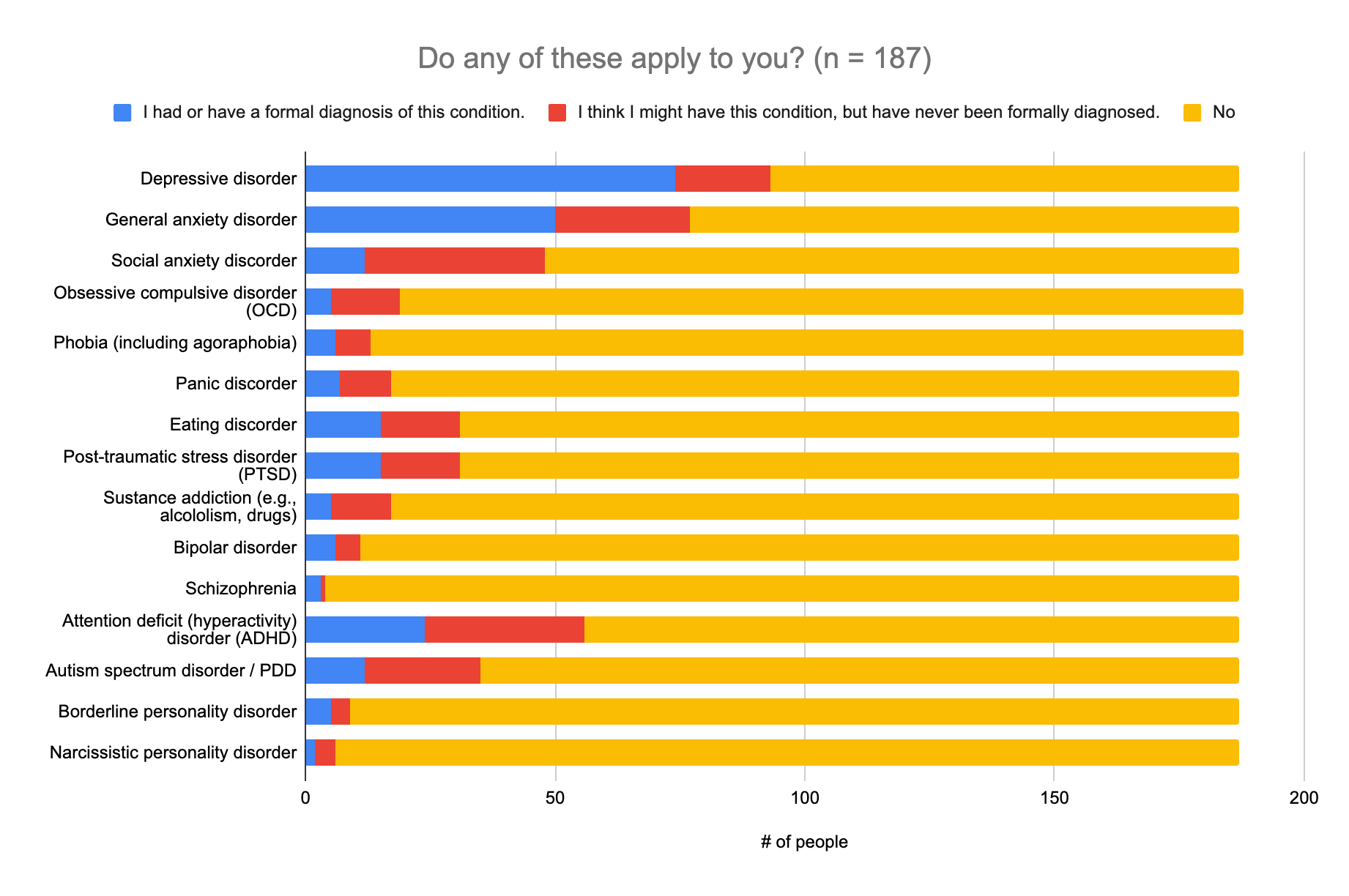
 (2) Applicable categories of disorders
(2) Applicable categories of disordersThis question was meant to get a better idea of the prevalence of diagnosed and suspected mental health struggles in the community, and listed out categories of disorders as defined in the DSM-V. The distinction in this question is important for determining what kind of help people will be able to access (which can depend on having a diagnosis), and therefore determining how to prioritize what information is needed.
 (3) Other disorders and conditions
(3) Other disorders and conditionsOther disorders (or suspected disorders) and conditions provided were:
Answers that were reclassified and added to Question 2, based on the DSM-V were:
The top three symptoms or topics people struggle the most with are concentration, attention, and focus (n =103; 55%), followed by productivity (n = 68; 36%) and procrastination (n = 63; 34%). Over a quarter of those surveyed (n = 50+; 27%) have been diagnosed with a depressive disorder, an anxiety disorder, or ADHD, or feel that they have a disorder that falls into one of these categories, but have not been diagnosed. It would therefore probably be helpful to focus on providing more information on dealing with or finding support for anxiety, depression, and ADHD, and improving one’s concentration, attention, focus, and productivity, as well overcoming procrastination.
This section was designed to gauge the state of mental well-being across the wider community, and satisfaction with one's life, relationships, community, and productivity.
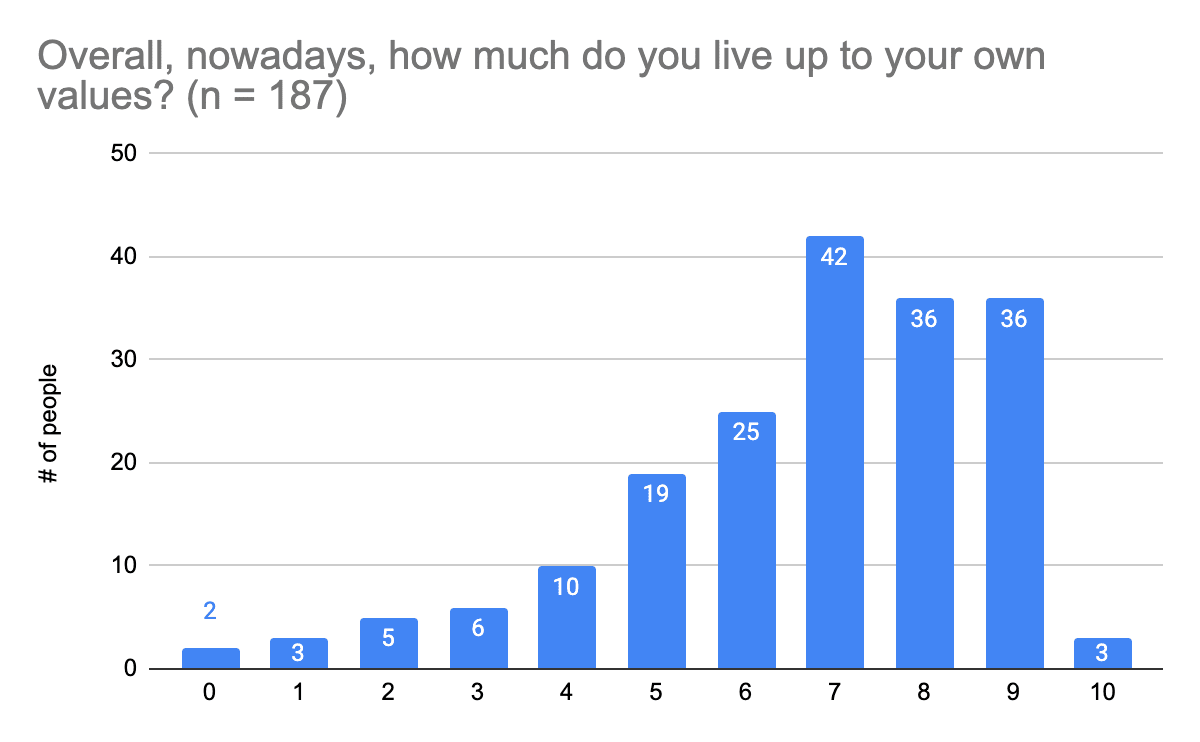
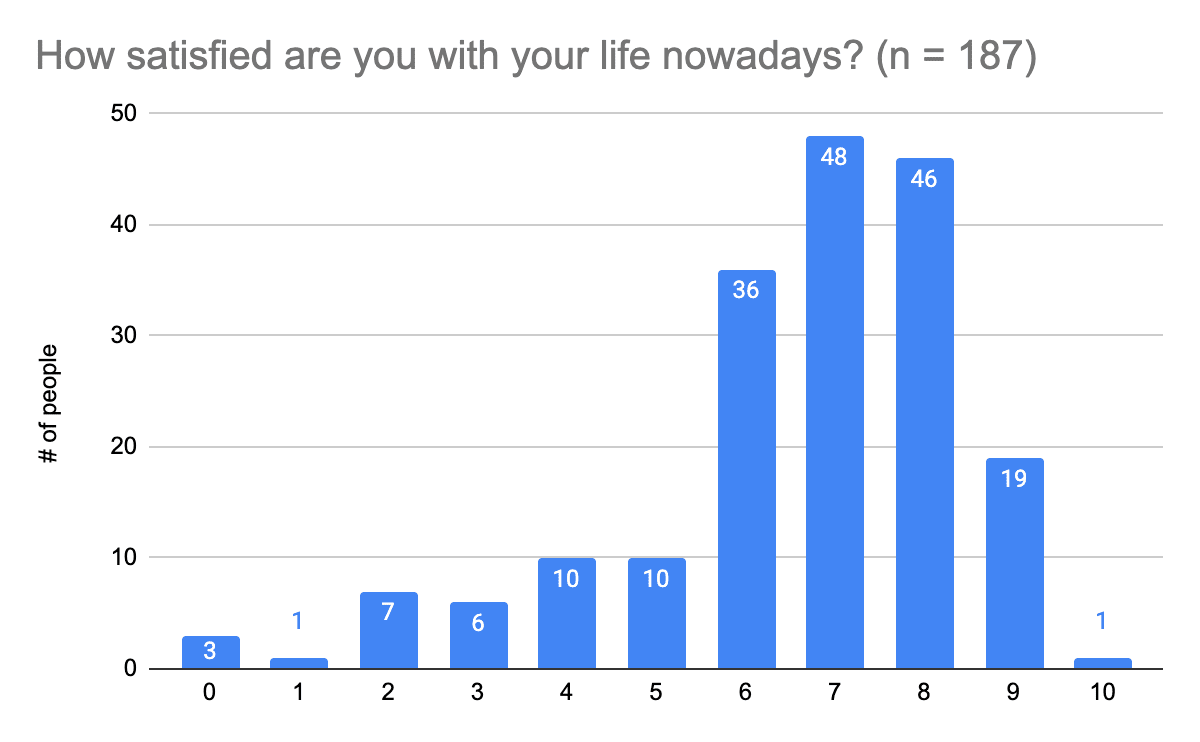
Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”.
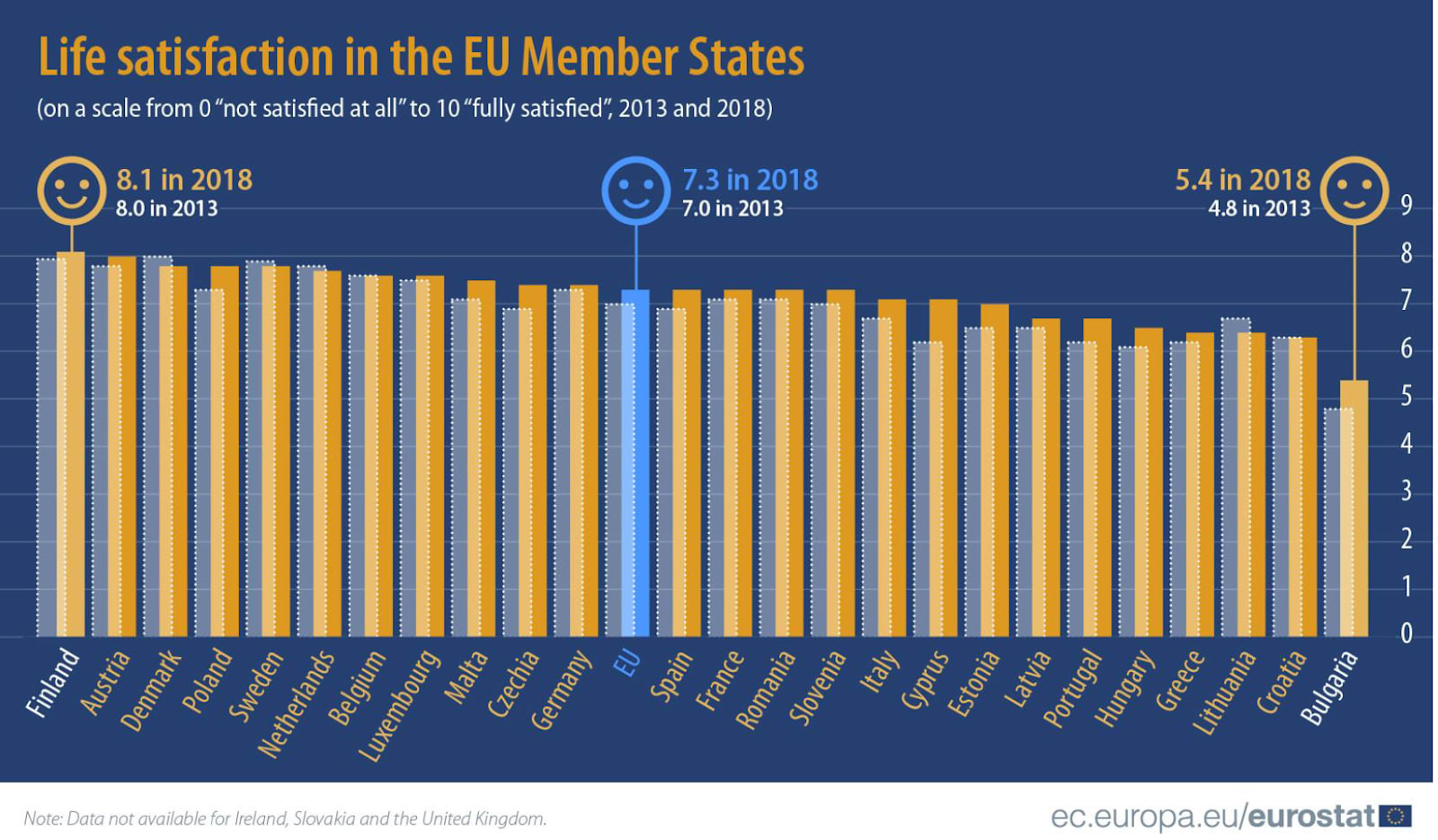
We used the same question that was asked in the report ‘Personal and economic wellbeing' by the Office of National Statistics, and in 2018 the average overall life satisfaction in the EU was 7.3, while in our survey it was 6.6. The life satisfaction of people in the EA community who filled out this survey in 2023 seems to be lower than the one of the typical EU member in 2018, and is similar to the one of people in Greece or Hungary (see Figure 1).
Figure 1. Results of the report Personal and economic wellbeing
Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”.
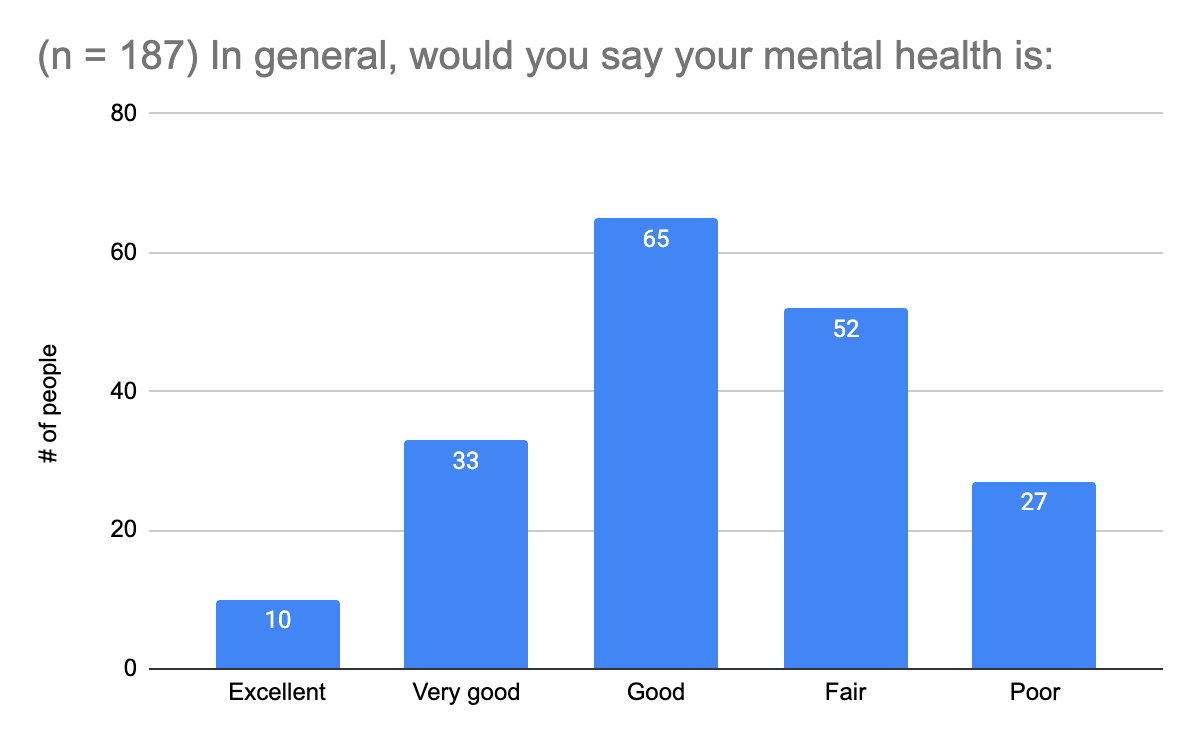
 (3) Mental health status
(3) Mental health statusWe asked a single standardized item question to self-rate mental health (the SRMH). In this scoping review (2014), you can find out more about the item, correlates, and applications.
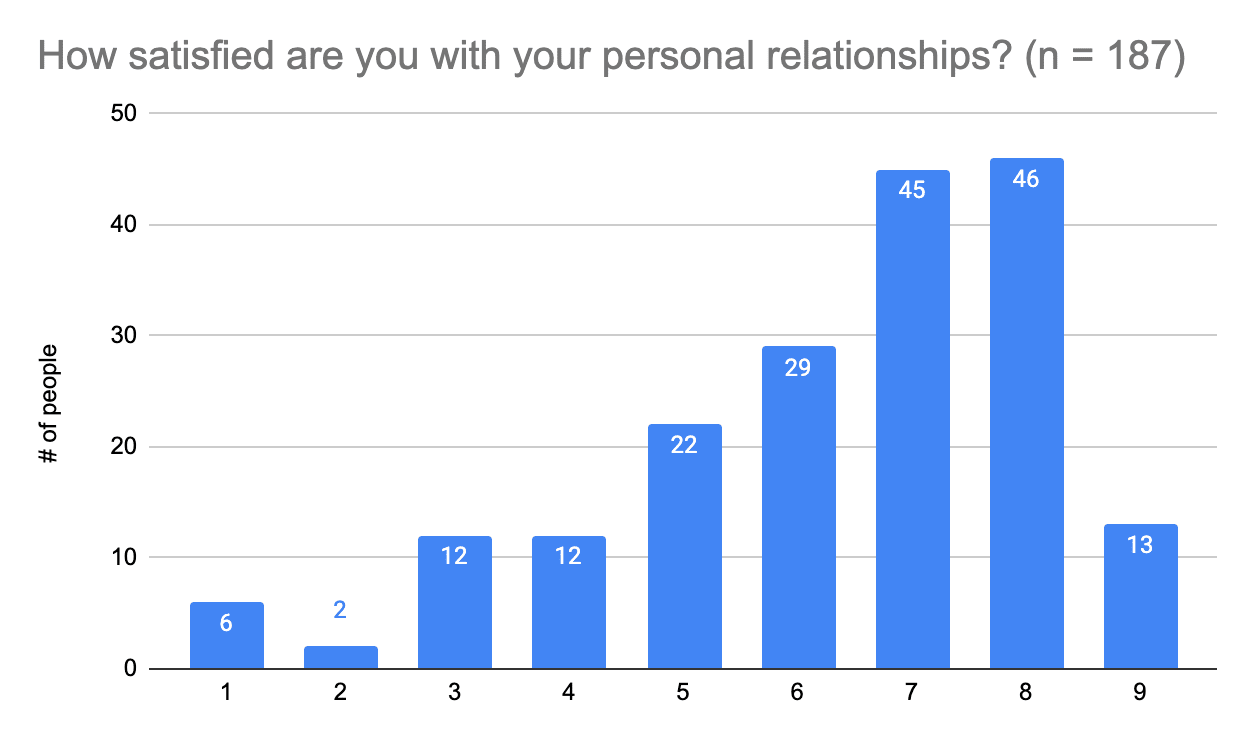
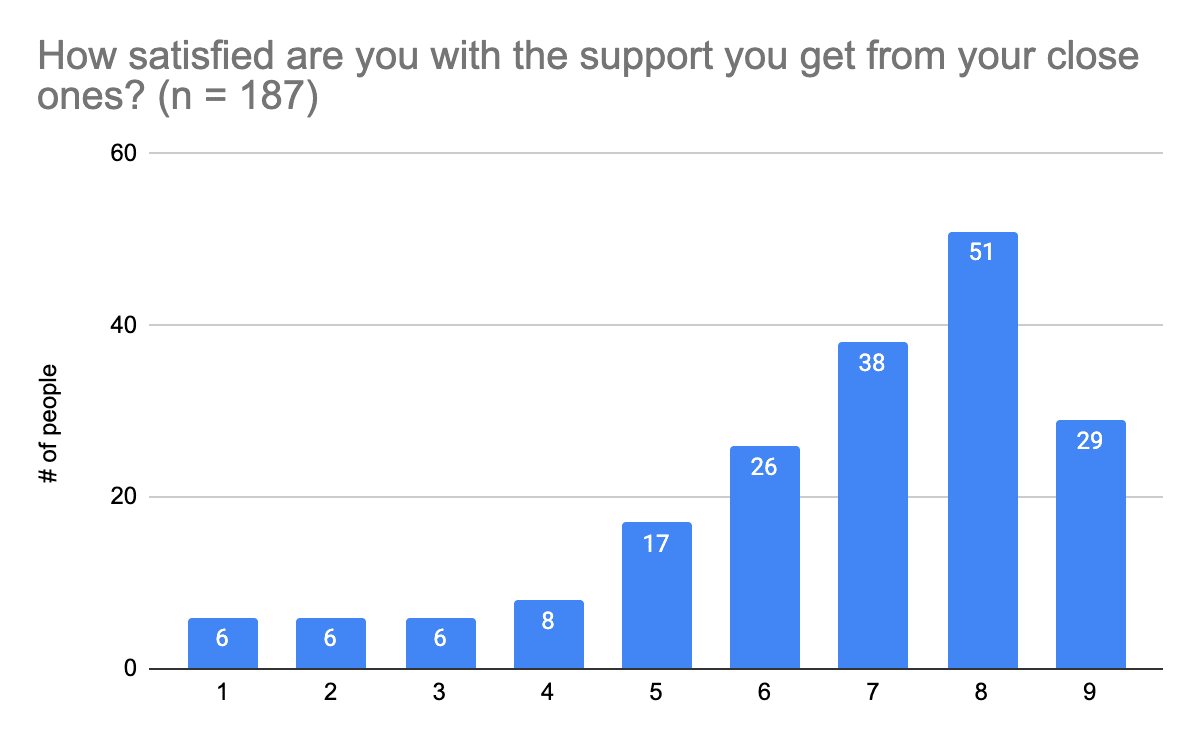
Answers to this question were on a scale of 1 to 9, where 1 was “Very dissatisfied” and 9 was “Very satisfied”.
 (5) Satisfaction with support in close personal relationships (x̄=6.7, Mdn.=7.0 SD=2)
(5) Satisfaction with support in close personal relationships (x̄=6.7, Mdn.=7.0 SD=2)Answers to this question were on a scale of 1 to 9, where 1 was “Very dissatisfied” and 10 was “Very satisfied”.
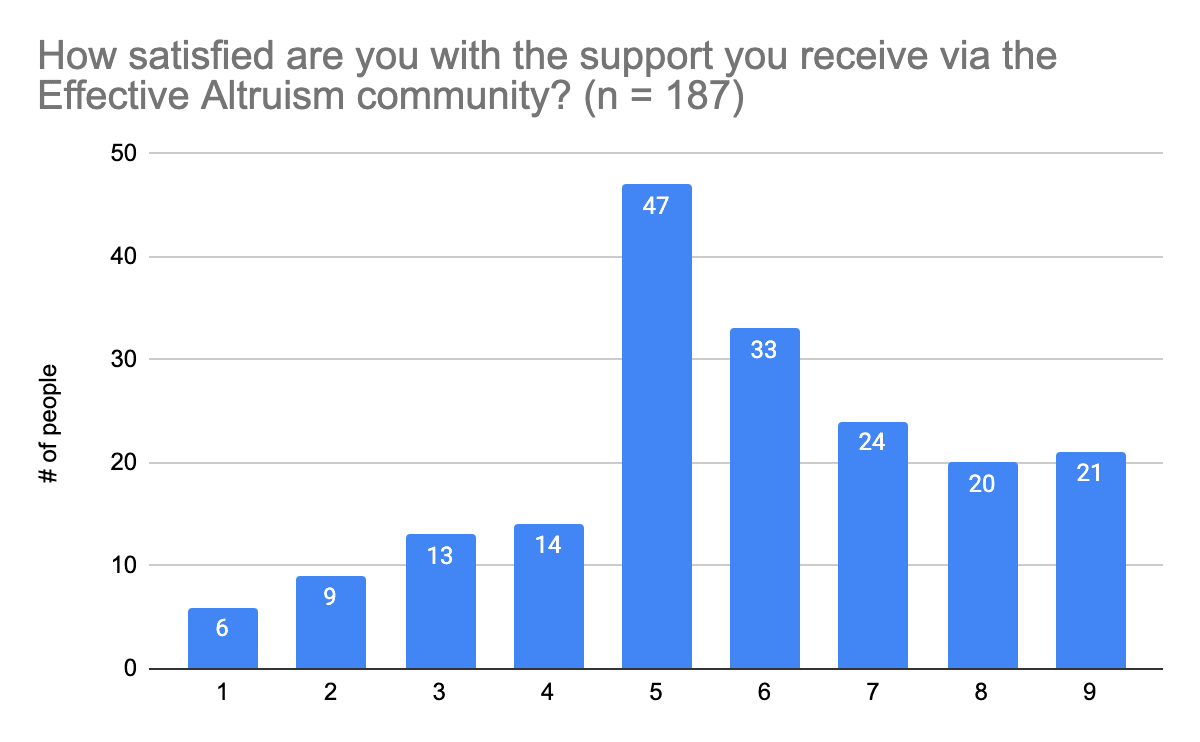
 (6) Satisfaction with support from the Effective Altruism community (x̄=5.7, SD=2.1)
(6) Satisfaction with support from the Effective Altruism community (x̄=5.7, SD=2.1)Answers to this question were on a scale of 1 to 9, where 1 was “Strongly disagree” and 9 was “Strongly agree”.
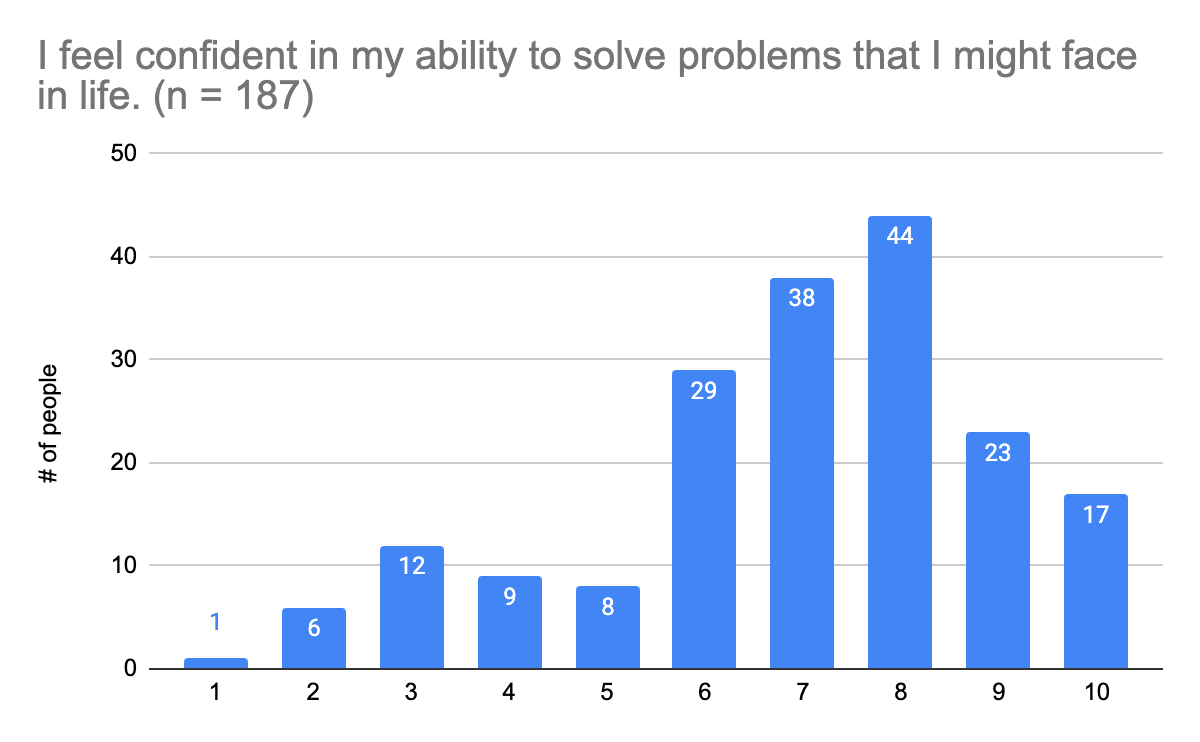
Answers to this question were on a scale of 1 to 10, where 1 was “Very dissatisfied” and 10 was “Very satisfied”. We used this standardized single item to measure self-efficacy. Find out more about the item in the corresponding paper (2016) here.
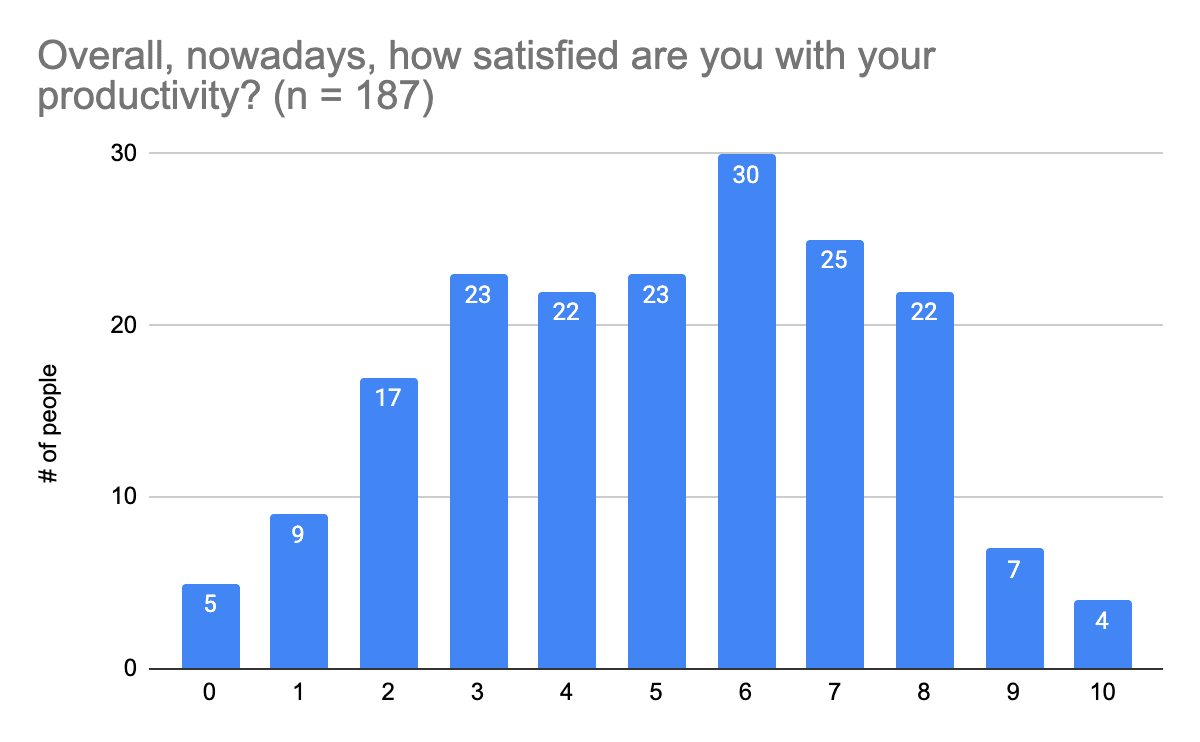
 (8) Satisfaction with productivity (x̄=5.1, SD=2.4)
(8) Satisfaction with productivity (x̄=5.1, SD=2.4)Answers to this question were on a scale of 0 to 10, where 0 was “Not at all” and 10 was “Completely”. Satisfaction with productivity seems to be much lower than satisfaction with relationships and general life in the EA community members who took part in this survey.
This was a free-form response, so answers have been grouped into units of 10.
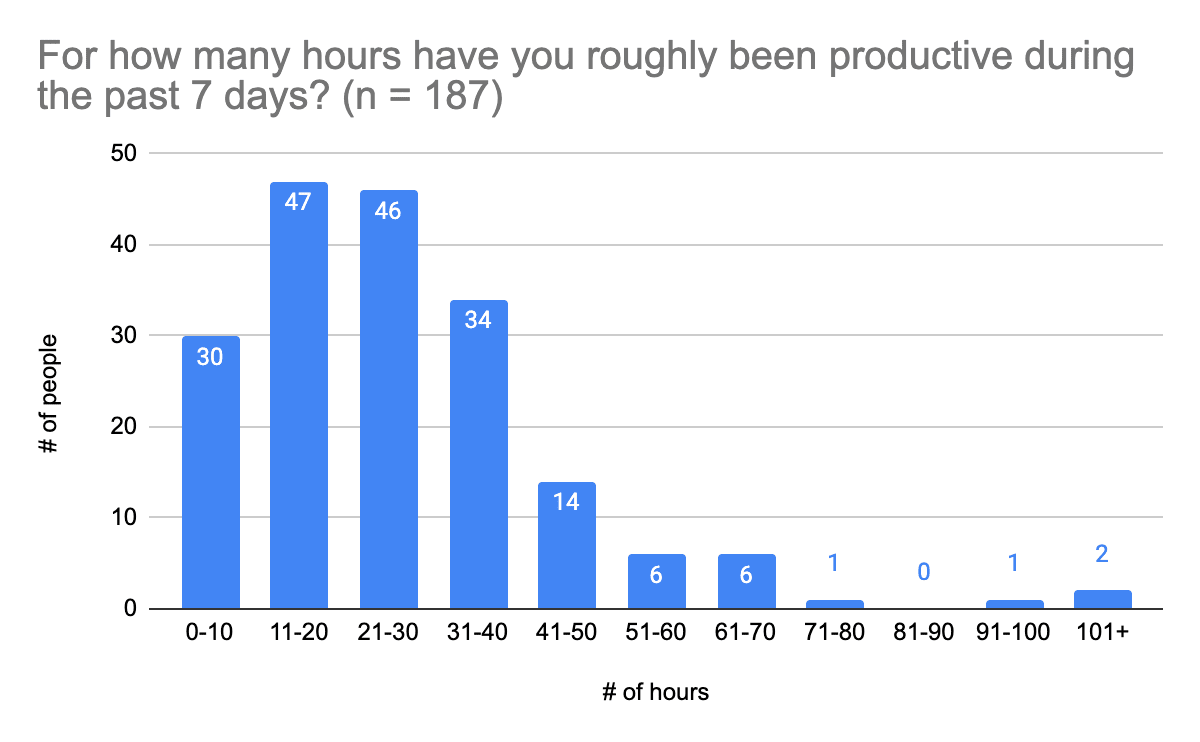
This was a free-form response, so answers have been grouped into units of 10.
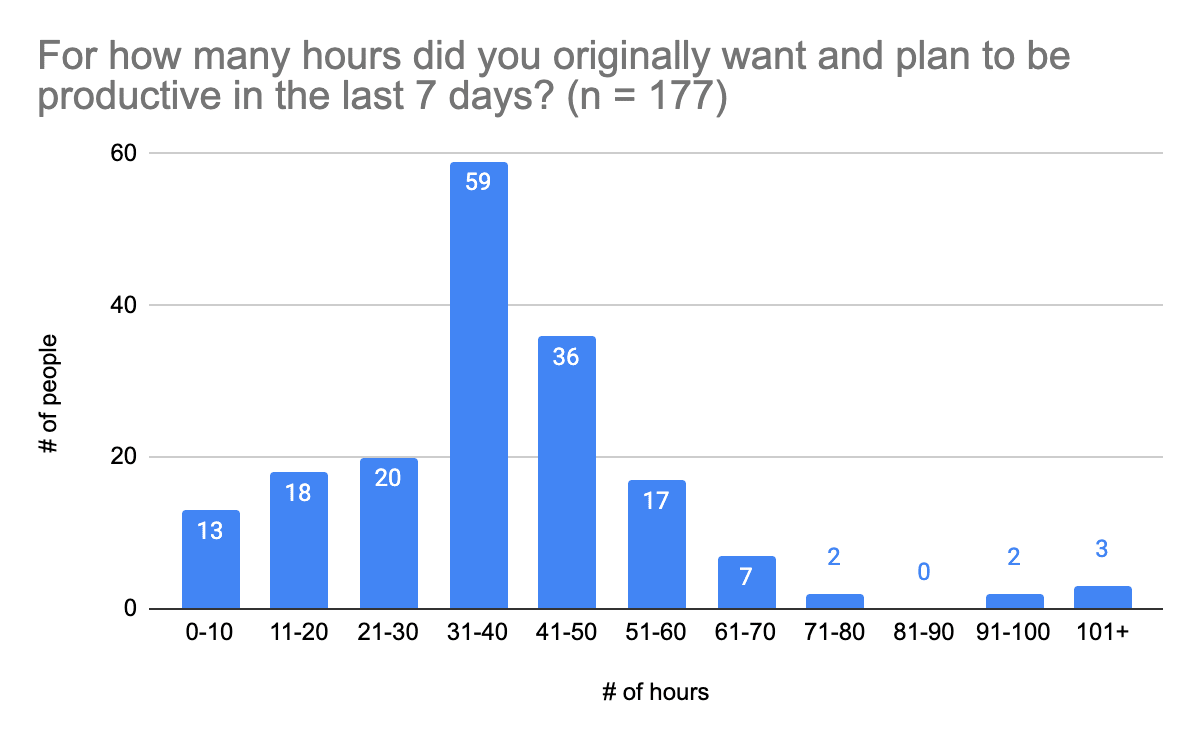
Visual comparison of planned versus actual hours of productivity:
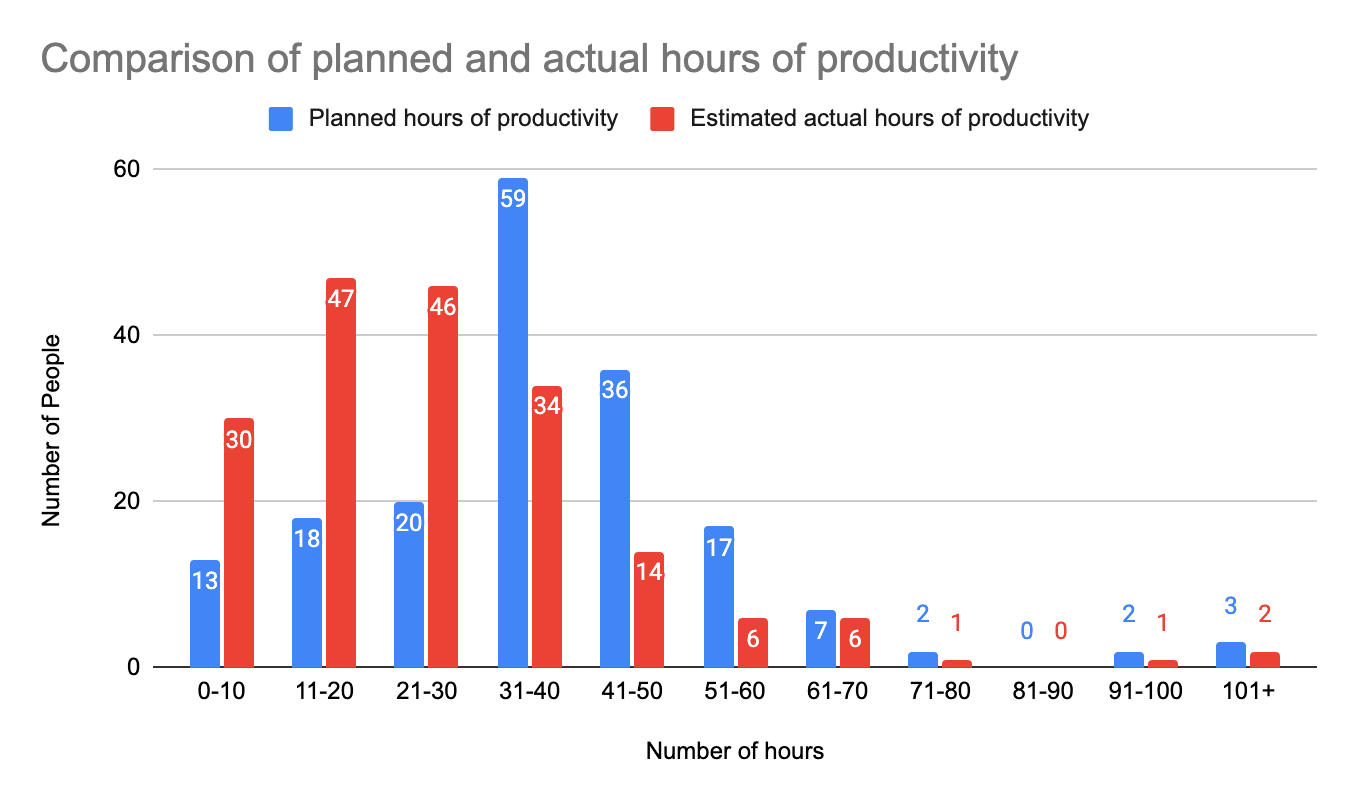
The results mean that people who filled out the survey estimated that they worked nearly 15 hours less than they had planned (x̄=14.9), and for roughly ⅔ of survey participants, two out of 3 hours were lost due to mental wellbeing or other internal reasons.
Answers to this question were on a scale of 0 to 10, where 0 was 0% and 10 was 100%.
Most people who completed this survey (n = 130; 70%) are generally satisfied with their lives nowadays (scores of 6-8 out of 10), but a few people (n = 20; 11%) are very satisfied (scores of 9 or 10). Similarly, most survey participants generally feel that they live up to their values (scores of 7-9 out of 10, n = 114; 61%), and would say their mental health is “good” or better (n = 108; 58%). Those who completed this survey are generally satisfied in their relationships (score 7+ out of 9, n = 104; 56%) and the support they get from their loved ones (score 7+ out of 9, n = 118; 63%). Most survey participants are generally somewhat satisfied with the support they get from the Effective Altruism community (score of 5-7 on 9-point scale, n = 104; 56%). So people generally experience good mental health and feel supported, but that doesn’t mean there isn’t room to improve life satisfaction and well-being, and increase feelings of support (especially given the information provided in the Demand for Interventions section of this post).
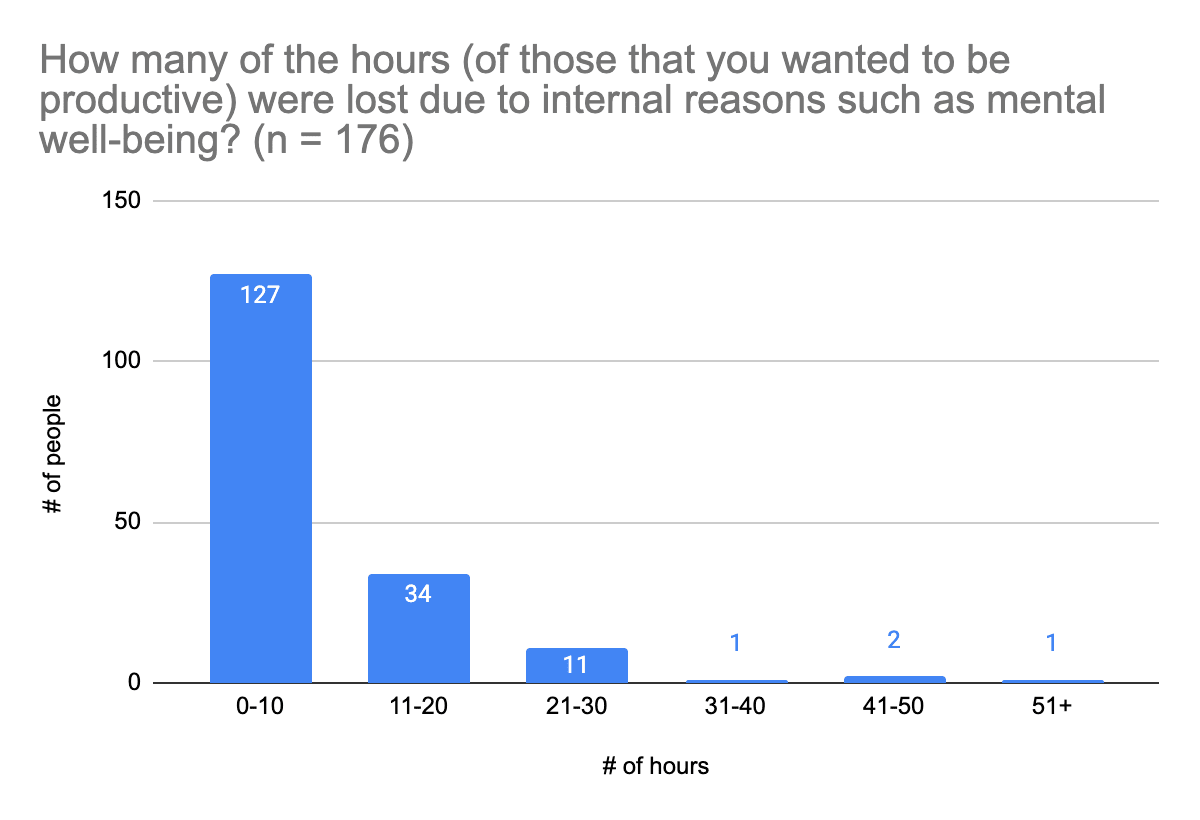
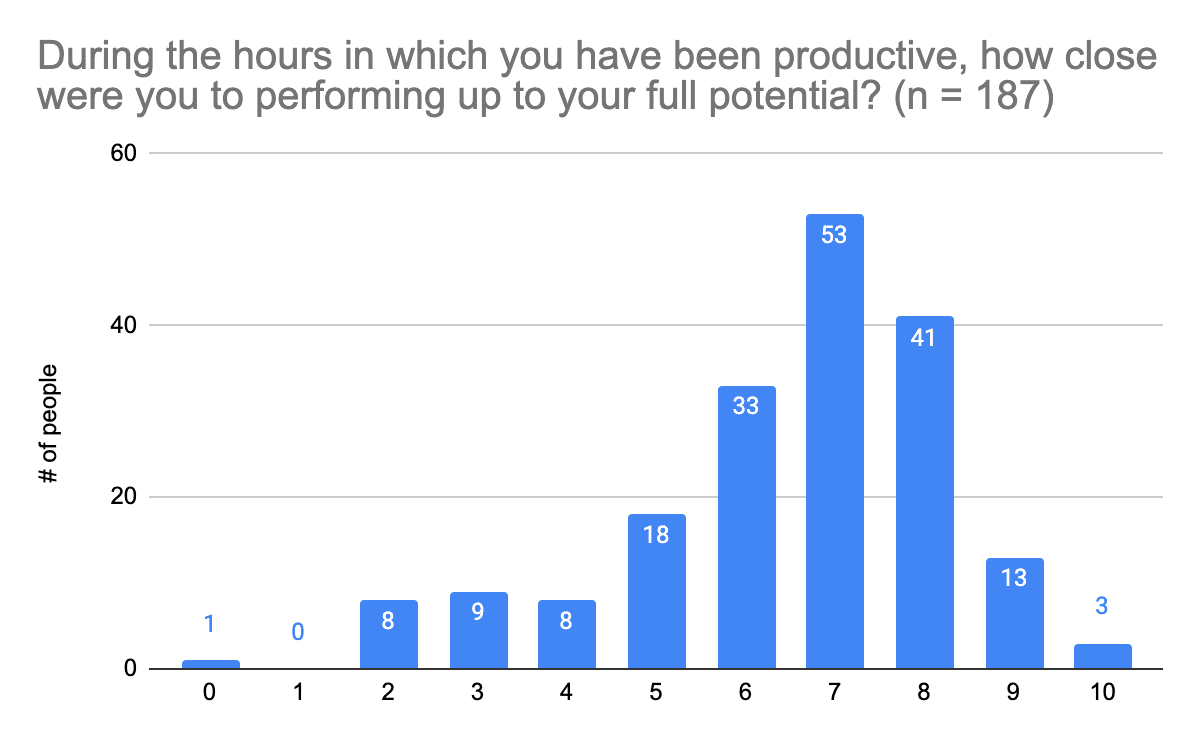
People appear to mostly be somewhat confident in their abilities to solve problems they face in life (score of 6 to 9 on 10-point scale, n = 134; 72%), and somewhat satisfied with their overall levels of productivity (score of 5 or above on 10-point scale, n = 111; 59%). Most survey participants were productive for up to 40 hours in a week (n = 157; 84%), though a lot of people were not as productive as they would have liked. A majority of participants (n = 112; 63%) aimed to be productive for 31-60 hours in a week; 54 people (31%) achieved this. Most survey participants lost up to 10 hours of productivity due to reasons related to mental well-being (n = 127; 72%). Most participants (though not all) also felt they were somewhat close to reaching their full potential during the hours in which they were productive (score of 6 or above on 10-point scale, n = 143; 76%); few felt they reached their full potential (score of 9+, n = 16; 9%). So it could be beneficial to provide people with information on improving their productivity, especially since this is a topic a lot of people (n = 68; 36%) said they struggle with.
This section was included to get a better idea of the types of mental health interventions community members have tried, including various types of behavioral interventions, therapeutic methods, and substances.
Please note: People who answered this question could provide multiple answers.
Please note: Numbers above the chart are associated with the color groups in the respective columns. Also, people who answered this question could provide multiple answers.
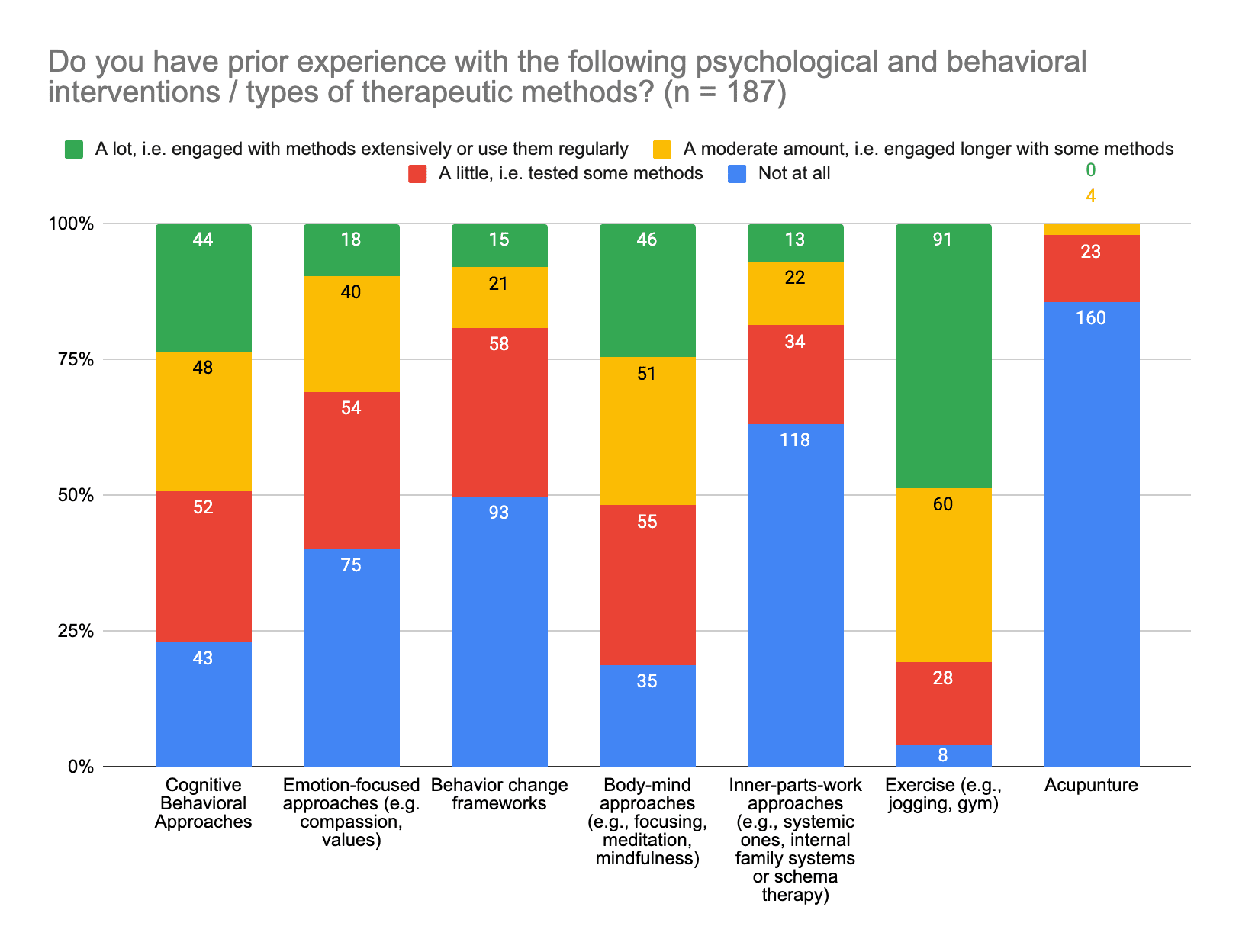
Categories were (top to bottom of chart):
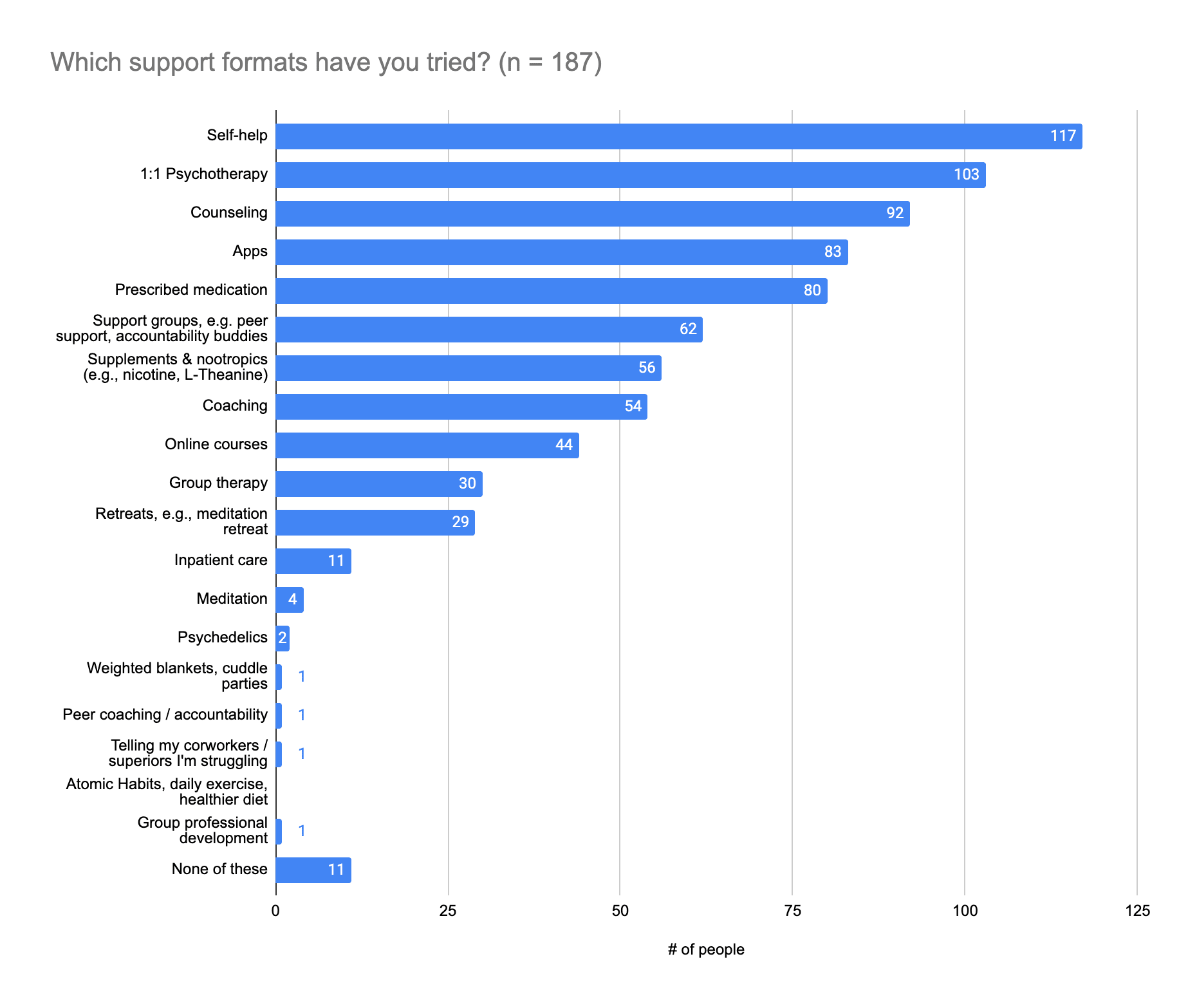
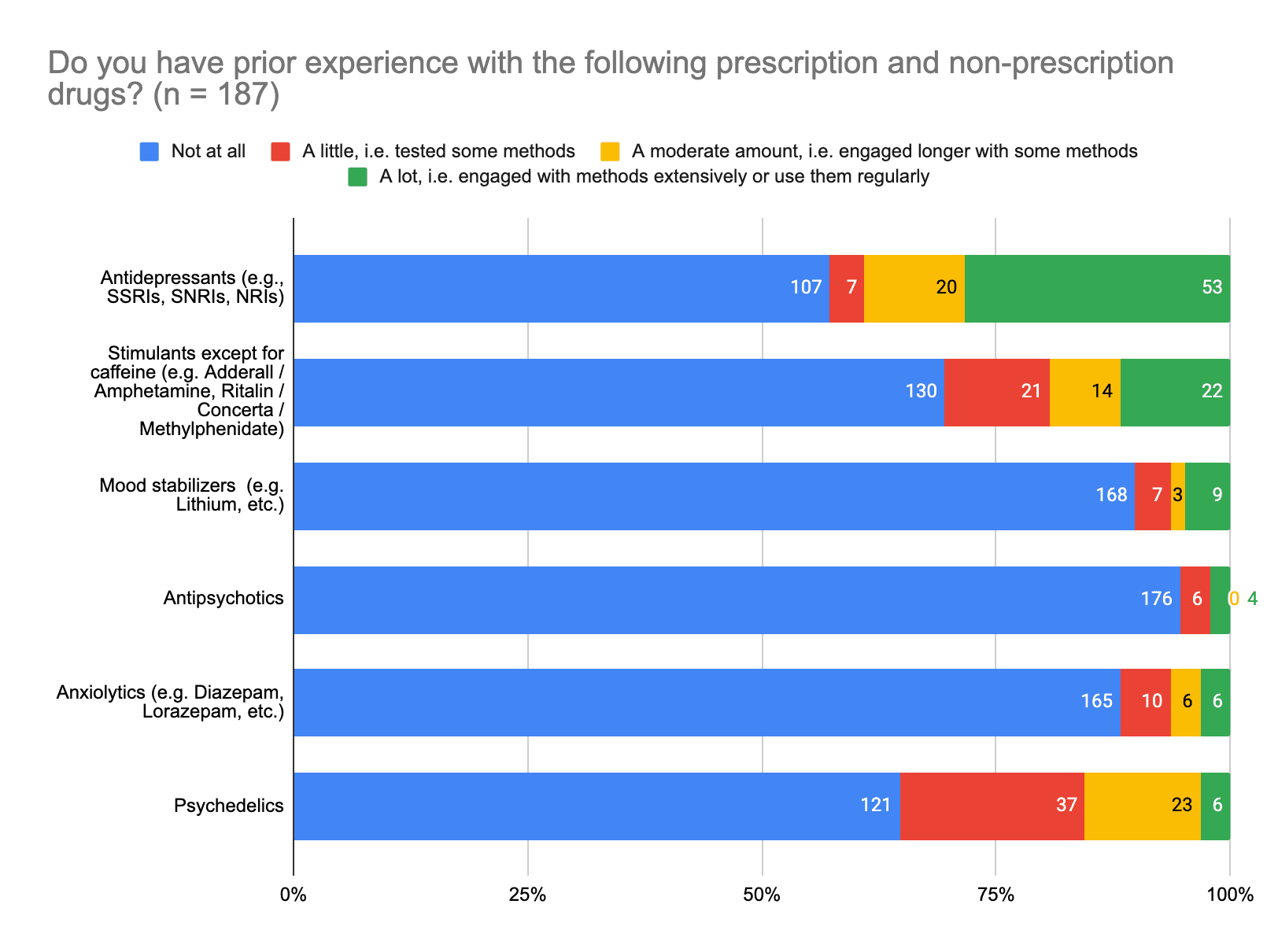
Please note: Numbers to the right margin of the chart are associated with the color groups in the respective rows. Also, people who answered this question could provide multiple answers.
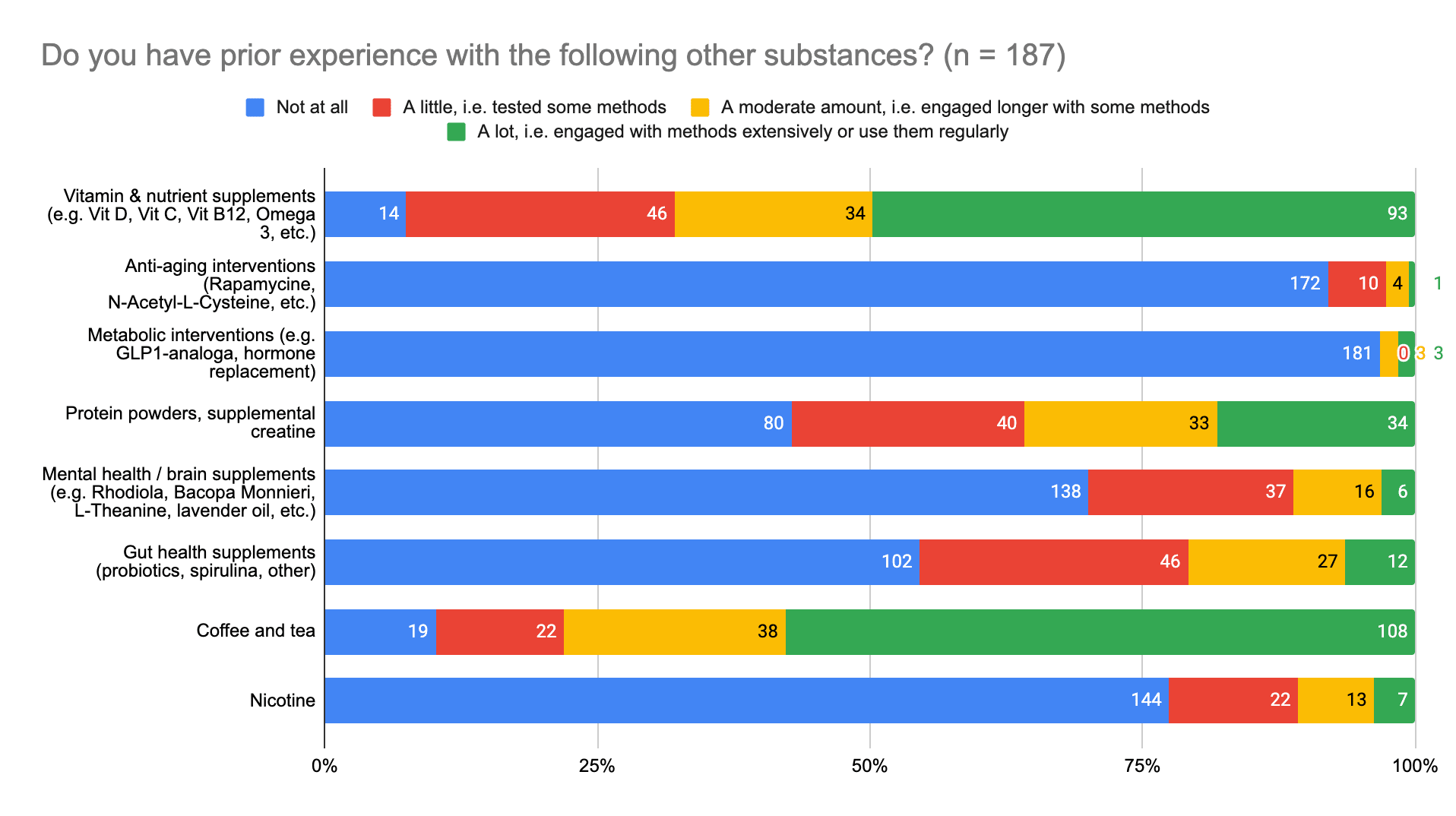
Please note: Numbers to the right margin of the chart are associated with the color groups in the respective rows. Also, people who answered this question could provide multiple answers.
Categories were (top to bottom of chart):
There was at least one response for each of the following:
The support formats most survey participants have tried are self-help (n = 117; 63%), 1:1 psychotherapy (n = 103; 55%), and counseling (n = 92; 49%). The next most popular were apps (n = 83; 44%) and prescribed medication (n = 80; 43%). It could therefore be helpful to provide people with information on support formats with which they are less familiar, such as support groups (n = 62; 33%), supplements and nootropics (n = 56; 30%), coaching (n = 54; 29%), online courses (n = 44; 24%), and atomic habits and other lifestyle changes, such a healthy diet and use of weighted blankets.
In terms of behavioral and psychological interventions, survey participants have engaged at least a little with exercise (n = 179; 96%), body-mind approaches (e.g., focusing, meditation, mindfulness) (n = 152; 81%), and cognitive behavioral approaches (n = 144; 77%), but not much with acupuncture and inner-parts-work (e.g., systemic methods, internal family systems or schema therapy). It might be a good idea then to provide information about these less popular approaches, as well as emotion focused approaches and behavior change frameworks, both of which some people have tested (n = 54 (29%) and 58 (31%), respectively), but fewer people have used (n = 58 (31%) and 36 (19%) respectively).
Most survey participants have had at least a little experience with antidepressants (n = 80; 43%) and stimulants (n = 57; 30%), and no experience with antipsychotics (n = 176; 94%), mood stabilizers (n = 168; 89%), and anxiolytics (n = 165; 88%). It might therefore be useful to point people to resources where they can access medical literature and medical support on these topics, should they wish to know more.
Most people have at least a little experience with vitamins and nutrient supplements (n = 173; 93%) and coffee and tea (n = 168; 90%), but not any with anti-aging interventions (n = 172; 92%) and metabolic interventions (n = 181; 97%). It might be helpful to provide information on substances people have no experience with, or have tested or used a moderately, though not extensively, such as protein powders and supplemental creatine (n = 73; 39%), mental health / brain supplements (e.g., Rhodiola, Bacopa Monnieri, L-Theanine, lavender oil) (n = 53; 28%), and gut health supplements (e.g., probiotics, spirulina) (n = 73; 39%), so that people can make more informed decisions about these substances, and whether or not they’d be helpful to them.
This included everything from lifestyle changes (e.g. better sleep), behavioral techniques (e.g. meditation), supplements (e.g. Omega 3, vitamins), nootropics (e.g. L-Theanine, Bacopa Monnieri), drugs (e.g. Ritalin / Concerta), to biohacking (e.g. hormone replacement).
Yes:
Reasons for answering "Partly":
Reasons for answering "No":
Please note: People who answered this question could provide multiple answers.
Other answers that were provided were:
Please note: People who answered this question could provide multiple answers.
Categories of psychological and behavioral interventions provided were (top to bottom of the chart):
Other answers provided were:
Types of therapy people emphasized as of interest or previously helpful:
Some people were not sure about how to respond to this question, because they didn't know what all of the options were or entail.
Please note: People who answered this question could provide multiple answers.
Categories of drugs were (top to bottom of the chart):
Other answers provided:
Please note: People who answered this question could provide multiple answers.
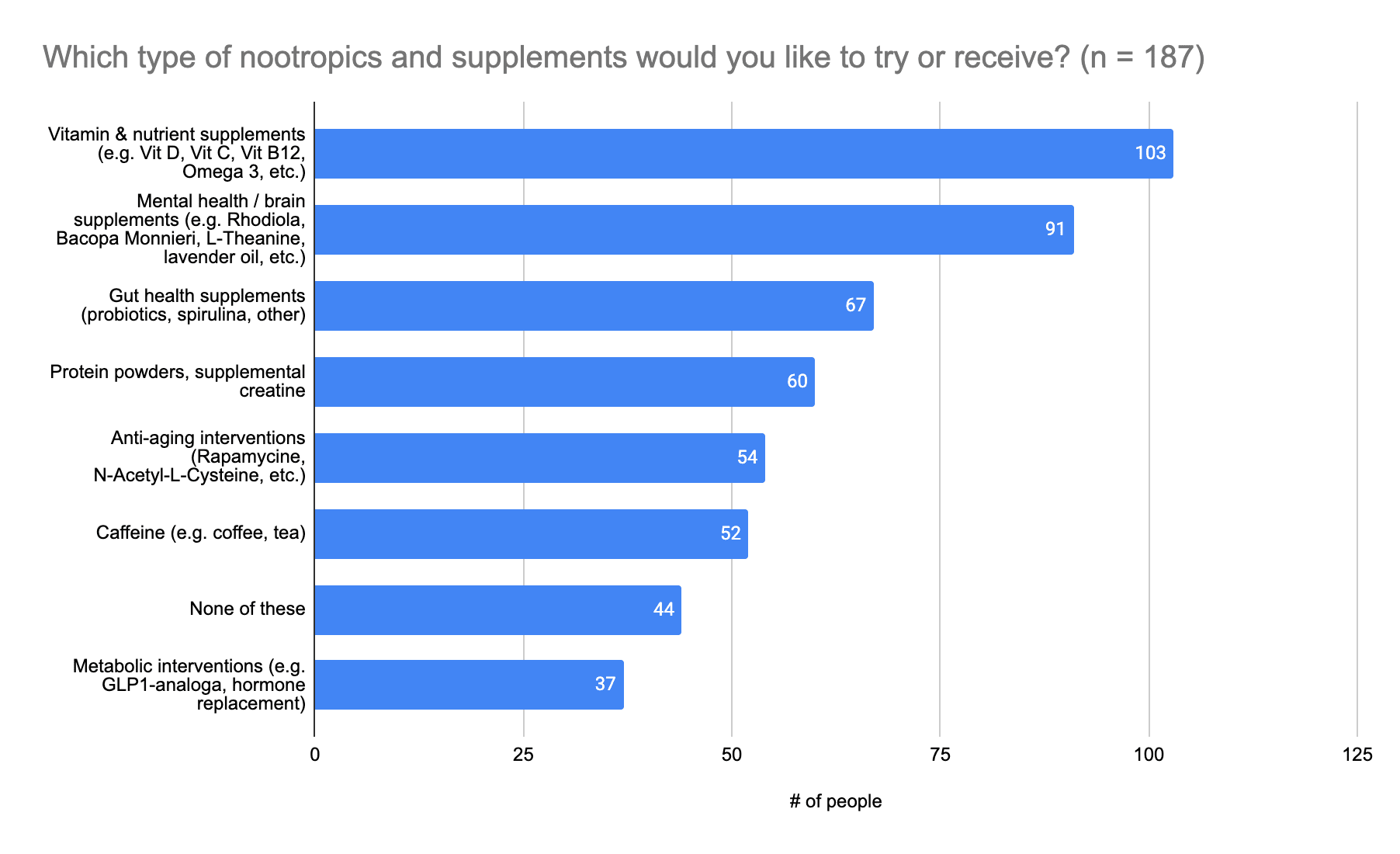
Categories of nootropics and supplements were (top to bottom of the chart):
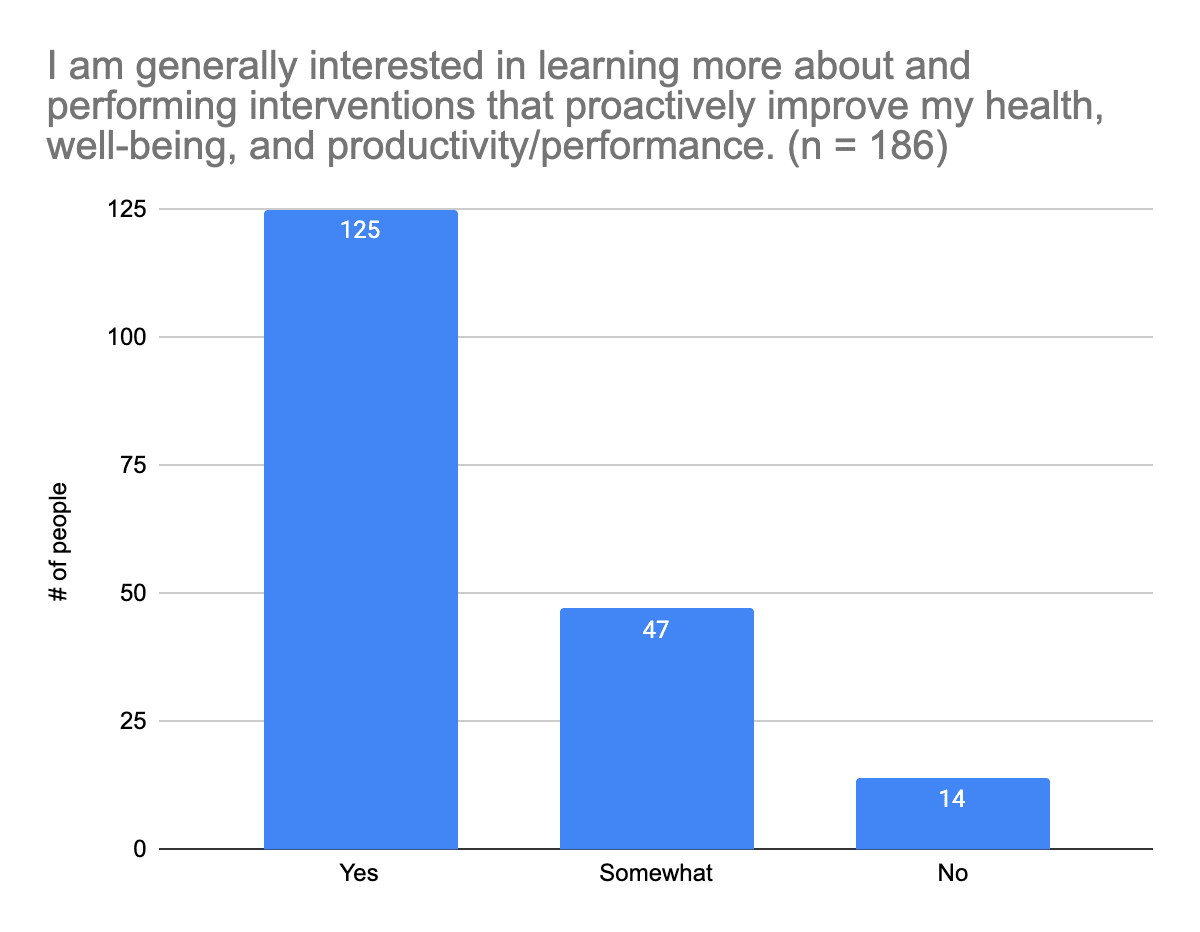
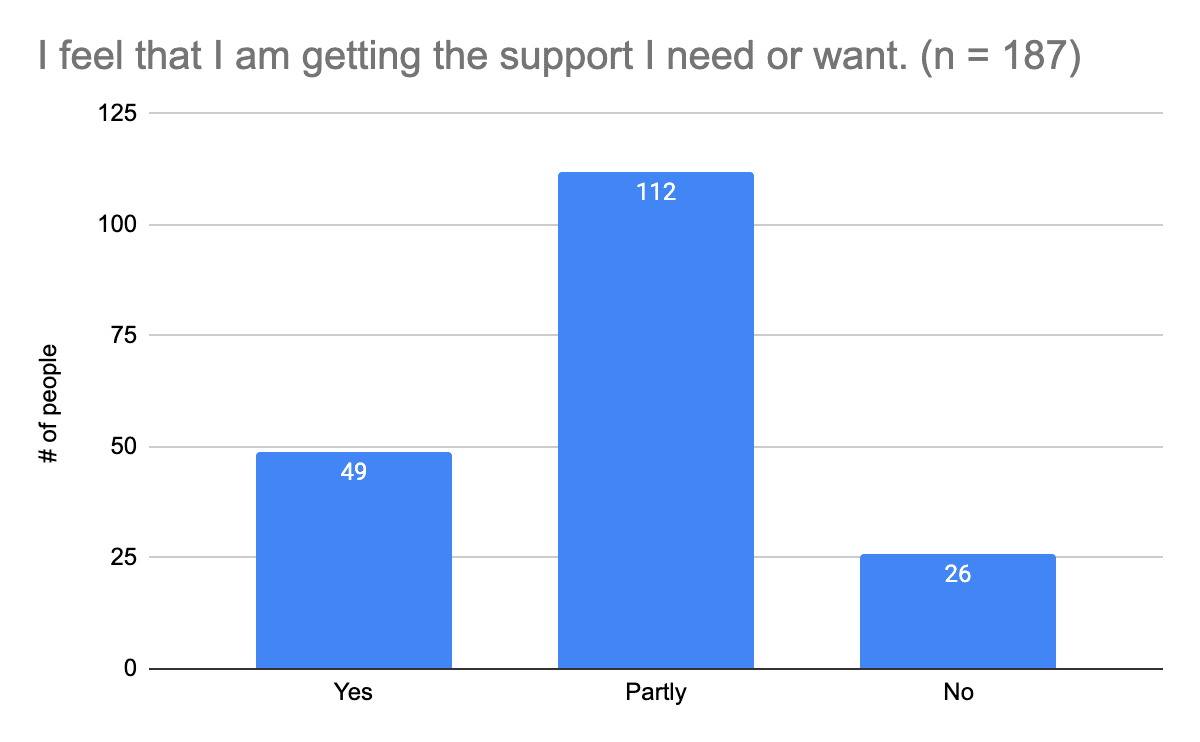
Most survey participants are interested (n = 125; 67%) or at least somewhat interested (n = 47; 25%) in learning more about and using interventions that could help them improve their health, well-being, and productivity or performance. About a quarter of survey participants feel they are getting the support they need or want (n = 49; 26%), but most feel that’s only partly true (n = 112; 60%), so there’s definitely room for improvement. Reasons for people feeling they are only partly receiving the support they need vary, but a common trend appears to be a need for help with mental health routines, priorities and structure, and help with feeling comfortable understanding and communicating what one is feeling and needs, and finding people with whom one is comfortable discussing those feelings and needs.
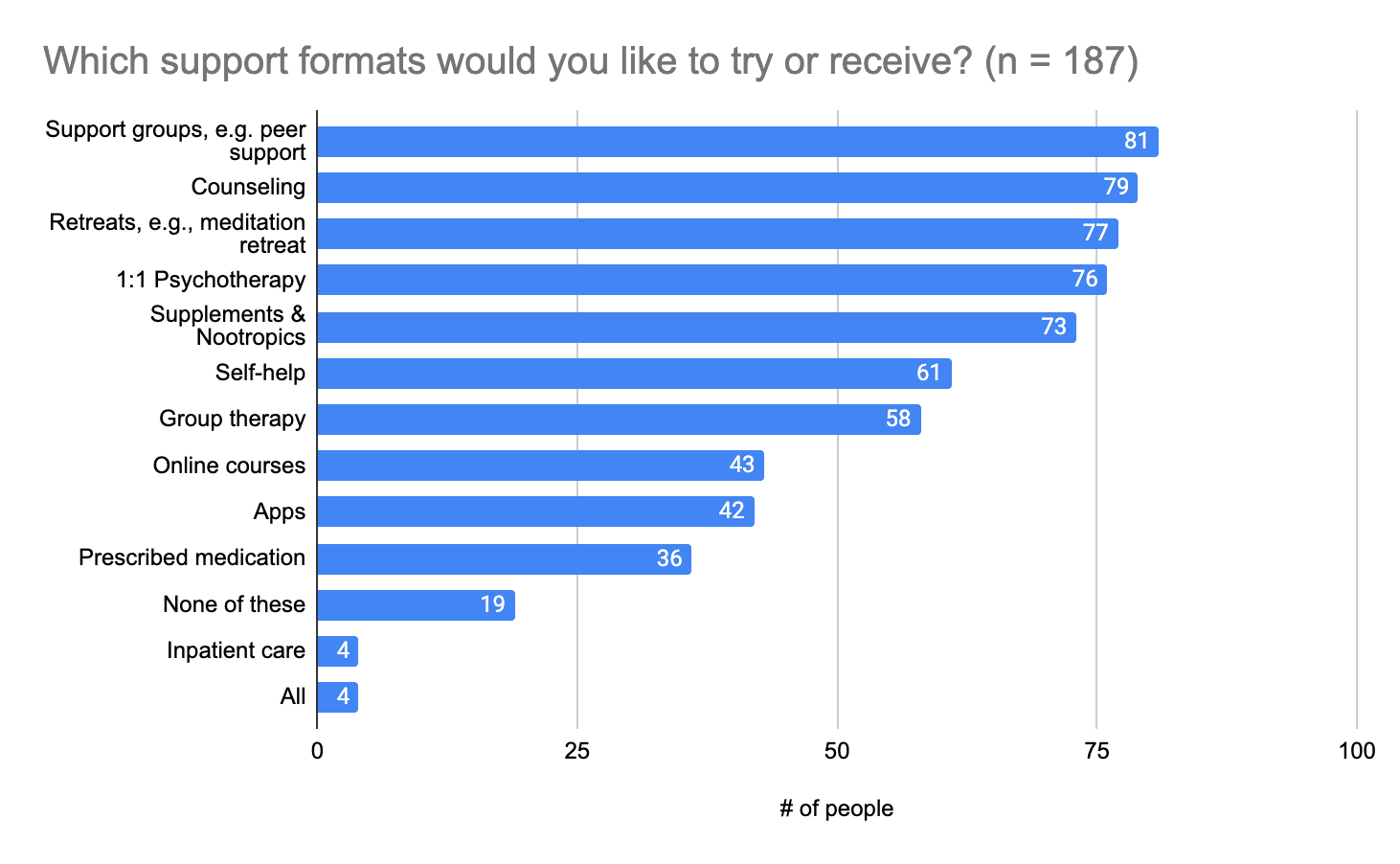
The top five support formats survey participants are interested in trying are support groups (n = 81; 43%), counseling (n = 79; 42%), retreats (such as meditation retreats (n = 77; 41%), 1:1 psychotherapy (n = 76; 41%), and supplements and nootropics (n = 73; 39%). People are also generally interested in trying all of the behavioral and psychological interventions listed (n = 79+; at least 42%), with the exception of acupuncture.
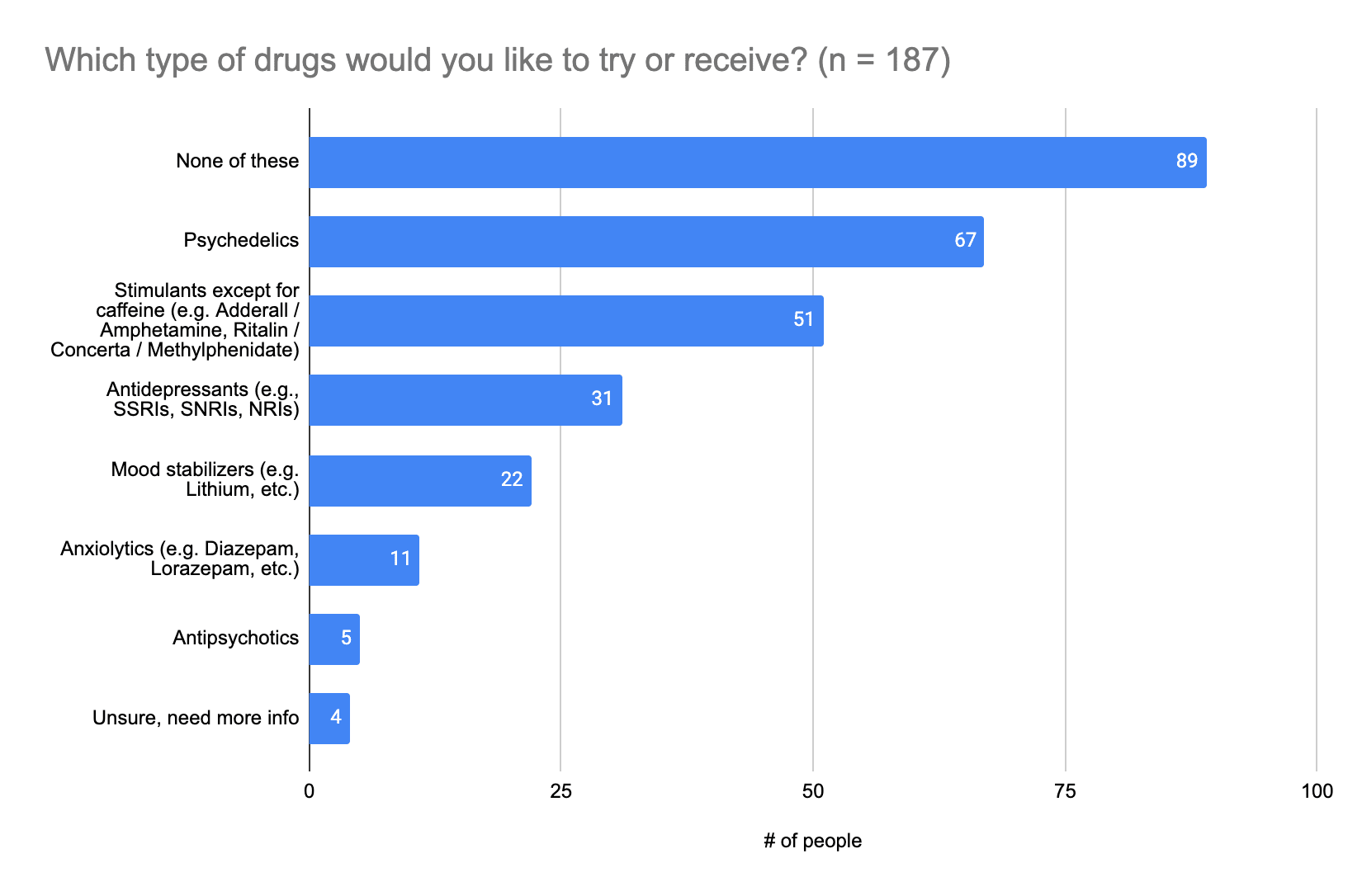
In terms of drugs, a lot of people would like to try psychedelics (n = 67; 36%) and stimulants (n = 51; 27%), and in terms of nootropics and supplements, there’s a lot of interest in trying vitamins and nutrient supplements (n = 103; 55%), as well as mental health / brain supplements (n = 91; 49%).[1]
The answer was provided by selecting the missing word in the sentence “The likelihood of me using an intervention is ... by this criterion.”
Answer options were:
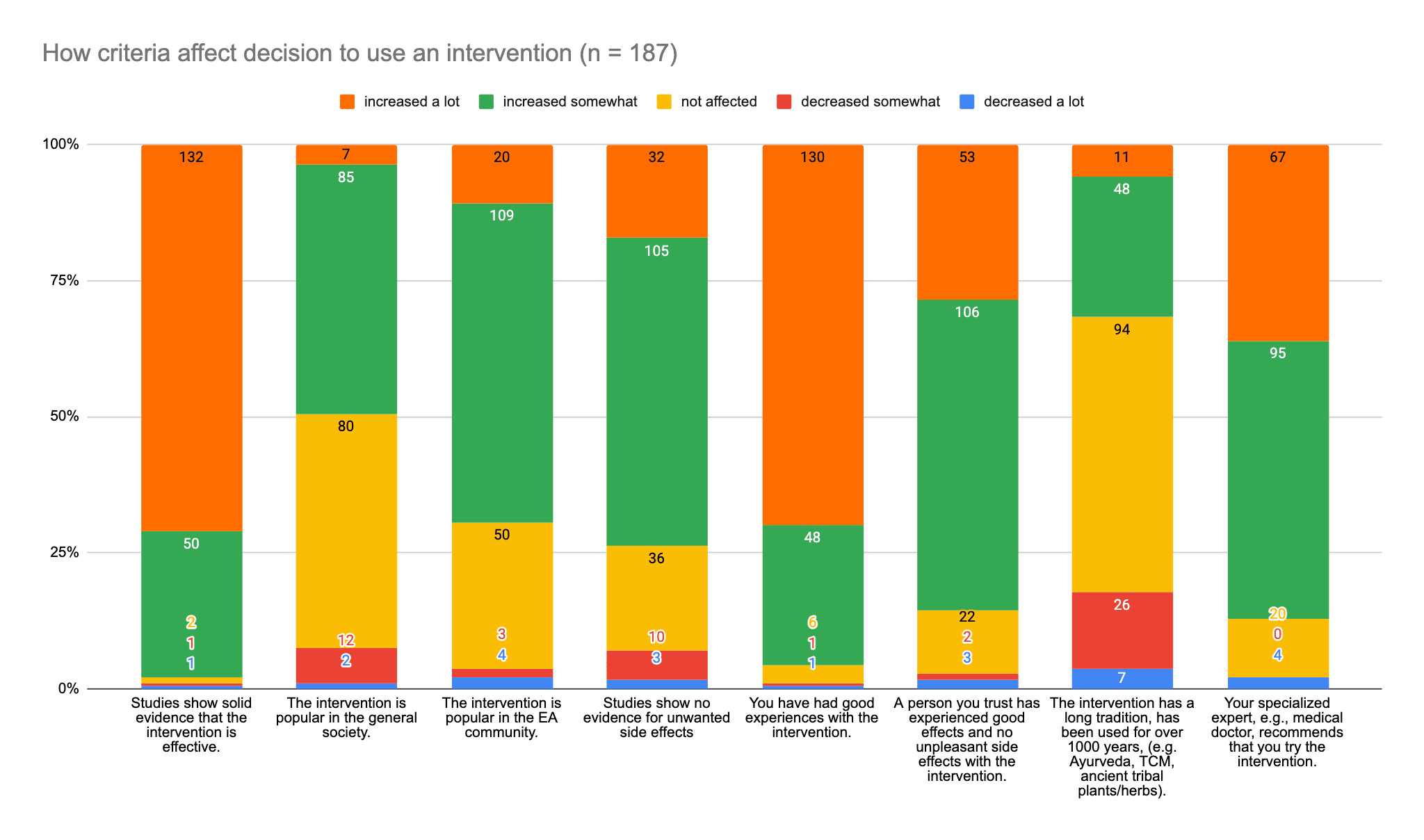
Criteria were as follows, and are provided as column labels from left to right:
The answer was provided by selecting the missing word in the sentence “The likelihood of me using an intervention is ... by this criterion.”
Answer options were:
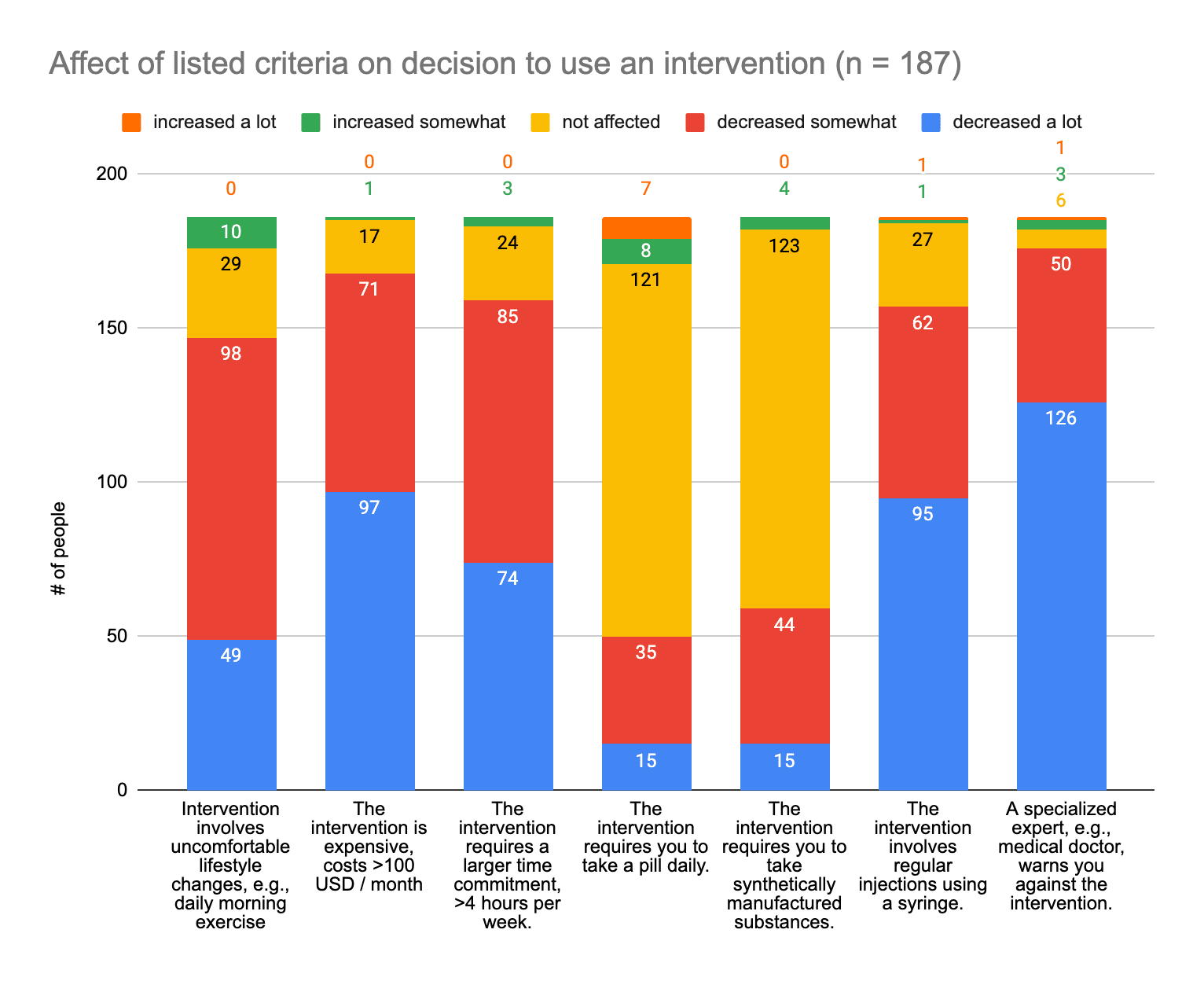
Criteria were as follows, and are provided as column labels from left to right:
Please note: Numbers above the chart are associated with the color groups in the respective columns.
Most people (n = 99) think it would be nice to meet with a therapist, counselor, or coach familiar with Effective Altruism, but that is not something they require to receive mental health support, and for many people it is not necessary at all (n = 74).
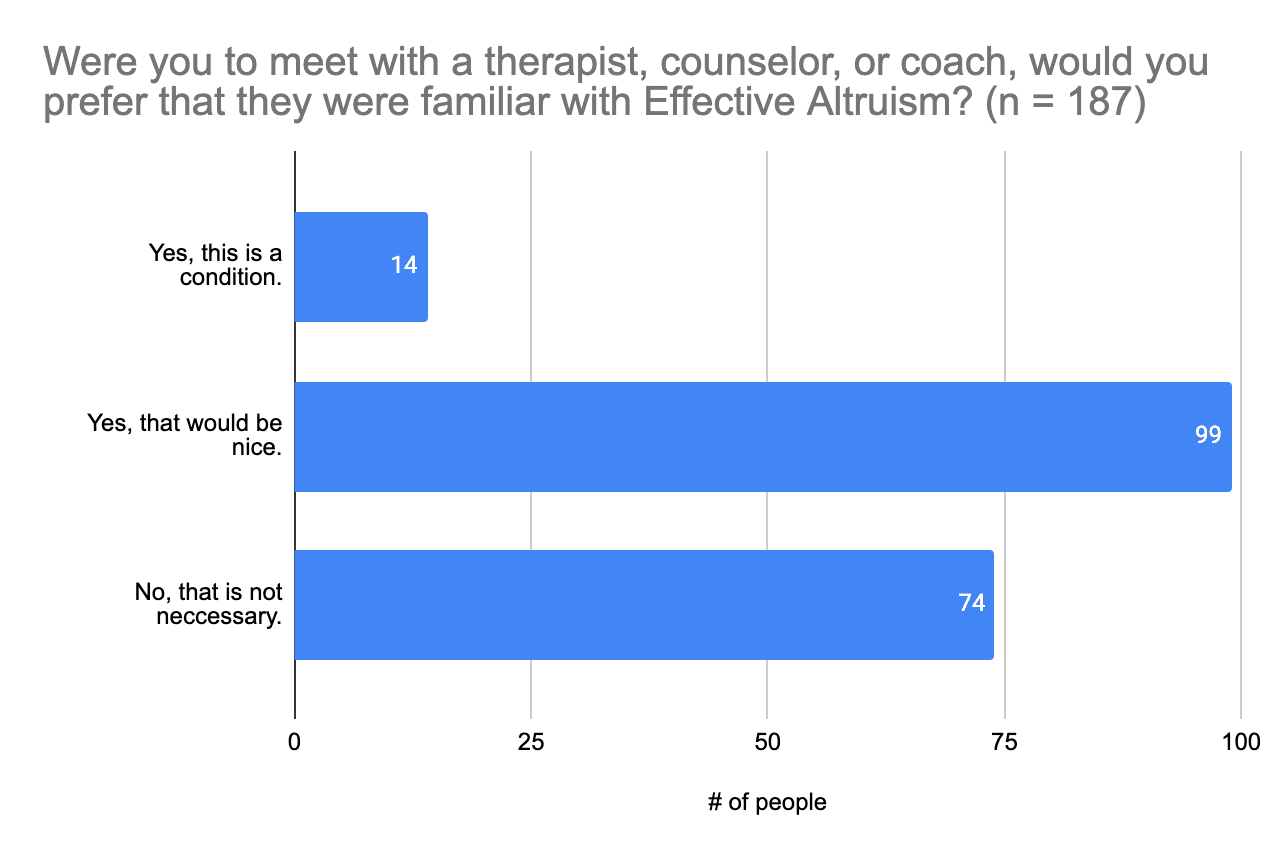
Studies that show solid evidence that an intervention is effective and good experiences with an intervention are the two factors that have a lot of influence over 50% of survey participants’ decisions to use a given intervention. For more than half of participants, decisions were somewhat affected by the popularity of the intervention (n = 109; 58%), studies showing no evidence of unwanted side effects (n = 105; 56%), a person they know having good experiences and no bad experiences with the intervention (n = 106; 57%), and a specialized professional, such as a medical doctor, recommending the intervention (n = 95; 51%). Survey participants are less likely or far less likely to use an intervention if a specialized professional warns them against it (n = 176; 94%), it involves regular injections (n = 157; 84%), it requires a larger time commitment (i.e., >4 hours per week) (n = 159; 85%), it’s expensive (> $100 (USD) each month) (n = 168; 90%), or it involves uncomfortable lifestyle changes (n = 147; 77%). So interventions ideally need to be certified by professionals, involve little commitment in terms of time and money, and not have large effects on people’s lifestyles. And for the majority of survey participants (n = 173; 93%), they do not necessarily need to be provided by therapists, counselors, or coaches familiar with Effective Altruism.
Members of the Effective Altruism community who participated in this survey are generally satisfied with their lives (70%) and the level of support they receive (63%), but they could do with and are open to trying a range of interventions that could help them improve their mental health and productivity, especially as it concerns anxiety, depression, and ADHD; improving one’s concentration, attention, focus, and productivity; and overcoming procrastination. Furthermore, there appears to be a need for help with mental health routines, priorities and structure, and help with learning to communicate what one is feeling and needs.
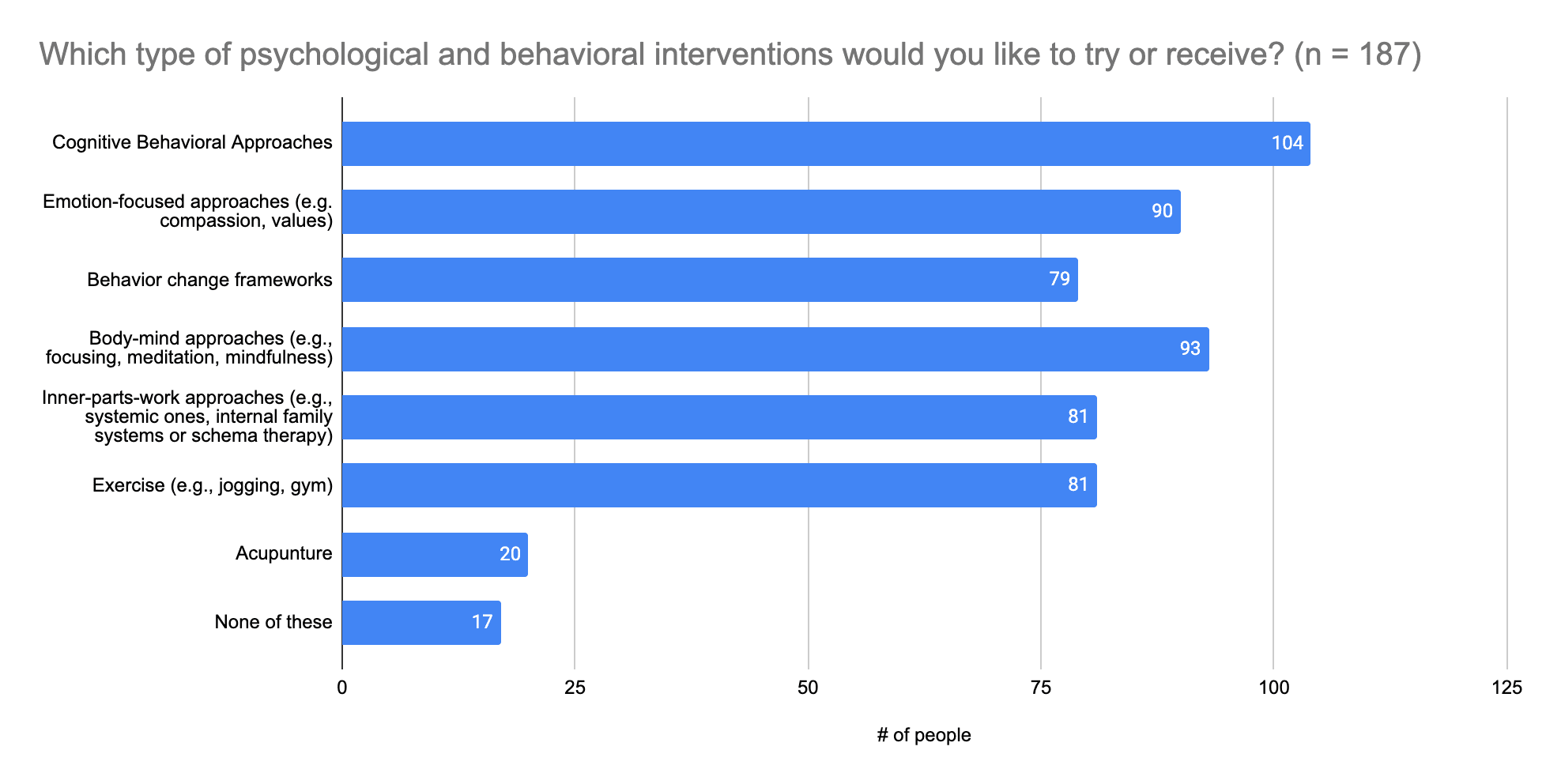
As far as behavioral and psychological interventions are concerned, there’s interest in trying to learning more about cognitive behavioral approaches, emotion-focused approaches (e.g., compassion, values), behavior change frameworks, body-mind approaches (e.g., focusing, meditation, mindfulness), inner-parts-work approaches (e.g., systemic approaches, internal family systems or schema therapy), and exercise. As it pertains to substances, people are generally interested in trying psychedelics, stimulants, vitamins and nutrient supplements, mental health / brain supplements.
A lot of other interesting ideas and suggestions were made via the free-form responses in this survey as well, so please do take a look at those if you are looking for inspiration.
These survey results are likely limited by selection bias. It is likely that more people who are struggling with mental health than those who are not have taken part in this survey. For this reason, this survey does not allow us to make statements about how prevalent things are in the community but only how prevalent they are among those interested in mental health and productivity. This bias was additionally fed by a distribution bias, as this survey, though advertised in common places such as the EA Forum and the large EA Facebook group, was also heavily advertised in EA circles with an interest in mental health and productivity.
A big thank you to everyone who participated in the 2023 EA Mental Health & Productivity Survey! Your answers will help us and others in the community provide mental health resources and information on resources more suited to your needs and interests.
Emily Jennings (Mental Health Navigator), Inga Grossmann (Rethink Wellbeing), and Tim Farkas designed this survey in December 2022. Tim Farkas and Samuel Nellessen contributed questions concerning productivity and substances, and Tim Farkas provided feedback on the survey design. Emily wrote up the results in May and June 2023, and Inga reviewed the draft and added sources, calculations, and a few reflections.
The anonymized data generated and analyzed (with the exception of responses to open-ended questions) are available upon request to the Mental Health Navigator at [email protected] for those who might wish to do follow-up analyses.
We’d be happy for you to reach out and leave constructive comments and suggestions to make us and readers aware of and discuss:
If you feel more comfortable sending your suggestions or comments by email, feel free to send them to the Mental Health Navigator at [email protected].
We might add to the report or update for a more polished version later on. If you’d like to support this effort or help run the next EA Mental Health and Productivity Survey, please let us know via [email protected].
Please note that we do not encourage the use of anything illegal.
Thanks for putting this together!
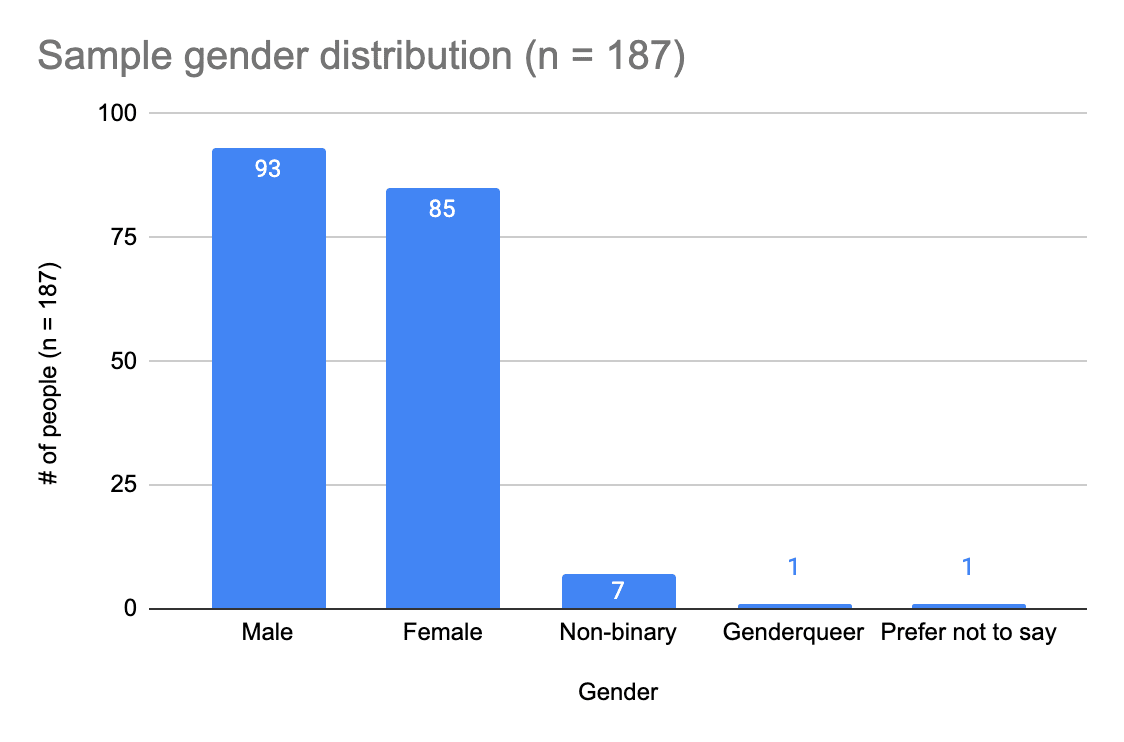
At a glance, it looks like this broadly matched the demographics of the broader EA Survey, except for gender (women were dramatically over-represented in the mental health survey) and engagement (people who took the mental health survey were much more highly engaged).
I agree with you that this survey will also very likely select for people with more of an interest in mental health and perhaps suffering from mental health issues. I imagine this might explain the relatively low life satisfaction you found: